
What is the latest national and international evidence about the existence of long COVID or post-COVID and its persistence for COVID-19 survivors?
Download Full Summary of Evidence (PDF)
Main Points
- ‘Long COVID’ is described using a number of different names but is generally regarded as the persistence of symptoms at least 4 weeks post SARS-CoV-2 infection and for which there is no other clinical explanation.
- There is a broad range of potential symptoms associated with the condition, both physiological and psychological.
- Research to date is methodologically limited and more research is needed to establish a clear understanding of the mid- and long-term effects of COVID-19.
- Countries need to plan health services to meet the needs of those with persistent symptoms.
Summary of Evidence
The designation “long COVID” has its origins in social media as COVID-19 survivors shared narratives of persisting symptoms after recovery from the acute phase of illness. Post-COVID conditions are being referred to by a wide range of names, including long COVID, post-acute COVID-19, long-term effects of COVID, post-acute COVID syndrome, chronic COVID, long-haul COVID, late sequelae, and others, as well as the research term “post-acute sequelae of SARS-COV-2 infection (PASC).” Although standardized case definitions are still being developed, in the broadest sense, post-COVID conditions can be considered a lack of return to a usual state of health following acute COVID-19 illness. Post-COVID conditions might also include development of new or recurrent symptoms that occur after the symptoms of acute illness have resolved.2
The condition ‘long COVID’ has been defined by the Centers for Disease Control and Prevention (CDC) in the United States as one in which symptoms persist 4 or more weeks post infection2, 3; or by the World Health Organization1 as one in which symptoms are still in evidence 3 months after infection and continue for at least a further 3 months. Other definitions describe the period of 4-12 weeks as ongoing symptomatic COVID-19, and the period after 12 weeks as post COVID-19.6 Symptoms are typically not explained by any other diagnosis.
Clinical characteristics of the mid- and long-term effects of COVID-19 are still not clearly understood1, 2, 3, 6, and studies published to date have significant methodologic limitations, such as lack of a control population, selection and reporting bias, and lack of standardized assessment protocols7, 27. Interim guidelines have been published4, 5, but several authors highlight the need for more research8, 13, 14, including a very recent review by Yelin et al15 which states that there is “insufficient evidence to provide any recommendations other than conditional guidance.”
However, it is apparent that persistent physical symptoms following acute COVID-19 are common, and typically include fatigue, dyspnea, chest pain, and cough. Patients recovering from COVID-19 may also have additional psychological (anxiety, depression, post-traumatic stress disorder) and cognitive (poor memory and concentration) symptoms, similar to the syndrome experienced by patients recovering from other critical illnesses known as Post-Intensive Care Syndrome (PICS).7
A majority of studies agree that the most common symptoms of long COVID are both physiological and psychological, and include fatigue, breathlessness, pain, voice changes, cough, dysphagia, anxiety and depression, PTSD, problems with concentration or memory, and gastrointestinal manifestations1, 8-43. Other ongoing symptoms identified include cardiovascular44-45, oral health46-49, and neurological issues61-65, with Lopez-Leon et al32 identifying more than 50, and Hayes et al26 more than 100 symptoms. Some reviews focus principally on ongoing psychological symptoms57-59, and on the appearance of long COVID in paediatric patients70-72. Other reviews reflect on the impact of these symptoms on the quality of life of those affected33, 37.
Nguyen et al report that the main risk factors for persisting symptoms are being female, older, having comorbidities, and disease severity at the acute phase of COVID-1912.
