
What is the evidence for mass screening of asymptomatic HCWs?
Download full summary of evidence (pdf)
The following information resources have been selected by the National Health Library and Knowledge Service Evidence Virtual Team in response to your question. The resources are listed in our estimated order of relevance to practicing healthcare professionals confronted with this scenario in an Irish context. In respect of the evolving global situation and rapidly changing evidence base, it is advised to use hyperlinked sources in this document to ensure that the information you are disseminating to the public or applying in clinical practice is the most current, valid and accurate. For further information on the methodology used in the compilation of this document ¾ including a complete list of sources consulted ¾ please see our National Health Library and Knowledge Service Summary of Evidence Protocol.
In A Nutshell
Treibel et al5 state that RNA testing to prevalent infection is a key part of the exit strategy, but the role of testing for asymptomatic infection remains unclear. Understanding the determinants of asymptomatic or pauci-symptomatic infection will provide new opportunities for personalised risk stratification and reveal much-needed correlates of protective immunity, whether induced by vaccination or natural exposure. The authors suggest that the rate of asymptomatic infection among HCWs more probably reflects general community transmission than in-hospital exposure. Prospective patients should be reassured that as the overall epidemic wave recedes, asymptomatic infection among HCWs is low and may not be a major source of transmission. The authors conclude that study data reinforce the importance of epidemic multi-timepoint surveillance of HCWs. The data also suggest that a testing strategy should link population-representative epidemiological surveillance to predict prevalence with adaptive testing for symptomatic individuals at times of low prevalence and rapidly expanding to include asymptomatic HCWs during possible new infection waves.
Black et al10 put forward the case for mass testing of both symptomatic and asymptomatic HCWs to: 1. mitigate workforce depletion by unnecessary quarantine; 2. reduce spread in atypical, mild or asymptomatic cases; and 3. protect the healthcare workforce. HCW testing could reduce in-hospital transmission. In a retrospective, single-centre study in Wuhan, 41% of 138 patients were thought to have acquired infection in hospital. The scale of this problem is not yet fully understood; nor is the full potential for asymptomatic and presymptomatic HCWs to transmit infection to patients who do not have COVID-19, other HCWs or the public. However, given that asymptomatic transmission has been documented, utmost caution is urged.
West et al6 focus on the problem of false-negative tests and argue that for HCWs in endemic areas, return to work after negative testing may need to be delayed until more sensitive tests can be administered and repeat testing is negative.
Two American Universities8, 9 are currently conducting research on testing asymptomatic HCWs. The objective of the research from the University of Colorado is to enact an early warning system in long-term care facilities which would permit temporarily removing asymptomatic but COVID-19 positive caregivers from the workforce until they are no longer virus shedding. The School of Public Health at the University of Minnesota is researching how common asymptomatic carriage of the COVID-19 virus is among HCWs.
IRISH AND INTERNATIONAL GUIDANCE
What does the HIQA say?
Of the studies on pre-symptomatic transmission, 6 out of 11 were based on transmission through families, 2 through the workplace, 1 through a social gathering and 1 in a hospital setting between a visitor and a patient. In Wei et al[ii], of the 7 COVID-19 epidemiologic clusters included, 3 were household clusters, 2 were between friends, 1 was due to proximity in a church and 1 appeared to be environmental contamination in a church. All 5 studies reporting on asymptomatic transmission involved transmission of COVID-19 between family members.
[i] HIQA (21 April 2020) Evidence summary for asymptomatic transmission of COVID-19 https://www.hiqa.ie/sites/default/files/2020-04/Evidence-summary-for-asymptomatic-transmission-of-COVID-19.pdf [Accessed 13 May 2020]
[ii] Wei WE, Li Z, Chiew CJ, Yong SE, Toh MP, Lee VJ. Presymptomatic Transmission of SARS-CoV-2 – Singapore, January 23-March 16, 2020. MMWR Morb Mortal Wkly Rep. 2020;69(14):411‐415. Published 2020 Apr 10. doi:10.15585/mmwr.mm6914e1.
INTERNATIONAL LITERATURE
What does the international literature say?
Black et al (2020) COVID-19: the case for health-care worker screening to prevent hospital transmission[i]
Here we outline the case for mass testing of both symptomatic and asymptomatic health-care workers to: 1. mitigate workforce depletion by unnecessary quarantine; 2. reduce spread in atypical, mild or asymptomatic cases; and 3. protect the healthcare workforce.
HCW testing could reduce in-hospital transmission. In a retrospective, single-centre study in Wuhan, 41% of 138 patients were thought to have acquired infection in hospital. The scale of this problem is not yet fully understood, nor is the full potential for asymptomatic and presymptomatic HCWs to transmit infection to patients who do not have COVID-19, other HCWs or the public. However, given that asymptomatic transmission has been documented, utmost caution is urged.
