
What seroprevalence studies have been completed in other countries – general population studies and also studies on specific population subgroups such as health workers, hospitalized patients, blood donors and children?
Download Full Summary of Evidence (pdf)
The following information resources have been selected by the National Health Library and Knowledge Service Evidence Virtual Team in response to your question. The resources are listed in our estimated order of relevance to practicing healthcare professionals confronted with this scenario in an Irish context. In respect of the evolving global situation and rapidly changing evidence base, it is advised to use hyperlinked sources in this document to ensure that the information you are disseminating to the public or applying in clinical practice is the most current, valid and accurate. For further information on the methodology used in the compilation of this document including a complete list of sources consulted please see our National Health Library and Knowledge Service Summary of Evidence Protocol.
TABLE OF CONTENTS
In a nutshell
Serological tests detect antibodies to SARS-CoV-2 in the blood, and those that have been adequately validated can help identify patients who have had the virus6.The World Health Organization (WHO) states that most studies they have examined show that people who have recovered from the SARS-CoV-2 infection have antibodies to the virus. It also reports that it is unknown whether the presence of antibodies to SARS-CoV-2 confers immunity to subsequent infection by the virus in humans1. The Centers for Disease Control and Prevention (CDC) concur4. WHO cautions against so-called ‘immunity passports’ as this may lead to those previously infected not following public health advice1.
The WHO have created a protocol to investigate the extent of SARS-CoV-2 infection as determined by seropositivity in the general population2. It cautions that each country may need to tailor some aspects of this protocol to align with public health, laboratory and clinical systems, according to capacity, availability of resources and cultural appropriateness. Similarly, the European Commission has published guidance on current performance of COVID-19 test methods and devices and proposed performance criteria with the most critical performance parameters being diagnostic sensitivity and specificity3. The CDC is evaluating the performance of commercially manufactured antibody tests tests in collaboration with the other federal organisations. CDC’s serologic test is designed to detect antibodies produced in response to SARS-CoV-2 and to avoid detection of antibodies against other common coronaviruses that cause less severe illnesses, such as colds4.
It is important to choose the correct serological test and this is discussed extensively throughout the document 2, 3 , 4, 6, 7 , 9 , 1 0, 11.
There are a wide range of seroprevalence studies with defined populations from various cities and countries that have taken place and there are many examples included throughout this evidence summary. A key objective of such studies is to find out what%age of the population has been exposed to the virus already. According to one study, the herd immunity threshold for SARS-CoV-2 is estimated at 50 to 67%21. Looking at the national, regional and city tests that have provided results it seems clear that no place studied is near this%age yet. For instance, just 5% of the Spanish population has been infected and has developed antibodies29. A study estimated the seroprevalence in the Netherlands at just 2.7%21. Some cities that have been hit hard by the virus appear to have a higher%age of their population that have been previously infected. New York has reported that around 21% of the city has SARS-CoV-2 antibodies37 while London’s figure has been calculated at approximately 17% 33.
Serological tests of healthcare workers to ascertain if they have been infected is an important question and articles concerning this topic are included in the document12, 13, 14, 15. Studies that examine serological testing of blood donors are also considered16, E, 19, 20, 23.
IRISH AND INTERNATIONAL GUIDANCE
What does the World Health Organization say?
‘Immunity passports’ in the context of COVID-19 – Scientific Brief [i]
Measurement of Antibodies Specific to COVID-19
WHO continues to review the evidence on antibody responses to SARS-CoV-2 infection. Most of these studies show that people who have recovered from infection have antibodies to the virus. However, some of these people have very low levels of neutralizing antibodies in their blood, suggesting that cellular immunity may also be critical for recovery. As of 24 April 2020, no study has evaluated whether the presence of antibodies to SARS-CoV-2 confers immunity to subsequent infection by this virus in humans.
At this point in the pandemic, there is not enough evidence about the effectiveness of antibody-mediated immunity to guarantee the accuracy of an ‘immunity passport’ or ‘risk-free certificate.’ People who assume that they are immune to a second infection because they have received a positive test result may ignore public health advice. The use of such certificates may therefore increase the risks of continued transmission.
The following protocol has been designed to investigate the extent of infection, as determined by seropositivity in the general population in any country in which COVID-19 virus infection has been reported. Each country may need to tailor some aspects of this protocol to align with public health, laboratory and clinical systems according to capacity, availability of resources and cultural appropriateness. However, using a standardized protocol such as this one below, epidemiological exposure data and biological samples can be systematically collected and shared rapidly in a format that can be easily aggregated, tabulated and analyzed across many different settings globally for timely estimates of COVID-19 virus infection severity and attack rates, as well as to inform public health responses and policy decisions. This is particularly important in the context of a novel respiratory pathogen, such as COVID-19 virus.
What does the European Centre for Disease Prevention and Control say?
Coronavirus disease 2019 (COVID-19) in the EU/EEA and the UK– ninth update (23 April 2020)[iii]
Testing Population Immunity
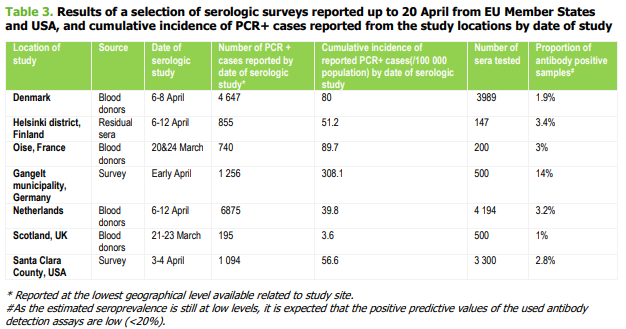
Population-based seroepidemiological studies have been started in some EU/EEA Member States. Preliminary results from Denmark, Finland, France, Netherlands, Scotland and the US show that 1-3.4% of healthy adult blood donors ¾ patients examined for other diseases than infectious diseases or population based on convenience sample ¾ had antibodies against SARS-CoV-2 virus in the period 20 March-12 April. In Gangelt municipality, Germany, in a household study in a highly-affected area, the proportion of positive specimens was 14% in early April. In addition, in Denmark, in the capital area, the preliminary results of an antibody screening by a rapid test of healthcare employees showed that infection among health professionals is at 4.1%. These estimates provide a consistent picture, suggesting significant underreporting, under-ascertainment, or asymptomatic infection across multiple locations in Europe and North America. Many uncertainties and sources of bias remain in interpreting these preliminary results. Clinically validated laboratory assays for detection of antibodies are still largely lacking and therefore these results need to be interpreted with caution. In addition, specimens from blood donors are from healthy adults, and will necessarily exclude people with symptomatic respiratory or febrile illness. With levels of prevalence in the range of 2-3%, the expected positive predictive value of such test is in the range of 20%, therefore the reported proportions are to be seen as significant overestimates of population prevalence.
Test Validation
The European Commission has published guidance on current performance of COVID-19 test methods and devices and proposed performance criteria with the most critical performance parameters being diagnostic sensitivity and specificity. Diagnostic sensitivity and specificity of rapid tests and serological assays for COVID-19 in well-designed clinical trials is still missing and essential to perform before introducing them into the routine as a standalone test. In addition, it is important to be vigilant about fraudulent commercial claims of test performance, as communicated by WHO in a Medical Product Alert on 31 March 2020 in relation to reports of falsified in vitro diagnostics (IVDs) and laboratory reagents for the detection of SARS-CoV-2. ECDC is working closely with the European Commission, Member State authorities and national laboratories, FIND and WHO to help monitor the ongoing validation of these rapid tests.