The World Health Organisation reports that COVID-19 patients admitted to ICU had greater prevalence of symptoms in almost all reported symptom domains than COVID-19 patients not admitted to ICU.1
Several reviews suggest that there is a need to establish appropriate care models to take account of the needs of long COVID patients, including the establishment of multi-disciplinary care teams11, 12, 17, 21, 23, 25, 32, 39. Healthcare professionals and patients are encouraged to set achievable goals through shared decision-making and to approach treatment by focusing on specific symptoms or conditions. A comprehensive management plan focusing on improving physical, mental, and social wellbeing may be helpful for some patients.3
Irish and/or International Guidance
| Level 1 |
World Health Organization (2021) Living guidance for clinical management of COVID-19[1]
Section 24: Care of COVID-19 patients after acute illness
New evidence is emerging about COVID-19-related persistent symptoms, which have parallels with other coronavirus diseases. The clinical characterization of mid- and long-term effects of COVID-19 remain to be clearly described and understood. In hospitalized patients (ICU and non-ICU), there are reports of new illness-related fatigue, breathlessness, PTSD symptoms, pain, voice change, cough, dysphagia, anxiety, and depression; and problems with concentration, memory and continence. Patients admitted to ICU had greater prevalence of symptoms in almost all reported symptom domains than COVID-19 patients not admitted to ICU. More than half of all COVID-19 patients who had been hospitalized — regardless of their clinical management — reported persistence of fatigue at 60 days since onset of symptoms. Early findings report that most common ongoing symptoms (regardless of hospitalization status) are fatigue, muscle ache, shortness of breath, and headache at a follow-up of 4 months. Not returning to usual health within2–3 weeks oftesting was reported by approximately one third of symptomatic adults in an outpatient setting. A study reported that at 3 months after the onset of symptoms, one third of non-hospitalized patients were to some degree dependent on others for personal care.
| Level 1 |
Some patients who have been infected with SARS-CoV-2 have new, recurring or ongoing symptoms and clinical findings 4 or more weeks after infection, sometimes after initial symptom recovery. Post-COVID conditions can occur in patients who have had varying degrees of illness during acute infection, including those who had mild or asymptomatic infections. Medical and research communities are still learning about these post-acute symptoms and clinical findings.
Post-COVID conditions are being referred to by a wide range of names, including long COVID, post-acute COVID-19, long-term effects of COVID, post-acute COVID syndrome, chronic COVID, long-haul COVID, late sequelae, and others, as well as the research term post-acute sequelae of SARS-COV-2 infection (PASC). Although standardized case definitions are still being developed, in the broadest sense, post-COVID conditions can be considered a lack of return to a usual state of health following acute COVID-19 illness. Post-COVID conditions might also include development of new or recurrent symptoms that occur after the symptoms of acute illness have resolved.
Scientific knowledge is still limited about these effects, including what causes them and how often they occur. Interim terminology will be updated as more information becomes available.
| Level 1 |
The term “post-COVID condition” is an umbrella term for the wide range of physical and mental health consequences experienced by some patients that are present 4 or more weeks after SARS-CoV-2 infection, including by patients who had initial mild or asymptomatic acute infection. Based on current information, many post-COVID conditions can be managed by primary care providers, with the incorporation of patient-centred approaches to optimize the quality of life and function in affected patients.
Objective laboratory or imaging findings should not be used as the only measure or assessment of a patient’s well-being; lack of laboratory or imaging abnormalities does not invalidate the existence, severity, or importance of a patient’s symptoms or conditions.
Healthcare professionals and patients are encouraged to set achievable goals through shared decision-making and to approach treatment by focusing on specific symptoms or conditions; a comprehensive management plan focusing on improving physical, mental, and social wellbeing may be helpful for some patients.
Understanding of post-COVID conditions remains incomplete and guidance for healthcare professionals will likely change over time as the evidence evolves.
| Level 1 |
This guideline covers identifying, assessing and managing the long-term effects of COVID-19, often described as ‘long COVID.’ It makes recommendations about care in all healthcare settings for adults, children and young people who have new or ongoing symptoms 4 weeks or more after the start of acute COVID-19. It also includes advice on organising services for long COVID.
| Level 1 |
This guideline on managing the long-term effects of COVID-19 covers the care of people who have signs and symptoms that develop during or after an infection that is consistent with COVID-19, which continue for more than four weeks and are not explained by an alternative diagnosis. These recommendations will be of interest to general practitioners and members of the primary care team, healthcare professionals in specialist secondary care services, occupational therapists, rehabilitation medicine staff, and social workers. It will also be of interest to people experiencing long-term symptoms of COVID-19, their family and carers, supportive organisations in the voluntary sector and policy makers.
Point-of-Care Tools
| Level 2 |
BMJ Best Practice (2022) COVID-19[6]
See Section: Complications: post-COVID-19 syndrome (Long COVID)
Also known as post-acute COVID-19, post-acute COVID-19 syndrome, chronic COVID, long-haul COVID, post-acute sequelae of SARS-CoV-2 infection (PASC), and post-COVID conditions.