Rivett et al (2020) Screening of Healthcare Workers for SARS-CoV-2 Highlights the Role of Asymptomatic Carriage in COVID-19 Transmission[ii]
Significant differences
exist in the availability of healthcare worker SARS-CoV-2 testing between
countries, and existing programmes focus on screening symptomatic rather than
asymptomatic staff. Over a 3-week period in April 2020, 1,032 asymptomatic HCWs
were screened for SARS-CoV-2 in a large UK hospital. Symptomatic staff and
symptomatic household contacts were additionally tested. Real-time PCR was used
to detect viral RNA from a throat and nose self-swab. 3% of HCWs in the asymptomatic screening group tested
positive for SARS-CoV-2. 17/30 [57%] were truly asymptomatic/pauci-symptomatic.
12/30 [40%] had experienced symptoms compatible with COVID-19 >7 days prior
to testing, most self-isolating, returning well. Clusters of HCW infection were
discovered on two independent wards. Viral genome sequencing showed that the
majority of HCWs had the dominant lineage B∙1. Our data demonstrates the
utility of comprehensive screening of HCWs with minimal or no symptoms which
will be of critical importance in protecting patients and hospital staff.
RNA testing to prevalent infection is a key part of the exit strategy, but the role of testing for asymptomatic infection remains unclear. Understanding the determinants of asymptomatic or pauci-symptomatic infection will provide new opportunities for personalised risk stratification and reveal much-needed correlates of protective immunity, whether induced by vaccination or natural exposure. We set up COVIDsortium [NCT04318314], a bioresource focusing on asymptomatic healthcare workers at Barts Health NHS Trust, London, to collect data through 16 weekly assessments with a health questionnaire, nasal swab and blood samples; and a further two concluding assessments at 6 and 12 months. HCWs were self-declared as healthy and fit to work for study visits. Participants were not given swab results and those with symptoms or in self-isolation resumed study visits on return to work.
The number and percentage of asymptomatic HCWs who tested positive for SARS-CoV-2 on consecutive weeks from March 23, 2020: 28 [7·1%; 95% CI 4·9–10·0] of 396 HCWs in week 1; 14 [4·9%; 3·0–8·1] of 284 HCWs in week 2; 4 [1·5%; 0·6–3·8] of 263 HCWs in week 3; 4 [1·5%; 0·6–3·8] of 267 HCWs in week 4; and 3 [1·1%, 0·4–3·2] of 269 HCWs in week 5 [figure]. 7 HCWs tested positive on two consecutive timepoints, and 1 HCW tested positive on three consecutive timepoints. During this time, 50 HCWs ¾ not necessarily those who were SARS-CoV-2 positive ¾ self-isolated for symptoms. Of the 44 HCWs who tested positive for SARS-CoV-2, 12 [27%] had no symptoms in the week before or after positivity.
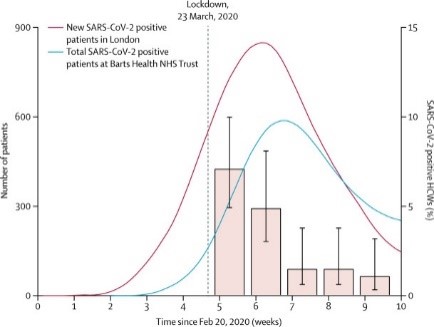
Testing of HCWs has so far been restricted to symptomatic individuals, and no studies have reported serial testing in high-exposure asymptomatic volunteers. If our results are generalisable to the wider HCW population, then asymptomatic infection rates among HCWs tracked the London general population infection curve, peaking at 7·1% and falling six-fold over 4 weeks, despite the persistence of a high burden of COVID-19 patients through this time [representing most inpatients]. Taken together, these data suggest that the rate of asymptomatic infection among HCWs more probably reflects general community transmission than in-hospital exposure. Prospective patients should be reassured that as the overall epidemic wave recedes, asymptomatic infection among HCWs is low and may not be a major source of transmission.
These data reinforce the importance of epidemic multi-timepoint surveillance of HCWs. The data also suggest that a testing strategy should link population-representative epidemiological surveillance to predict prevalence with adaptive testing for symptomatic individuals at times of low prevalence and rapidly expanding to include asymptomatic HCWs during possible new infection waves.
West et al (2020) COVID-19 Testing: The Threat of False-Negative Results[iv]
As tests become more available, observing principles of evidence-based clinical reasoning concerning the meaning of diagnostic test results is
essential. For negative test results in particular, failure to do so has direct implications for the safety of the public and health care workers and for the success of efforts to curb the pandemic. Specifically, anticipation of a less-visible second wave of infection from individuals with false-negative test results is needed.