What do the Centers for Disease Control and Prevention (United States) say?
Serology Testing for COVID-19 at CDC [iv]
CDC has developed a laboratory blood test to assist with efforts to determine how much of the US population has been infected with SARS-CoV-2, the virus that causes COVID-19. CDC is also using its serologic test to evaluate the performance of commercial antibody tests.
An antibody test looks for the presence of antibodies which are specific proteins made in response to infections. Antibodies can be found in the blood of people who are tested after infection and show that people have had an immune response to the infection. Antibody test results are especially important for detecting previous infections with few or no symptoms.
However, we do not know if the antibodies that result from SARS-CoV-2 infection will provide someone with immunity from a future infection. If antibodies do provide immunity, we don’t know what titer or amount of antibodies would be protective or the duration that protection would last. CDC scientists are conducting studies to better understand the level of antibodies needed for protection, the duration of that protection, and the factors associated with whether a person develops a protective antibody response.
Commercially manufactured antibody tests check for SARS-CoV-2 antibodies in individuals and are available through healthcare providers and commercial laboratories. CDC is evaluating the performance of these tests in collaboration with the following federal organizations:
- Biomedical Research and Development Authority
- U.S. Food and Drug Administration (FDA)
- National Institutes of Health
- Department of Defense
- White House Office of Science and Technology Policy
Results from the initial federal evaluation are expected in May and will be updated as more tests are evaluated.
Antibody tests designed to provide results to individuals or healthcare providers can show whether someone was previously infected with SARS-CoV-2. However, these tests have limitations. Specificity [doesn’t detect non-target viruses] and sensitivity [true positive rate] of antibody tests vary.
CDC’s serologic test is based on a set of serologic tests that CDC developed and optimized to detect SARS-CoV-2 antibodies in serum, which is a component of blood. These tests use live virus and a specific SARS-CoV-2 protein, the spike antigen, designed and produced by the Vaccine Research Center at the National Institutes of Health.
CDC’s serologic test is designed to detect antibodies produced in response to SARS-CoV-2 and to avoid detection of antibodies against other common coronaviruses that cause less severe illnesses, such as colds.
CDC’s test has a specificity of greater than 99% and a sensitivity of 96% based on initial tests. It can be used to identify past SARS-CoV-2 infection in people who were infected at least 1 to 3 weeks previously.
POINT-OF-CARE TOOLS
What does BMJ Best Practice say?
Coronavirus disease 2019 (COVID-19)[v]
Serological Testing
Serological testing is becoming increasingly available for use; however, while rapid antibody detection kits have been approved in Europe and the US for the qualitative detection of SARS-CoV-2 immunoglobulin G (IgG)/IgM antibodies in serum, plasma, or whole blood, the World Health Organization does not recommend the use of these tests outside of research settings as they have not been validated as yet. Antibody responses to SARS-CoV-2 typically occur during the first 3 weeks of illness, with the seroconversion time of IgG antibodies often being earlier than that of IgM antibodies. Serum samples can be stored to retrospectively define cases when validated serology tests become available.
What does UpToDate say?
Serology to Identify Prior Infection
Serologic tests detect antibodies to SARS-CoV-2 in the blood, and those that have been adequately validated can help identify patients who have had COVID-19. Serologic tests may also be able to identify some patients with current infection, particularly those who present late in the course of illness, but they are less likely to be reactive in the first several days to weeks of infection and thus may have less utility for diagnosis in the acute setting. Additionally, individual results should be interpreted with caution in settings of low seroprevalence, in which even serologic tests that have high specificity still have a low positive predictive value: ie a positive test may be as likely to reflect a false positive as a true positive.
In the United States, several serologic tests have been granted emergency use authorization by the FDA for use by laboratories certified to perform moderate- and high-complexity tests. The FDA highlights that serologic tests should not be used as the sole test to diagnose or exclude active SARS-CoV-2 infection. The sensitivity and specificity of many of these serologic tests are uncertain; a catalog of these tests can be found at centerforhealthsecurity.org.
Detectable antibodies generally take several days to weeks to develop. In a study of 173 patients with COVID-19, the median time from symptom onset to antibody detection with an enzyme-linked immunosorbent assay [ELISA] that detects antibodies to the receptor-binding domain of the spike protein was 12 days for IgM and 14 days for IgG In the first week since symptom onset, fewer than 40% had detectable antibodies; by day 15, IgM and IgG were detectable in 94 and 80%, respectively.
The accuracy and time to antibody detection vary with the particular test used. Studies evaluating the specificity of serologic tests in a broad population are lacking; in particular, the rate of cross-reactivity with other coronaviruses is a potential concern, and IgM tests are prone to false-positive results.
Large-scale serologic screening with validated tests may be able to provide a better sense of the scope of the burden of disease by identifying people who were not diagnosed by PCR or who may have had asymptomatic or subclinical infection; and also identify individuals who may have immunity to infection; serologic correlates of protective immunity, however, have not been defined.
Other Tests
- Tests that identify SARS-CoV-2 antigen are under development. Rapid antigen tests are easy to use and can be performed at the point of care, but for respiratory pathogens, they are typically less sensitive than nucleic acid amplification testing. Several manufacturers are selling rapid, point-of-care antigen tests, and in the United States, the FDA has started to issue emergency use authorizations on such tests. Clinicians should be aware of the possibility of false negatives with antigen tests. The WHO had previously cautioned against the use of rapid tests based on antigen testing or antibody detection that have not undergone adequate validation because of concerns regarding false-positive or false-negative results.
- For safety reasons, specimens from a patient with suspected or documented COVID-19 should not be submitted to clinical laboratories for viral culture. Viral culture is mainly reserved for research purposes.
INTERNATIONAL LITERATURE
What does the international literature say?
General Serological Studies
Kontou et al (2020) Antibody Tests in Detecting SARS-CoV-2 Infection: A Meta-Analysis[vii]
The emergence of Coronavirus disease 2019 (COVID-19) caused by SARS-CoV-2 made imperative the need for diagnostic tests that can identify the infection. Although Nucleic Acid Test (NAT) is considered to be the gold standard, serological tests based on antibodies could be very helpful. However, individual studies are usually inconclusive; thus, a comparison of different tests is needed. We performed a systematic review and meta-analysis in PubMed, medRxiv and bioRxiv. We used the bivariate method for meta-analysis of diagnostic tests pooling sensitivities and specificities. We evaluated IgM and IgG tests based on Enzyme-linked immunosorbent assay (ELISA), Chemiluminescence Enzyme Immunoassays (CLIA), Fluorescence Immunoassays (FIA), and the Lateral Flow Immunoassays (LFIA). We identified 38 studies containing data from 7848 individuals. Tests using the S antigen are more sensitive than N antigen-based tests. IgG tests perform better compared to IgM ones and show better sensitivity when the samples were taken longer after the onset of symptoms. Moreover, a combined IgG/IgM test seems to be a better choice in terms of sensitivity than measuring either antibody alone. All methods yield high specificity with ELISA and LFIA reaching levels around 99%. ELISA- and CLIA-based methods perform better in terms of sensitivity [90%-94%] followed by LFIA and FIA with sensitivities ranging from 80% to 89%. ELISA tests could be a safer choice at this stage of the pandemic. LFIA tests are more attractive for large seroprevalence studies but show lower sensitivity, and this should be taken into account when designing and performing seroprevalence studies.