Definition: case definitions vary. The World Health Organization defines it as a condition that occurs in people with a history of probable or confirmed SARS-CoV-2 infection, usually occurring 3 months from the onset of symptoms and lasting for at least 2 months, which cannot be explained by an alternative diagnosis. The National Institute for Health and Care Excellence defines post-COVID-19 syndrome as signs and symptoms that develop during or after an infection consistent with COVID-19, continue for more than 12 weeks, and are not explained by an alternative diagnosis. Ongoing symptomatic COVID-19 is defined as signs and symptoms from 4 weeks up to 12 weeks. The term long COVID may be used to describe either of these case definitions. The Centers for Disease Control and Prevention defines post-COVID conditions as an umbrella term for the wide range of health consequences that are present more than 4 weeks after infection with SARS-CoV-2. The syndrome is not thought to be linked to disease severity during the acute phase of illness. Protracted symptoms are common after many viral and bacterial infections, including influenza. However, while the clinical features were also observed after influenza infection, the incidence appears to be higher after COVID-19. The neurological symptoms are similar to symptoms of other neurological conditions such as chronic fatigue syndrome and functional neurological disorder. Evidence from a cross-sectional analysis of a large, population-based cohort suggests that persistent physical symptoms after COVID-19 may be associated more with the belief in having been infected than with having laboratory-confirmed infection. Laboratory-confirmed infection was associated only with anosmia. Findings suggest that persistent physical symptoms after infection should not be automatically ascribed to COVID-19, but further research is required.
| Level 2 |
UpToDate (2022) COVID-19: Evaluation and management of adults following acute viral illness[7]
Persistent symptoms
It is important to note that many studies evaluating the prevalence and severity of persistent post-COVID-19 symptoms have significant methodologic limitations, such as lack of a control population, selection and reporting bias, and lack of standardized assessment protocols.
However, it is apparent that persistent physical symptoms following acute COVID-19 are common and typically include fatigue, dyspnea, chest pain, and cough. Patients recovering from COVID-19 may also have additional psychological (eg, anxiety, depression, posttraumatic stress disorder [PTSD]) and cognitive (eg, poor memory and concentration) symptoms, similar to the syndrome experienced by patients recovering from other critical illnesses known as post-intensive care syndrome (PICS).
Irish and/or International Literature
| Level 1 |
The authors sought to estimate the prevalence of persistent symptoms and signs at least 12 weeks after acute COVID-19 at different follow-up periods. Random-effect meta-analysis was performed to produce pooled prevalence for each symptom at 4 different follow-up time intervals.
After screening 3209 studies, a total of 63 studies were eligible for inclusion, with a total COVID-19 population of 257,348. The most commonly reported symptoms were fatigue, dyspnea, sleep disorder and concentration difficulty (32%, 25%, 24%, and 22%, respectively) at 3-6 months follow-up; effort intolerance, fatigue, sleep disorder and dyspnea (45%, 36%, 29% and 25%, respectively) at 6-9 months follow-up; fatigue (37%) and dyspnea (21%) at 9-12 months; and fatigue, dyspnea, sleep disorder, myalgia (41%, 31%, 30%, and 22%, respectively) at >12 months follow-up. There was substantial heterogeneity between-studies for all reported symptoms prevalence. Meta-regressions identified statistically significant effect modifiers: world region, male gender, diabetes mellitus, disease severity and overall study quality score. Five of six studies including a comparator group consisting of COVID-19 negative cases observed significant adjusted associations between COVID-19 and several long-term symptoms.
This systematic review found that a large proportion of patients experience continuing symptoms 3 to 12 months after recovery from the acute phase of COVD-19. However, available studies are highly heterogeneous. Future studies need to have appropriate comparator groups, standardized symptom definitions and measurements, and longer follow-up.

| Level 1 |
D’ETTORRE et al (2022) COVID-19 sequelae in working age patients: A systematic review[9]
This systematic review found that the most frequent organic sequelae found in post-COVID patients was pulmonary fibrosis. The number of symptoms during the acute phase of SARS-CoV-2 infection, severity of disease, and high serum levels of D-dimer were related to high risk of post-COVID syndrome. Rehabilitation and follow-up in multidisciplinary rehabilitation programs should be considered for working-age patients.
| Level 1 |
This study aimed to systematically synthesise evidence on post-COVID symptoms persisting for at least 12 months. Random-effects meta-analyses were conducted to estimate pooled prevalence of specific post-COVID symptoms. Eighteen papers that reported one-year follow-up data from 8591 COVID-19 survivors were included. Fatigue/weakness (28%, 95% CI: 18-39), dyspnoea (18%, 95% CI: 13-24), arthromyalgia (26%, 95% CI: 8-44), depression (23%, 95% CI: 12-34), anxiety (22%, 95% CI: 15-29), memory loss (19%, 95% CI: 7-31), concentration difficulties (18%, 95% CI: 2-35), and insomnia (12%, 95% CI: 7-17) were the most prevalent symptoms at one-year follow-up. Existing evidence suggested that female patients and those with more severe initial illness were more likely to suffer from the sequelae after one year.