OTHER SOURCES
Devlin (2020) [News Article] “Healthcare Workers Should Be Screened for COVID-19 Every Week”[v]
Healthcare workers should be screened
for COVID-19 every week to protect patients from asymptomatic infection, the
head of the Francis Crick Institute’s testing facility has said. The call comes
amid concerns that hospitals are becoming hotspots for disease transmission and
evidence that a significant fraction of those infected show few or no symptoms.
The Institute is next week launching a pilot to screen staff at University
College Hospital to identify asymptomatic COVID-19 cases, but the approach has
not been explicitly endorsed by the government and there have been no
indications that this is being considered as a national strategy.
Over the last two months, a lab run by Greg Ebel, Professor in the Department of Microbiology, Immunology and Pathology, tested samples from 462 healthcare workers in Colorado to determine if workers without symptoms were silently carrying the virus. The tests identified 57 people who tested positive for COVID-19 but had no symptoms. The purpose of the research, Ehrhart explained, is to enact an early warning system in long-term care facilities that would permit temporarily removing asymptomatic but COVID-19 positive caregivers from the workforce until they are no longer virus shedding.
A new School of Public Health study will test 500 health workers without symptoms of COVID-19 to see what proportion of them are actually infected with SARS-CoV-2, the virus that causes the illness. “The study will reveal how common asymptomatic carriage of the COVID-19 virus is among health care workers,” says Demmer. “The findings can help health care leaders improve policies and procedures to keep health care workers and patients safe.”
[i] Black JRM, Bailey C, Przewrocka J, Dijkstra KK, Swanton C. COVID-19: the case for health-care worker screening to prevent hospital transmission [published correction appears in Lancet. 2020 Apr 17;:]. Lancet. 2020;395(10234):1418‐1420. doi:10.1016/S0140-6736(20)30917-X
[ii] Rivett L, Sridhar S, Sparkes D, et al. Screening of healthcare workers for SARS-CoV-2 highlights the role of asymptomatic carriage in COVID-19 transmission [published online ahead of print, 2020 May 11]. Elife. 2020;9:e58728. doi:10.7554/eLife.58728
[iii] Treibel TA, Manisty C, Burton M, et al. COVID-19: PCR screening of asymptomatic health-care workers at London hospital [published online ahead of print, 2020 May 8]. Lancet. 2020;S0140-6736(20)31100-4. doi:10.1016/S0140-6736(20)31100-]
[iv] West CP, Montori VM, Sampathkumar P. COVID-19 Testing: The Threat of False-Negative Results [published online ahead of print, 2020 Apr 11]. Mayo Clin Proc. 2020;S0025-6196(20)30365-7. doi:10.1016/j.mayocp.2020.04.004
[v] Devlin, Hannah. “Healthcare Workers ‘Should Be Screened for COVID-19 Every Week’.” The Guardian 2020-04-16 2020. https://www.theguardian.com/world/2020/apr/16/healthcare-workers-screened-COVID-19-every-week-infectious-unethical [Accessed 13 May 2020]
[vi] Gulden, Mary. “Minimizing Transmission: Testing Asymptomatic Healthcare Workers to Find Silent COVID-19 Carriers.” Colorado State University College news. 2020-04-27 2020. https://source.colostate.edu/minimizing-transmission-testing-asymptomatic-healthcare-workers-to-find-silent-COVID-19-carriers/ [Accessed 13 May 2020]
[vii] Plain, Charlie “Study to Identify How Common COVID-19 Virus Is among Health Care Workers without Symptoms – School of Public Health” University of Minnesota.” (2020). https://www.sph.umn.edu/news/study-to-identify-how-common-COVID-19-virus-is-among-health-care-workers-without-symptoms/ [Accessed 13 May 2020]
Produced by the members of the National Health Library and Knowledge Service Evidence Team†. Current as at 13 May 2020. This evidence summary collates the best available evidence at the time of writing and does not replace clinical judgement or guidance. Emerging literature or subsequent developments in respect of COVID-19 may require amendment to the information or sources listed in the document. Although all reasonable care has been taken in the compilation of content, the National Health Library and Knowledge Service Evidence Team makes no representations or warranties expressed or implied as to the accuracy or suitability of the information or sources listed in the document. This evidence summary is the property of the National Health Library and Knowledge Service and subsequent re-use or distribution in whole or in part should include acknowledgement of the service.
Isabelle Delaunois, Medical Librarian, University of Limerick [Author]; Brendan Leen, Regional Librarian, HSE South, St. Luke’s General Hospital, Kilkenny

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.