Objective: To estimate the infection fatality rate of coronavirus disease 2019 (COVID-19) from data of seroprevalence studies.
Methods: Population studies with sample size of at least 500 and published as peer-reviewed papers or preprints as of May 12, 2020 were retrieved from PubMed, preprint servers, and communications with experts. Studies on blood donors were included, but studies on healthcare workers were excluded. The studies were assessed for design features and seroprevalence estimates. Infection fatality rate was estimated from each study dividing the number of COVID-19 deaths at a relevant time point by the number of estimated people infected in each relevant region. Correction was also attempted accounting for the types of antibodies assessed.
Results: Twelve studies were identified with usable data to enter into calculations. Seroprevalence estimates ranged from 0.113% to 25.9% and adjusted seroprevalence estimates ranged from 0.309% to 33%. Infection fatality rates ranged from 0.03% to 0.50% and corrected values ranged from 0.02% to 0.40%.
Conclusions: The infection fatality rate of COVID-19 can vary substantially across different locations and this may reflect differences in population age structure and case-mix of infected and deceased patients as well as multiple other factors. Estimates of infection fatality rates inferred from seroprevalence studies tend to be much lower than original speculations made in the early days of the pandemic.
Bryant et al (2020) Serology for SARS-CoV-2: Apprehensions, opportunities, and the path forward[ix]
Serological testing for SARS-CoV-2 has enormous potential to contribute to COVID-19 pandemic response efforts. However, the required performance characteristics of antibody tests will critically depend on the use case ¾ individual-level vs. population-level.
Kadkhoda. (2020) COVID-19 serologic testing: FAQs and caveats[x]
This article investigates the following questions:
- Is IgM/IgA serology reliable for diagnosing acute symptomatic COVID-19?
- Is IgG serology a reliable option for diagnosing acute or convalescent COVID-19?
- Is IgG serology reliable for evaluating infectivity and clinical immunity to reinfection with COVID-19?
- Is IgG serology reliable for screening a COVID-19-convalescent donor?
- Is IgG serology reliable for SARS-CoV-2 serosurveys?
In this study, we aimed to evaluate the diagnostic value of serological assay for SARS-CoV-2. A newly-developed ELISA assay for IgM and IgG antibodies against N protein of SARS-CoV-2 was used to screen the serums of 238 admitted hospital patients between February 6 and February 14, 2020 with confirmed or suspected SARS-CoV-2. SARS-CoV-2 RNA was detected on pharyngeal swab specimens using real time RT-PCR. 194 (81.5%) of the serums were detected to be antibody (IgM and/or IgG) positive, significantly higher than the positive rate of viral RNA (64.3%). There was no difference in the positive rate of antibodies between the confirmed patients (83.0%, 127/153) and the suspected patients (78.8%, 67/85) whose nucleic acid tests were negative. The antibody positive rates were very low in the first five days after initial onset of symptoms, and then rapidly increased as the disease progressed. After 10 days, the antibody positive rates jumped from below 50% to over 80%. However, the positive rates of viral RNA maintained above 60% in the first 11 days after initial onset of symptoms, and then rapidly decreased. Overall, the suspected patients were most likely infected by SARS-CoV-2. Before the eleventh day after initial onset of symptoms, nucleic acid test is key for confirmation of viral infection. The combination of serological assay can greatly improve the diagnostic efficacy. After the 11th day post-disease onset, the diagnosis for viral infection should be majorly dependent on serological assay.
Healthcare Workers
Serial serological screening with a validated technique such as CLIA could provide a significant contribution to IPC in hospitals and LTCFs, considering its lower cost, easier repeatability and sustainability in the medium term, compared to swab-based molecular assays. While serological tests have limited utility in diagnosing individual acute infections, they can inform actions to protect the hospital community. A serum antibody screening approach is indeed already used in surveillance campaigns among HCW for other communicable diseases: eg viral hepatitides.
A possible protocol could include systematic serological testing of all hospital personnel, and subsequent second-line testing with viral RT-PCR to differentiate active cases from past infections. All IgG-negative subjects are then retested every 2-4 weeks according to the local epidemiological context and available resources. In case of seroconversion, a RT-PCR test is warranted. This approach would not substitute the standard, shorter window RT-PCR testing of symptomatic subjects, but would allow easier identification of asymptomatic carriers and guide subsequent contact tracing and testing, with more judicious resource usage compared to a hypothetical universal serial RT-PCR screening
Background: The novel coronavirus SARS-CoV-2 is associated with a severe respiratory manifestation, COVID-19, and presents a challenge for healthcare systems worldwide. Healthcare workers are a vulnerable cohort for SARS-CoV-2 infection due to frequent and close contact to patients with COVID-19.
Study design: Serum samples from 316 healthcare workers of the University Hospital Essen, Germany were tested for SARS-CoV-2-IgG antibodies. A questionnaire was used to collect demographic and clinical data. Healthcare workers were grouped depending on the frequency of contact to COVID-19 patients in high-risk-group (n = 244) with daily contact to known or suspected SARS-CoV-2 positive patients, intermediated-risk-group (n = 37) with daily contact to patients without known or suspected SARS-CoV-2 infection at admission and low-risk-group (n = 35) without patient contact.
Results: In 5 of 316 (1.6%) healthcare workers SARS-CoV-2-IgG antibodies could be detected. The seroprevalence was higher in the intermediate-risk-group vs. high-risk-group (2/37 (5.4%) vs. 3/244 (1.2%), p = 0.13). Four of the five subject were tested negative for SARS-CoV-2 via PCR. One (20%) subject was not tested via PCR since he was asymptomatic.
Conclusion: The overall seroprevalence of SARS-CoV-2 in healthcare workers of a tertiary hospital in Germany is low (1.6%). The data indicate that the local hygiene standard might be effective.
The prevalence of antibodies to SARS-CoV-2 among healthcare personnel is unclear. A recent study noted an unadjusted prevalence of 1.5% of SARS-CoV-2 antibodies using a point of care test in a community surveillance study in Santa Clara, CA. Other community surveillance projects have reported varying rates of COVID-19 antibody seropositivity, and were as high as 32% in an area of Boston considered a hot spot for COVID-19. Healthcare personnel may have a higher risk of exposure to COVID-19 than the general population. In this letter we report the findings of a voluntary program for SARS-CoV-2 antibody testing for faculty and staff at the University of Utah Hospital Emergency Department (ED), an urban, academic emergency department in Salt Lake City, Utah.
A COVID-19 outbreak among staff members of a major German children’s and women’s hospital was followed by massive RT-PCR SARS-CoV-2 tests and provided the opportunity to study symptoms, chains of infection and SARS-CoV-2 specific antibody responses by ELISA. Study participants were classified as COVID-19 cases, and persons with close, moderate or no exposure to SARS-CoV-2 in the clinical setting, respectively.
We found that a significant number of diseased did not develop relevant antibody responses three weeks after symptom onset. Our data also suggests that exposure to COVID-19 positive co-workers in a hospital setting is not leading to the development of measurable immune responses in a significant proportion of asymptomatic contact-persons.
Regional Seroprevalence Studies
Italy: Milan metropolitan area
Objectives: The Milan metropolitan area in Northern Italy was among the most severely hit by the SARS-CoV-2 outbreak. The epidemiological trends of mild COVID-19 are however still unknown. The aim of this study was to examine the seroprevalence of SARS-CoV-2 infection in healthy asymptomatic adults, the risk factors, and laboratory correlates.