The authors affirm that there is an urgent need for elucidating the pathophysiologic mechanisms and developing and testing targeted interventions for long-COVID patients.
| Level 6 |
The authors sought to explore the experiences of people living with long COVID and how they perceive the healthcare services available to them.
Papers reporting qualitative or mixed-methods studies that focused on the experiences of long COVID and/or perceptions of accessing healthcare by people with long COVID were included. Five studies met the inclusion criteria. Participants were predominantly young white females recruited from social media or online support groups. Three analytical themes were generated: symptoms and self-directed management of long COVID; emotional aspects of living with long COVID; and healthcare experiences associated with long COVID.
The authors conclude that people experience long COVID as a heterogeneous condition, with a variety of physical and emotional consequences. The design of emerging long COVID services or adaptation of existing services for long COVID patients should take account of patients’ varied experiences.
| Level 1 |
This study aimed to describe the burden of the long-term persistence of clinical symptoms in COVID-19 patients. The authors included studies on the prevalence of somatic clinical symptoms lasting at least 4 weeks after the onset of a PCR- or serology-confirmed diagnosis of COVID-19. The prevalence of persisting clinical symptoms was assessed and risk factors described when investigated. Psychological symptoms and cognitive disorders were not evaluated.
Thirty-seven articles met the inclusion criteria. Eighteen studies involved in-patients only with a duration of follow-up of either less than 12 weeks, 12 weeks to 6 months, or more than 6 months. In these studies, fatigue (16-64%), dyspnea (15-61%), cough (2-59%), arthralgia (8-55%), and thoracic pain (5-62%) were the most frequent persisting symptoms. In nineteen studies conducted in a majority of out-patients, the persistence of these symptoms was lower, and 3% to 74% of patients reported prolonged smell and taste disorders. The main risk factors for persisting symptoms were being female, older, having comorbidities, and disease severity at the acute phase of COVID-19.
The authors conclude that COVID-19 patients should have access to dedicated multidisciplinary healthcare allowing a holistic approach. Effective outpatient care for patients with long-COVID-19 requires coordination across multiple sub-specialties, which can be proposed in specialized post-COVID units.
| Level 6 |
PIERCE et al (2022) Post-COVID-19 Syndrome[13]
The purpose of this integrative review was to summarize and evaluate post-COVID-19 syndrome from a biological perspective. The authors’ literature search generated 27,929 articles; 68 articles, including 54 specifically related to the pathophysiology of post-COVID-19 syndrome, were retained. Findings indicate that there were four pathophysiologic categories involved: virus-specific pathophysiologic variations; oxidative stress; immunologic abnormalities; and inflammatory damage.
Although studies examining the pathophysiology of post-COVID-19 syndrome are still relatively few, there is growing evidence that this is a complex and multifactorial syndrome involving virus-specific pathophysiologic variations that affect many mechanisms, but specifically oxidative stress, immune function, and inflammation. Further research is needed to elucidate the pathophysiology, pathogenesis, and longer-term consequences involved in post-COVID-19 syndrome.
| Level 6 |
The main objective of this systematic review was to create an overview of the nature and frequency of persistent symptoms experienced by patients after mild COVID-19 infection.
In total, nine articles were included in the systematic review. The frequency of persistent symptoms in patients after mild COVID-19 infection ranged between 10% and 35%. Symptoms persisting after a mild COVID-19 infection can be distinguished into physical, mental, and social symptoms. Fatigue was the most frequently described persistent symptom. Other frequently occurring persistent symptoms were dyspnoea, cough, chest pain, headache, decreased mental and cognitive status, and olfactory dysfunction. In addition, the authors found that persisting symptoms after a mild COVID-19 infection can have major consequences for work and daily functioning.
| Level 6 |
YELIN et al (2022) ESCMID rapid guidelines for assessment and management of long COVID[15]
The aim of these guidelines is to provide evidence-based recommendations for assessment and management of individuals with persistent symptoms after acute COVID-19 infection, and provide a definition for this entity, termed “long COVID.”
The authors performed a search of the literature on studies addressing epidemiology, symptoms, assessment, and treatment of long COVID. The recommendations were grouped by these headings and by organ systems for assessment and treatment. An expert opinion definition of long COVID is provided. Symptoms were reviewed by a search of the available literature. For assessment recommendations, the authors attempted to perform a diagnostic meta-analysis, but no studies provided relevant results. For treatment recommendations, the authors performed a systematic review of the literature in accordance with the PRISMA statement. The authors evaluated patient-related outcomes, including quality of life, return to baseline physical activity, and return to work.
Evidence was insufficient to provide any recommendation other than conditional guidance. The panel recommended considering routine blood tests, chest imaging and pulmonary functions tests for patients with persistent respiratory symptoms at 3 months. Other tests should be performed mainly to exclude other conditions according to symptoms. For management, no evidence-based recommendations could be provided. Physical and respiratory rehabilitation should be considered. On the basis of limited evidence, the panel suggested designing high quality prospective clinical studies, including a control group, to further evaluate assessment and management of individuals with persistent symptoms of COVID-19.
| Level 6 |
AHMAD et al (2021) “Long COVID”: an insight[16]
This systematic review aimed to analyze and review the currently available published literature relating to long COVID, understand its pattern, and predict the long-term effects on survivors. Twenty articles were regarded as eligible and analyzed in the present analysis. All of the included studies had an adult population.
The median length of hospital stay of COVID-19 patients during the acute infection phase ranged from 8 days to 17 days. The most common prevalent long-term symptoms in COVID-19 patients included persistent fatigue and dyspnea. Other reported common symptoms included shortness of breath, cough, joint pain, chest pain or tightness, headache, loss of smell/taste, sore throat, diarrhea, loss of memory, depression, and anxiety. Associated cardiovascular events included arrhythmias, palpitations, and hypotension, increased heart rate, venous thromboembolic diseases, myocarditis, and acute/decompensated heart failure. Among neurological manifestations, headache, peripheral neuropathy symptoms, memory issues, concentration, and sleep disorders were most commonly observed with varying frequencies. Mental health issues including mood fluctuations, anxiety, depression and sleep disorders were commonly observed. Further, diarrhea, vomiting, digestive disorders, and loss of appetite or weight loss were common gastrointestinal manifestations.
| Level 6 |
AIYEGBUSI et al (2021) Symptoms, complications and management of long COVID: a review[17]
Patients with ‘long COVID’ experience a wide range of physical and mental/psychological symptoms. Pooled prevalence data showed the 10 most prevalent reported symptoms were fatigue, shortness of breath, muscle pain, joint pain, headache, cough, chest pain, altered smell, altered taste, and diarrhoea. Other common symptoms were cognitive impairment, memory loss, anxiety, and sleep disorders. Apart from symptoms and complications, individuals with long COVID often reported impaired quality of life, mental health, and employment issues. These individuals may require multidisciplinary care involving the long-term monitoring of symptoms to identify potential complications, physical rehabilitation, mental health, and social services support. Resilient healthcare systems are needed to ensure efficient and effective responses to future health challenges.
| Level 6 |
AKBARIALIABAD et al (2021) Long COVID, a comprehensive systematic scoping review[18]
Of 120 papers identified as part of their systematic scoping review, the authors found one randomized clinical trial. Of the 67 original studies, 22 were cohort, and 28 were cross-sectional studies. Of the total 120 publications, 49.1% focused on signs and symptoms, 23.3% on management, and 10.8% on pathophysiology. Ten publications focused on imaging studies. The results are presented in a narrative synthesis in separate sections: nomenclature; diagnosis; pathophysiology; risk factors; signs/symptoms; management.