Design: We conducted a cross-sectional study during the outbreak. Presence of anti-SARS-CoV-2 IgM/IgG antibodies against the Nucleocapsid protein was assessed by a lateral flow immunoassay. Setting: Blood center at a leading academic hospital serving as COVID-19 referral center. Participants: We considered a random sample of blood donors since the start of the outbreak (February 24th to April 8th 2020, n=789). Main outcome measures: The main outcome was the prevalence of IgG/IgM anti-SARS-CoV-2 antibodies.
Results: The test had a 98.3% specificity and 100% sensitivity, and for IgG was validated in a subset by an independent ELISA against the Spike protein (N=34, P<0.001). At the start of the outbreak, the overall seroprevalence of SARS-CoV-2 was 4.6% (2.3 to 7.9; P<0.0001 vs. 120 historical controls). During the study period characterized by a gradual implementation of social distancing measures, there was a progressive increase in seroprevalence to 7.1% (4.4 to 10.8), due to a rise in IgG+ to 5% (2.8 to 8.2; P=0.004 for trend, adjusted weekly increase 2.7, SE 1.3%), but not of IgM+ (P=NS). At multivariate logistic regression analysis, seroconversion to IgG was more frequent in younger (P=0.043), while recent infections (IgM+) in older individuals (P=0.002). IgM+ was independently associated with higher triglycerides, eosinophils, and lymphocytes (P<0.05).
Conclusions: SARS-CoV-2 infection was already circulating in Milan at the outbreak start. Social distancing may have been more effective in younger individuals, and by the end of April 4.4-10.8% of healthy adults had evidence of seroconversion. Asymptomatic infection may affect lipid profile and blood count.
Denmark
Background: The pandemic due to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has tremendous consequences for our societies. Knowledge of the seroprevalence of SARS-CoV-2 is needed to accurately monitor the spread of the epidemic and also to calculate the infection fatality rate (IFR). These measures may help the authorities to make informed decisions and adjust the current societal interventions. Blood donors comprise approximately 4.7% of the similarly aged population of Denmark and blood is donated in all areas of the country. The objective of this study was to perform real-time seroprevalence surveying among blood donors as a tool to estimate previous SARS-CoV-2 infections and the population based IFR. Methods: All Danish blood donors aged 17-69 years giving blood April 6 to 17 were tested for SARS-CoV-2 immunoglobulin M and G antibodies using a commercial lateral flow test. Antibody status was compared between areas and an estimate of the IFR was calculated. The seroprevalence was adjusted for assay sensitivity and specificity taking the uncertainties of the test validation into account when reporting the 95% confidence intervals (CI).
Results: The first 9,496 blood donors were tested and a combined adjusted seroprevalence of 1.7% (CI: 0.9-2.3) was calculated. The seroprevalence differed across areas. Using available data on fatalities and population numbers a combined IFR in patients younger than 70 is estimated at 82 per 100,000 (CI: 59-154) infections.
Conclusions: The IFR was estimated to be slightly lower than previously reported from other countries not using seroprevalence data. The IFR, including only individuals with no comorbidity, is likely several fold lower than the current estimate. This may have implications for risk mitigation. We have initiated real-time nationwide anti-SARS-CoV-2 seroprevalence surveying of blood donations as a tool in monitoring the epidemic.
Switzerland: Geneva
Background: Assessing the burden of COVID-19 based on medically-attended case counts is suboptimal given its reliance on testing strategy, changing case definitions and the wide spectrum of disease presentation. Population-based serosurveys provide one avenue for estimating infection rates and monitoring the progression of the epidemic, overcoming many of these limitations.
Methods: Taking advantage of a pool of adult participants from population-representative surveys conducted in Geneva, Switzerland, we implemented a study consisting of 8 weekly serosurveys among these participants and their household members older than 5 years. We tested each participant for anti-SARS-CoV-2-IgG antibodies using a commercially available enzyme-linked immunosorbent assay [Euroimmun AG, Lubeck, Germany]. We estimated seroprevalence using a Bayesian regression model taking into account test performance and adjusting for the age and sex of Geneva’s population. Results: In the first three weeks, we enrolled 1335 participants coming from 633 households, with 16% <20 years of age and 53.6% female, a distribution similar to that of Geneva. In the first week, we estimated a seroprevalence of 3.1% (95% CI 0.2-5.99, n=343). This increased to 6.1% (95% CI 2.6-9.33, n=416) in the second, and to 9.7% (95% CI 6.1-13.11, n=576) in the third week. We found that 5-19 year-olds (6.0%, 95% CI 2.3-10.2%) had similar seroprevalence to 20-49 year olds (8.5%, 95% CI 4.99-11.7), while significantly lower seroprevalence was observed among those 50 and older (3.7%, 95% CI 0.99-6.0, p=0.0008).
Interpretation: Assuming that the presence of IgG antibodies is at least in the short-term associated with immunity, these results highlight that the epidemic is far from burning out simply due to herd immunity. Further, no differences in seroprevalence between children and middle age adults are observed. These results must be considered as Switzerland and the world look towards easing restrictions aimed at curbing transmission.
France: Oise Department
Background: The Oise department in France has been heavily affected by COVID-19 in early 2020. Methods: Between 30 March and 4 April 2020, we conducted a retrospective closed cohort study among pupils, their parents and siblings, as well as teachers and non-teaching staff of a high-school located in Oise. Participants completed a questionnaire that covered history of fever and/or respiratory symptoms since 13 January 2020 and had blood tested for the presence of anti-SARS-CoV-2 antibodies. The infection attack rate (IAR) was defined as the proportion of participants with confirmed SARS-CoV-2 infection based on antibody detection. Blood samples from two blood donor centres collected between 23 and 27 March 2020 in the Oise department were also tested for presence of anti-SARS-CoV-2 antibodies.
Findings: Of the 661 participants [median age: 37 years], 171 participants had anti-SARS-CoV-2 antibodies. The overall IAR was 25.9% (95% confidence interval (CI) = 22.6-29.4), and the infection fatality rate was 0% (one-sided 97.5% CI = 0-2.1). Nine of the ten participants hospitalised since mid-January were in the infected group, giving a hospitalisation rate of 5.3% (95% CI = 2.4-9.8). Anosmia and ageusia had high positive predictive values for SARS-CoV-2 infection (84.7% and 88.1%, respectively). Smokers had a lower IAR compared to non-smokers (7.2% versus 28.0%, P <0.001). The proportion of infected individuals who had no symptoms during the study period was 17.0% (95% CI = 11.2-23.4). The proportion of donors with anti-SARS-CoV-2 antibodies in two nearby blood banks of the Oise department was 3.0% (95% CI = 1.1-6.4). Interpretation: The relatively low IAR observed in an area where SARS-CoV-2 actively circulated weeks before confinement measures indicates that establishing herd immunity will take time, and that lifting these measures in France will be long and complex.