The predominant symptoms identified were fatigue, breathlessness, arthralgia, sleep difficulties, and chest pain. Recent reports also point to the risk of long-term sequela with cutaneous, respiratory, cardiovascular, musculoskeletal, mental health, neurologic, and renal involvement in those who survive the acute phase of the illness.
| Level 1 |
ANAYA et al (2021) Post-COVID syndrome. A case series and comprehensive review[19]
Adult patients with previously confirmed SARS-CoV-2 infection and a diagnosis of post-COVID syndrome (PCS) were systematically assessed through a semi-structured and validated survey. Total IgG, IgA and IgM serum antibodies to SARS-CoV-2 were evaluated by an electrochemiluminescence immunoassay. A systematic review of the literature and meta-analysis were conducted. Out of a total of 100 consecutive patients, 53 were women, the median of age was 49 years (IQR: 37.8-55.3), the median of post-COVID time after the first symptoms was 219 days (IQR: 143-258), and 65 patients were hospitalized during acute COVID-19. Musculoskeletal, digestive, and neurological symptoms including depression were the most frequently observed in PCS patients. A previous hospitalization was not associated with PCS manifestation. Arthralgia and diarrhea persisted in more than 40% of PCS patients. The median of anti-SARS-CoV-2 antibodies was 866.2 U/mL (IQR: 238.2-1681). Despite this variability, 98 patients were seropositive. Based on autonomic symptoms, two clusters were obtained with different clinical characteristics. Levels of anti-SARS-CoV-2 antibodies were not different between clusters. A total of 40 articles (11,196 patients) were included in the meta-analysis. Fatigue/muscle weakness, dyspnea, pain and discomfort, anxiety/depression, and impaired concentration were presented in more than 20% of patients reported.
The authors conclude that PCS is mainly characterized by musculoskeletal, pulmonary, digestive, and neurological involvement, including depression. PCS is independent of severity of acute illness and humoral response. Long-term antibody responses to SARS-CoV-2 infection and a high inter-individual variability were confirmed.
| Level 1 |
The authors aimed to identify, systematically evaluate and summarise the best available evidence on the frequency of long COVID-19 (post-acute COVID-19 syndrome), its clinical manifestations, and the criteria used for diagnosis.
25 observational studies with moderate to high methodological quality, considering 5440 participants, were included in the systematic review. The frequency of long COVID-19 ranged from 4.7% to 80%, and the most prevalent signs/symptoms were chest pain (up to 89%), fatigue (up to 65%), dyspnea (up to 61%), and cough and sputum production (up to 59%). Temporal criteria used to define long COVID-19 varied from 3 to 24 weeks after acute phase or hospital discharge. Potentially associated risk factors were old age, female sex, severe clinical status, a high number of comorbidities, hospital admission, and oxygen supplementation at the acute phase. However, limitations related to study designs added uncertainty to this finding. None of the studies assessed the duration of signs/symptoms.
Based on these systematic review findings, the authors affirm that there is an urgent need to understand this emerging, complex and challenging medical condition. Proposals for diagnostic criteria and standard terminology are welcome.
| Level 6 |
CHA et al (2021) Symptoms and management of long COVID: A scoping review[21]
This scoping review aims to describe published work on the symptoms and management of long COVID conditions. Among the 1880 articles retrieved, 34 articles met the authors’ criteria for review. Long COVID symptoms were described in 21 articles. After COVID-19 treatment, hospitalised patients most frequently reported dyspnoea, followed by anosmia/ageusia, fatigue and cough, while non-hospitalised patients commonly reported cough, followed by fever and myalgia/arthralgia. Thirteen studies described management of long COVID, with 7 articles focussing on a multidisciplinary approach, 3 on pulmonary rehabilitation, two on fatigue management, and one on psychological therapy.
The authors recommend that a rehabilitation care plan and community healthcare plans are necessary for COVID-19 patients before discharge.; and that remote programmes could facilitate the monitoring and screening of people with long COVID.
| Level 1 |
The primary aim of this study was to examine the prevalence of post-acute sequelae of COVID-19 (PASC) and to assess geographic heterogeneities through a systematic review and meta-analysis. A second aim was to provide prevalence estimates for individual symptoms that have been commonly reported as PASC.