France [3 separate sample populations]
It is of paramount importance to evaluate the prevalence of both asymptomatic and symptomatic cases of SARS-CoV-2 infection and their antibody response profile. Here, we performed a pilot study to assess the levels of anti-SARS-CoV-2 antibodies in samples taken from 491 pre- epidemic individuals, 51 patients from Hopital Bichat (Paris), 209 pauci-symptomatic individuals in the French Oise region and 200 contemporary Oise blood donors. Two in-house ELISA assays, that recognize the full-length nucleoprotein (N) or trimeric Spike (S) ectodomain were implemented. We also developed two novel assays: the S-Flow assay, which is based on the recognition of S at the cell surface by flow-cytometry, and the LIPS assay that recognizes diverse antigens [including S1 or N C- terminal domain] by immunoprecipitation. Overall, the results obtained with the four assays were similar, with differences in sensitivity that can be attributed to the technique and the antigen in use. High antibody titers were associated with neutralisation activity, assessed using infectious SARS-CoV- 2 or lentiviral-S pseudotypes. In hospitalized patients, seroconversion and neutralisation occurred on 5-14 days post symptom onset, confirming previous studies. Seropositivity was detected in 29% of pauci-symptomatic individuals within 15 days post-symptoms and 3% of blood of healthy donors collected in the area of a cluster of COVID cases. Altogether, our assays allow for a broad evaluation of SARS-CoV2 seroprevalence and antibody profiling in different population subsets.
Netherlands
The world is combating an ongoing COVID-19 pandemic. Health-care systems, society and the economy are impacted in an unprecedented way. It is unclear how many people have contracted the causative coronavirus SARS-CoV-2 unknowingly. Therefore, reported COVID-19 cases do not reflect the true scale of outbreak. Natural herd immunity has been suggested as a potential exit strategy during COVID-19 outbreaks, which may arise when 50-67% of a community has been infected. Here we present the prevalence and distribution of antibodies to SARS-CoV-2 in a healthy adult population of a highly affected country using a novel immunoassay, indicating that one month into the outbreak: 1 the seroprevalence in the Netherlands is 2.7% with substantial regional variation; 2 the hardest-hit areas show a seroprevalence of up to 9.5%; 3 the seroprevalence is sex-independent throughout age groups (18-72 years); 4 antibodies are significantly more often detected in younger people 18-30 years; and 5 the number of immune individuals in the current epidemic stage is far below the herd immunity threshold. This study provides vital information on the extent of virus spread in a country where social distancing is in place, concluding that herd immunity to SARS-CoV-2 is not a realistic short-term exit strategy option.
Germany: Gangelt
Background: The world faces an unprecedented SARS-CoV2 pandemic where many critical factors still remain unknown. The case fatality rates (CFR) reported in the context of the SARS-CoV-2 pandemic substantially differ between countries. For SARS-CoV-2 infection with its broad clinical spectrum from asymptomatic to severe disease courses, the infection fatality rate (IFR) is the more reliable parameter to predict the consequences of the pandemic. Here we combined virus RT-PCR testing and assessment for SARS-CoV2 antibodies to determine the total number of individuals with SARS-CoV-2 infections in a given population.
Methods: A sero-epidemiological GCP- and GEP-compliant study was performed in a small German town which was exposed to a super-spreading event [carnival] followed by strict social distancing measures causing a transient wave of infections. Questionnaire-based information and biomaterials were collected from a random, household-based study population within a seven-day period, six weeks after the outbreak. The number of present and past infections was determined by integrating results from anti-SARS-CoV-2 IgG analyses in blood, PCR testing for viral RNA in pharyngeal swabs and reported previous positive PCR tests.
Results: Of the 919 individuals with evaluable infection status 15.5% (95% CI: [12.3%; 19.0%]) were infected. This is 5-fold higher than the number of officially reported cases for this community (3.1%). Infection was associated with characteristic symptoms such as loss of smell and taste. 22.2% of all infected individuals were asymptomatic. With the seven SARS-CoV-2-associated reported deaths the estimated IFR was 0.36% [0.29%; 0.45%]. Age and sex were not found to be associated with the infection rate. Participation in carnival festivities increased both the infection rate (21.3% vs. 9.5%, p<0.001) and the number of symptoms in the infected, estimated relative mean increase 1.6, p=0.007. The risk of a person being infected was not found to be associated with the number of study participants in the household this person lived in. The secondary infection risk for study participants living in the same household increased from 15.5% to 43.6%, to 35.5% and to 18.3% for households with two, three or four people respectively (p<0.001).
Conclusions: While the number of infections in this high prevalence community is not representative for other parts of the world, the IFR calculated on the basis of the infection rate in this community can be utilized to estimate the%age of infected based on the number of reported fatalities in other places with similar population characteristics. Whether the specific circumstances of a super-spreading event not only have an impact on the infection rate and number of symptoms but also on the IFR requires further investigation. The unexpectedly low secondary infection risk among persons living in the same household has important implications for measures installed to contain the SARS-CoV-2 virus pandemic.
Scotland
Background: The extent of spread of SARS coronavirus 2 (SARS-CoV-2) in the UK and elsewhere is unknown because typically only symptomatic individuals are diagnosed. We performed a serological study of recent blood donors in Scotland to detect antibodies to SARS-CoV-2 as a marker of past infection.
Methods: A pseudotyped SARS-CoV-2 virus microneutralisation assay was used to detect neutralising antibodies to SARS-CoV-2. The study group comprised samples from 1000 blood donors collected in Scotland during March, 2020. Controls were collected from 100 donors in Scotland during 2019. Findings. All samples collected on the 17th March, 2020 (n=500) were negative in the pseudotyped SARS-CoV-2 virus microneutralisation assay. Neutralising antibodies were detected in 5 of the 500 samples collected 21st to 23rd March; one further sample was reactive in an anti-spike ELISA.
Interpretation: Although we cannot use the rise in numbers seropositive to infer the contemporary seroprevalence or the growth rate of the epidemic, we note that they are consistent with frequency of reported diagnosed infections and SARS-CoV-2-associated deaths reported in that time period in Scotland, given that seroconversion takes up to 2-3 weeks. It should also be noted that blood donors are not representative of the general population; in particular, those with a history of recent respiratory infections are deferred. Finally, it is unknown what proportion of infected individuals seroconvert and become reactive in the assays used. Serial follow up studies are needed to track infection and seroconversion in this and other similar populations However, these data indicate that sero-surveys of blood banks can serve as a useful tool for tracking the emergence and progression of an epidemic like the current SARS-CoV-2 outbreak.
United States: Los Angeles County
In this community seroprevalence study in Los Angeles County, the prevalence of antibodies to SARS-CoV-2 was 4.65%. The estimate implies that approximately 367 000 adults had SARS-CoV-2 antibodies, which is substantially greater than the 8430 cumulative number of confirmed infections in the county in April. Therefore, fatality rates based on confirmed cases may be higher than rates based on number of infections. In addition, contact tracing methods to limit the spread of infection will face considerable challenges.
United States: Idaho
Coronavirus disease-19 (COVID19), the novel respiratory illness caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), is associated with severe morbidity and mortality. The rollout of diagnostic testing in the United States was slow, leading to numerous cases that were not tested for SARS-CoV-2 in February and March 2020, necessitating the use of serological testing to determine past infections. Here, we evaluated the Abbott SARS-CoV-2 IgG test for detection of anti-SARS-CoV-2 IgG antibodies by testing 3 distinct patient populations. We tested 1,020 serum specimens collected prior to SARS-CoV-2 circulation in the United States and found one false positive, indicating a specificity of 99.90%. We tested 125 patients who tested RT-PCR positive for SARS-CoV-2 for which 689 excess serum specimens were available and found sensitivity reached 100% at day 17 after symptom onset and day 13 after PCR positivity. Alternative index value thresholds for positivity resulted in 100% sensitivity and 100% specificity. We then tested 4,856 individuals from Boise, Idaho collected over one week in April 2020 as part of the Crush the Curve initiative and detected 87 positives for a positivity rate of 1.79%. These data demonstrate excellent analytical performance of the Abbott SARS-CoV-2 IgG test as well as the limited circulation of the virus on the West Coast. We expect the availability of high-quality serological testing will be a key tool in the fight against SARS-CoV-2.
Japan: Kolbe City
Background: Coronavirus disease 2019 (COVID-19) pandemic caused by SARS-CoV-2 has been affecting many people on earth and our society. Japan is known to have relatively less number of infections as well as deaths among developed nations. However, accurate prevalence of COVID-19 in Japan remains unknown. Therefore, we conducted a cross-sectional study to estimate seroprevalence of SARS-CoV-2 infection. Methods: We conducted a cross-sectional serologic testing for SARS-CoV-2 antibody using 1,000 samples from patients at outpatient settings who visited the clinic from March 31 to April 7, 2020, stratified by decade of age and sex.
Results: There were 33 positive IgG among 1,000 serum samples (3.3%, 95%CI: 2.3-4.6%). By applying this figure to the census of Kobe City (population: 1,518,870), it is estimated that the number of people with positive IgG be 50,123 (95%CI: 34,934-69,868). Age and sex adjusted prevalence of positivity was 2.7% (95%CI 1.8-3.9%), and the estimated number of people with positive IgG was 40,999 (95%CI: 27,333-59,221). These numbers were 396 to 858 fold more than confirmed cases with PCR testing in Kobe City.
Conclusions: Our cross-sectional serological study suggests that the number of people with seropositive for SARS-CoV-2 infection in Kobe, Japan is far more than the confirmed cases by PCR testing.
China: Wuhan
Wuhan City has ended the lockdown and people have been allowed to resume working since April 8 if meeting a set of COVID-19-associated tests including SARS-CoV-2 nucleic acid test (NAT) of nasopharyngeal swabs, chest CT scan or a SARS-CoV-2-specific serological test. Here, we reported the positive rate of COVID-19 tests based on NAT, chest CT scan and a serological SARS-CoV-2 test, from April 3 to 15 in one hospital in Qingshan Destrict, Wuhan. We observed a ~10% SARS-CoV-2-specific IgG positive rate from 1,402 tests. Combination of SARS-CoV-2 NAT and a specific serological test might facilitate the detection of COVID-19 infection, or the asymptomatic SARS-CoV-2-infected subjects. Large-scale investigation is required to evaluate the herd immunity of the city, for the resuming people and for the re-opened city.
Iran: Guilan Province
Background: The extent of infection by coronavirus disease 2019 has not been well documented. In this study we aimed to determine seropositivity of COVID-19 virus infection in population of a highly affected area in north of Iran.
Methods: In a population-based cluster random sampling design through phone call invitation, a total of 196 household including 552 subjects agreed to participate in this study. Each participant were taken 50ml blood sample at health care center. Rapid test kits were used to detect antibody against COVID-19. Crude, population-weight adjusted and test performance adjusted prevalence of antibody seropositivity to SARS-CoV-2 were reported.
Results: The prevalence of antibody seropositivity was 0.22 (95%CI: 0.19-0.26). The population weight adjusted estimate was 0.21 (95%CI: 0.14-0.29) and test performance adjusted prevalence was 0.33 (95%CI: 0.28-0.39). Based on these estimates the range of infected people in this province would be between 518000 and 777000.
Conclusion: The population seropositivity prevalence of COVID-19 virus infection indicated that the asymptomatic infection is much higher than the number of confirmed cases of COVID-19. This estimate can be used to better detect infection fatality rate and decide for public policy guidelines.
OTHER SOURCES
Spain
[Adapted from the Translation]This Thursday, the first data from the ENECOVID19 study, the seroprevalence survey that tries to estimate the%age of the population that has developed antibodies against the new SARS-Cov-2 coronavirus after passing the infection, have been presented. According to the preliminary results of the first wave of the survey, 5% of the Spanish population has been infected and has developed antibodies. There is considerable variability according to territory, with oscillations by province between 1-2% and 10-14% seroprevalence. The population’s contact with the virus [contagion cases] is greater in the central part of the peninsula. Only Madrid and Castilla-La Mancha exceed 10%, followed by Castilla y León with 7.2%, while most communities range from 2 to 5-6%. Ceuta, Melilla, Murcia, Asturias and the Canary Islands have prevalences of less than 2%.
According to these preliminary results, the prevalence of IgG anti SARS-CoV-2 antibodies in the Spanish population is 5%, and is very similar in men and women. It is lower in babies, children and young people, and remains quite homogeneous and stable in older groups.
Sweden
[Adapted from the Translation]The Public Health Authority has launched a survey to measure and estimate how many in the community have had COVID-19. Blood samples are collected from laboratories in clinical chemistry and clinical immunology in nine regions: Jämtland, Jönköping, Kalmar, Skåne, Stockholm, Uppsala, Västerbotten, Västra Götaland and Örebro.
The collection takes place during eight weeks in the spring of 2020. A total of 1,200 samples are collected each week for analysis of antibodies. Antibodies show that the immune system recognizes the SARS-CoV-2 virus.
The analyzes for week 18 ¾ a total of 1,104 analyzed samples ¾ show, as expected, the largest proportion of positive antibody tests in Stockholm. A total of 7.3% of the blood samples collected from people in Stockholm were positive in the antibody study, which can be compared with a total of 4.2% in Skåne and 3.7% in Västra Götaland.
The numbers reflect the state of the epidemic earlier in April, as it takes a few weeks for the body’s immune system to develop antibodies.
Regarding age differences, the results show that it was most common with antibodies to COVID-19 among people between 20 and 64 years. In total, 6.7% of the samples in this group were positive, which can be compared with 4.7% in the age group 0-19 years and 2.7% in the age group 65-95 years.
The antibody analyzes are done in collaboration with SciLifeLab / KTH.
Norway
NewsinEnglish.no (2020) [Webpage] Latest Corona-Related News in Brief[xxxi]
Only a small%age of Norwegianshave been infected by the Corona virus so far, Norway’s public health institute (FHI) announced Monday. That means the infection hasn’t spread much but it’s more deadly for those who do become infected. A new French study has prompted Folkehelseinstitutt to recalculate how many Norwegians are suspected of being infected, and slash the number. While they earlier thought around 1% of the population carried the virus, they now think the real number is between 0.58% and 0.73%: 32,000 to 40,000 Norwegians.
Slovenia
US Embassy in Slovenia (2020) [Webpage] COVID-19 Information[xxxii]
The Slovenian government released the results of a nationwide antibody study in which 3.1% of participants tested positive for antibodies indicating prior exposure to the novel coronavirus. Based on the study, researchers say with 95% certainty that 2-4% of the population had an immune response to COVID-19, far less than the 60-80% immunity rate believed to be needed to prevent renewed spread of the virus. Since yesterday there was no additional confirmed case, for a cumulative total of 1468. There were no additional fatalities, with the total remaining at 105. The number who are currently hospitalized is 21 persons, of whom 4 are in intensive care.
England: London
Fenn (2020) [News Article] UK tests reveal 17% of Londoners have COVID-19 antibodies[xxxiii]
The UK health secretary, Matt Hancock, says sample testing has shown that approximately17% of London’s population now have COVID-19 antibodies.
With a population of 8.9 million, the data mean roughly 1.5 million Londoners have had the disease during the crisis and produced antibodies that will fight the virus if they encounter the disease in the future.
That same testing sample found that approximately 5% of the wider UK population have antibodies, though Hancock stressed that more testing is required to paint a more accurate picture.
United States: Indiana
Preliminary results from a scientific study aimed at measuring the spread of the novel coronavirus in Indiana show a general population prevalence of about 2.8% of the state’s population.
“What we knew through conventional detection methods ¾ testing symptomatic people and those at high-risk for COVID-19 ¾ was just the tip of the iceberg,” said Nir Menachemi, lead scientist on the study and a professor and Fairbanks Endowed Chair in the Indiana University Richard M. Fairbanks School of Public Health at IUPUI. “Now we’re trying to figure out how big that iceberg actually is.” Paul Halverson, founding dean of the Fairbanks School of Public Health, said continued testing will answer this question and assist with fighting the spread of COVID-19.
“Ideally, we would test every Hoosier,” Halverson said. “But the next best thing is random-sample testing, a scientific approach that allows us to confidently assess how COVID-19 has spread in Indiana without having to test everyone.” As part of the first phase of the study, a collaboration between the Indiana State Department of Health and the Fairbanks School, researchers tested more than 4,600 Hoosiers between April 25 and May 1 for viral infections and antibodies of SARS-CoV-2, the novel coronavirus that causes COVID-19. This number includes more than 3,600 people who were randomly selected and an additional 900 volunteers recruited through outreach to the African American and Hispanic communities to more accurately represent state demographics.
After analyzing these test results, IUPUI public health researchers determined that during the last week of April, 1.7% of participants tested positive for the novel coronavirus and an additional 1.1% tested positive for antibodies ¾ bringing the estimated population prevalence of the virus in the state to 2.8%, or approximately 186,000 Hoosiers who were actively or previously infected as of May 1, Menachemi said.
United States: Miami-Dade County
Our data from this week and last tell a very similar story. In both weeks, 6% of participants tested positive for COVID-19 antibodies, which equates to 165,000 Miami-Dade County residents. This figure directly contrasts with testing site data, which indicated that there 10,000 positive cases, suggesting that the actual number of infections is potentially 16.5 times the number of those captured through testing sites and local hospitals alone. Using statistical methods that account for the limitations of the test, we are 95% certain that the true amount of infection lies between 4.4% and 7.9% of the population, or between 123,000 and 221,000 residents. These results are similar but not identical to other recent, non-randomized testing programs that have been conducted throughout the United States.
United States: Inner-City Boston
Boston officials Friday released the results of the coronavirus and antibody testing performed on 750 asymptomatic residents in some of the city’s neighborhoods hardest hit by the ongoing pandemic. The study, designed to help evaluate community exposure to the virus through representative sampling, found that of those tested in East Boston, Roslindale, and parts of Dorchester, 9.9% tested positive for antibodies and 2.6% tested positive for the coronavirus, officials said. In other words, approximately 1 in 10 residents who took part in the study had developed antibodies and about 1 in 40 tested positive for the coronavirus, meaning they are potentially infectious, officials said.
United States: New York City
Baskhar et al (2020) Cuomo Says 21% of Those Tested in N.Y.C. Had Virus Antibodies[xxxvii]
More than 21% of around 1,300 people in New York City who were tested for coronavirus antibodies this week were found to have them, Gov. Andrew M. Cuomo said on Thursday. The results were from a state program that tested 3,000 supermarket customers across New York State. Nearly 14% of the tests came back positive, Mr. Cuomo said. It was unclear just how telling the preliminary data was, as Mr. Cuomo acknowledged. And the accuracy of the antibody testing available in the United States in general has been called into question. Antibody tests are intended to signal whether a person may have built immunity to virus. They do not test for the virus itself. But if the state’s numbers indicated the true incidence of the virus, they would mean that more than 1.7 million people in New York City, and more than 2.6 million people statewide, have already been infected. That is far greater than the 250,000 confirmed cases of the virus itself that the state has recorded. It would also mean that the fatality rate from the virus was relatively low, about 0.5%, Mr. Cuomo said.
[i] World Health Organization (2020) “Immunity passports” in the context of COVID-19 Scientific Brief. https://www.who.int/news-room/commentaries/detail/immunity-passports-in-the-context-of-covid-19. [Accessed May 25 2020].
[ii] World Health Organization (2020) Population-based age-stratified seroepidemiological investigation protocol for COVID-19 virus infection. https://apps.who.int/iris/handle/10665/332188. [Accessed May 25 2020].
[iii] European Centre for Disease Prevention and Control (2020) Coronavirus disease 2019 (COVID-19) in the EU/EEA and the UK– ninth update. https://www.ecdc.europa.eu/sites/default/files/documents/covid-19-rapid-risk-assessment-coronavirus-disease-2019-ninth-update-23-april-2020.pdf [Accessed 22 May 2020].
[iv] Centers for Disease Control and Prevention (2020) Serology Testing for COVID-19 at CDC. https://www.cdc.gov/coronavirus/2019-ncov/lab/serology-testing.html [Accessed 22 May 2020].
[v] BMJ Best Practice (2020) Coronavirus disease 2019 (COVID-19) . https://bestpractice.bmj.com/topics/en-gb/3000168/pdf/3000168/Coronavirus%20disease%202019%20%28COVID-19%29.pdf. [Accessed 22 May 2020].
[vi] UpToDate (2020) Coronavirus disease 2019 (COVID-19): Epidemiology, virology, clinical features, diagnosis, and prevention. https://www.uptodate.com/contents/coronavirus-disease-2019-covid-19-epidemiology-virology-clinical-features-diagnosis-and-prevention. [Accessed 22 May 2020].
[vii] Kontou PI, Braliou GG, Dimou NL, Nikolopoulos G, Bagos PG. Antibody Tests in Detecting SARS-CoV-2 Infection: A Meta-Analysis. Diagnostics (Basel). 2020;10(5):E319. Published 2020 May 19. doi:10.3390/diagnostics10050319
[viii] Ioannidis. (2020) The infection fatality rate of COVID-19 inferred from seroprevalence data. https://www.medrxiv.org/content/10.1101/2020.05.13.20101253v1. [Accessed 25 May 2020].
[ix] Bryant JE, Azman AS, Ferrari MJ, et al Serology for SARS-CoV-2: Apprehensions, opportunities, and the path forward. Sci Immunol. 2020;5(47):eabc6347. doi:10.1126/sciimmunol.abc6347
[x] Kadkhoda K. COVID-19 serologic testing: FAQs and caveats [published online ahead of print, 2020 May 20]. Cleve Clin J Med. 2020;10.3949/ccjm.87a.20054. doi:10.3949/ccjm.87a.20054
[xi] Liu L, Liu W, Zheng Y, et al A preliminary study on serological assay for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in 238 admitted hospital patients [published online ahead of print, 2020 May 18]. Microbes Infect. 2020;S1286-4579(20)30086-1. doi:10.1016/j.micinf.2020.05.008
[xii] Quattrone F, Vabanesi M, Borghini A, De Vito G, Emdin M, Passino C. The value of hospital personnel serological screening in an integrated COVID-19 infection prevention and control strategy [published online ahead of print, 2020 May 15]. Infect Control Hosp Epidemiol. 2020;1-5. doi:10.1017/ice.2020.242
[xiii] Korth J, Wilde B, Dolff S, et al SARS-CoV-2-specific antibody detection in healthcare workers in Germany with direct contact to COVID-19 patients [published online ahead of print, 2020 May 13]. J Clin Virol. 2020;128:104437. doi:10.1016/j.jcv.2020.104437
[xiv] Madsen T, Levin N, Niehus K, et al Prevalence of IgG antibodies to SARS-CoV-2 among emergency department employees [published online ahead of print, 2020 May 3]. Am J Emerg Med. 2020;S0735-6757(20)30306-5. doi:10.1016/j.ajem.2020.04.076
[xv] Brandstetter S, Roth S, Harner S, et al Symptoms and immunoglobulin development in hospital staff exposed to a SARS-CoV-2 outbreak [published online ahead of print, 2020 May 15]. Pediatr Allergy Immunol. 2020;10.1111/pai.13278. doi:10.1111/pai.13278
[xvi] Valenti et al (2020) SARS-CoV-2 seroprevalence trends in healthy blood donors during the COVID-19 Milan outbreak. https://www.medrxiv.org/content/10.1101/2020.05.11.20098442v1. [Accessed 25 May 2020].
[xvii] Erikstrup et al (2020) Estimation of SARS-CoV-2 infection fatality rate by real-time antibody screening of blood donors. https://www.medrxiv.org/content/10.1101/2020.04.24.20075291v1. [Accessed 22 May 2020].
[xviii] Stringhini et al (2020) Repeated seroprevalence of anti-SARS-CoV-2 IgG antibodies in a population-based sample from Geneva, Switzerland. https://www.medrxiv.org/content/10.1101/2020.05.02.20088898v1. [Accessed 25 May 2020].
[xix] Fontanet et al (2020) Cluster of COVID-19 in northern France: A retrospective closed cohort study. https://www.medrxiv.org/content/10.1101/2020.04.18.20071134v1. [Accessed 25 May 2020].
[xx] Grzelak et al (2020) SARS-CoV-2 serological analysis of COVID-19 hospitalized patients, pauci-symptomatic individuals and blood donors. https://www.medrxiv.org/content/10.1101/2020.04.21.20068858v1. [Accessed 26 May 2020].
[xxi] Slot et al (2020) Herd immunity is not a realistic exit strategy during a COVID-19 outbreak. https://www.researchsquare.com/article/rs-25862/v1. [Accessed 25 May 2020].
[xxii] Streeck et al (2020) Infection fatality rate of SARS-CoV-2 infection in a German community with a super-spreading event. https://www.medrxiv.org/content/10.1101/2020.05.04.20090076v1. [Accessed 25 May 2020].
[xxiii] Thompson et al (2020) Neutralising antibodies to SARS coronavirus 2 in Scottish blood donors – a pilot study of the value of serology to determine population exposure. https://www.medrxiv.org/content/10.1101/2020.04.13.20060467v1. [Accessed 25 May 2020].
[xxiv] Sood N, Simon P, Ebner P, et al Seroprevalence of SARS-CoV-2-Specific Antibodies Among Adults in Los Angeles County, California, on April 10-11, 2020 [published online ahead of print, 2020 May 18]. JAMA. 2020;e208279. doi:10.1001/jama.2020.8279
[xxv] Bryan et al (2020) Performance Characteristics of the Abbott Architect SARS-CoV-2 IgG Assay and Seroprevalence Testing in Idaho. https://www.medrxiv.org/content/10.1101/2020.04.27.20082362v1. [Accessed 25 May 2020].
[xxvi] Doi et al (2020) Estimation of seroprevalence of novel coronavirus disease (COVID-19) using preserved serum at an outpatient setting in Kobe, Japan: A cross-sectional study. https://www.medrxiv.org/content/10.1101/2020.04.26.20079822v2. [Accessed 25 May 2020].
[xxvii] Wu X, Fu B, Chen L, Feng Y. Serological tests facilitate identification of asymptomatic SARS-CoV-2 infection in Wuhan, China [published online ahead of print, 2020 Apr 20]. J Med Virol. 2020;10.1002/jmv.25904. doi:10.1002/jmv.25904
[xxviii] Shakiba et al (2020) Seroprevalence of COVID-19 virus infection in Guilan province, Iran. https://www.medrxiv.org/content/10.1101/2020.04.26.20079244v1. [Accessed 25 May 2020].
[xxix] Instituto de Salud Carlos III (2020) [Coronavirus: los primeros datos de seroprevalencia estiman que un 5% de la población ha estado contagiada, con variabilidad según provincias] Coronavirus: the first seroprevalence data estimates that 5% of the population has been infected, with variability according to provinces. https://www.isciii.es/Noticias/Noticias/Paginas/Noticias/PrimerosDatosEstudioENECOVID19.aspx?fbclid=IwAR0askXAC4Is4rSY8EHR6S9TYAMZQWh6mAvuHNyUjNgiZP3TWe6Sj3pcwGo. [Accessed 22 May 2020].
[xxx] Public Health Agency of Sweden (2020) First results from ongoing study of antibodies to covid-19 virus. https://www.folkhalsomyndigheten.se/nyheter-och-press/nyhetsarkiv/2020/maj/forsta-resultaten-fran-pagaende-undersokning-av-antikroppar-for-covid-19-virus/. [Accessed 22 May 2020].
[xxxi] NewsinEnglish.no. (2020) Latest Corona-related news in brief. https://www.newsinenglish.no/2020/05/25/updates-here-as-corona-rages-on/. [Accessed 25 May 2020].
[xxxii] U.S. Embassy in Slovenia (2020) COVID-19 Information. https://si.usembassy.gov/covid-19-information/. [Accessed 25 May 2020].
[xxxiii] Fenn (2020) UK tests reveal 17% of Londoners have COVID-19 antibodies. https://newseu.cgtn.com/news/2020-05-22/UK-tests-reveal-17-of-Londoners-have-COVID-19-antibodies-QGoxm5G2Ig/index.html. [Accessed 26 May 2020].
[xxxiv] Indiana University News (2020) IU, ISDH release preliminary findings about impact of COVID-19 in Indiana. https://news.iu.edu/stories/2020/05/iupui/releases/13-preliminary-findings-impact-covid-19-indiana-coronavirus.html. [Accessed 25 May 2020].
[xxxv] Miami-Dade County (2020) Second round of COVID-19 community testing completed; Miami-Dade County and the University of Miami Miller School of Medicine announce initial findings. https://www.miamidade.gov/releases/2020-04-24-sample-testing-results.asp.[Accessed 25 May 2020].
[xxxvi] Gavin (2020) Boston has released the results of its coronavirus and antibody testing. Here’s what to know. https://www.boston.com/news/coronavirus/2020/05/15/boston-coronavirus-antibody-testing-results. [Accessed 25 May 2020].
[xxxvii] Baskhar et al (2020) Cuomo Says 21% of Those Tested in N.Y.C. Had Virus Antibodies. https://www.nytimes.com/2020/04/23/nyregion/coronavirus-new-york-update.html. [Accessed 25 May 2020].
Produced by the members of the National Health Library and Knowledge Service Evidence Team†. Current as at 27 May 2020.This evidence summary collates the best available evidence at the time of writing and does not replace clinical judgement or guidance. Emerging literature or subsequent developments in respect of COVID-19 may require amendment to the information or sources listed in the document. Although all reasonable care has been taken in the compilation of content, the National Health Library and Knowledge Service Evidence Team makes no representations or warranties expressed or implied as to the accuracy or suitability of the information or sources listed in the document. This evidence summary is the property of the National Health Library and Knowledge Service and subsequent re-use or distribution in whole or in part should include acknowledgement of the service.
Ronan Hegarty, Librarian, Naas General Hospital [Author]

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.