Findings suggest that globally PASC comprises a significant fraction (0.43 [95% CI: 0.35, 0.63]) of COVID-19 tested positive cases and more than half of hospitalized COVID-19 cases, based on available literature as of August 12, 2021. Geographic differences appear to exist, as lowest to highest PASC prevalence is observed for North America (0.30 [95% CI: 0.32, 0.66]) to Asia (0.49 [95% CI: 0.21, 0.42]). The case-mix across studies in respect of COVID-19 severity during the acute phase of infection and variation in the clinical definition of PASC may explain some of these differences. Nonetheless, the health effects of COVID-19 appear to be prolonged and can exert marked stress on healthcare systems.
| Level 6 |
DECARY et al (2021) [PREPRINT] Care models for long COVID: A rapid systematic review [23]
The authors screened 2181 citations and included 12 eligible articles reporting on care models for long COVID. The authors found that implementation of care models for long COVID is underway in several countries. Care models need to include both hospitalized and non-hospitalized patients. A complete care model for this population appears to design a care pathway integrating primary care, rehabilitation services and specialized clinics for medical assessment. The authors suggest that entry into care pathways is possible through a centralized referral system.
| Level 1 |
This meta-analysis analyses the prevalence of post-COVID-19 symptoms in hospitalized and non-hospitalized patients recovered from COVID-19.
From 15,577 studies identified, 29 peer-reviewed studies and 4 preprints met the authors’ inclusion criteria. The sample included 15,244 hospitalized and 9011 non-hospitalized patients. Results showed that 63.2, 71.9 and 45.9% of the sample exhibited at least one post-COVID-19 symptom at 30, 60, or ≥90days after onset/hospitalization. Fatigue and dyspnea were the most prevalent symptoms with a pooled prevalence ranging from 35% to 60% depending on the follow-up. Other post-COVID-19 symptoms included cough (20-25%), anosmia (10-20%), ageusia (15-20%) or joint pain (15-20%). Time trend analysis revealed a decreased prevalence 30days after with an increase after 60 days .
| Level 6 |
GARG et al (2021) The conundrum of long-COVID-19: A narrative review[25]
‘Long-COVID-19’ is a term given to the lingering or protracted illness that patients of COVID-19 continue to experience even in their post-recovery phase. Fatigue, dyspnea, cough, headache, brain fog, anosmia, and dysgeusia are common symptoms seen in long-COVID-19, but more varied and debilitating injuries involving pulmonary, cardiovascular, cutaneous, musculoskeletal and neuropsychiatric systems are also being reported. With the re-emergence of new waves of SARS-CoV-2 infection, long-COVID-19 is expected to produce another public health crisis on the heels of current pandemic. Thus, it becomes imperative to emphasize this condition and disseminate its awareness to medical professionals, patients, the public, and policymakers to prepare and augment health care facilities for continued surveillance of these patients. Further research comprising cataloguing of symptoms, longer-ranging observational studies, and clinical trials are necessary to evaluate long-term consequences of COVID-19, and it warrants setting-up of dedicated, post-COVID care, multi-disciplinary clinics, and rehabilitation centres.
| Level 6 |
In this scoping review of the literature, the authors aggregated type and prevalence of symptoms in people with long COVID. Original investigations concerning the name and prevalence of symptoms were considered in participants ≥4-weeks post-infection.
Among the 50 studies included in the authors’ analysis, in total, >100 symptoms were identified, and there was considerable heterogeneity in symptom prevalence. 10 studies reported cardiovascular symptoms; 4 examined pulmonary symptoms; 25 reported respiratory symptoms; 24 reported pain-related symptoms; 21 reported fatigue; 16 reported general infection symptoms; 10 reported symptoms of psychological disorders; 9 reported cognitive impairment; 31 reported a sensory impairment; 7 reported a dermatological complaint; 11 reported a functional impairment; and 18 reported a symptom which did not fit into any of the above categories.
| Level 1 |
A significant proportion of individuals experience lingering and debilitating symptoms following acute COVID-19 infection. The National Institute for Health and Care Excellence (NICE) have designated the persistent cluster of symptoms as post-COVID syndrome (PCS). PCS has been further sub-categorised into acute post-COVID syndrome for symptoms persisting 3 weeks beyond initial infection, and chronic post-COVID syndrome for symptoms persisting beyond 12 weeks. The aim of this review was to ascertain the prevalence of clinical features and identify potential predictors for acute and chronic PCS.
A total of 43 studies met the authors’ eligibility criteria, of which 38 allowed for meta-analysis. Fatigue and dyspnoea were the most prevalent symptoms in acute post-COVID (0·37 and 0·35) and fatigue and sleep disturbance in chronic post-COVID syndrome (0·48 and 0·44), respectively. The available evidence is generally of poor quality, with considerable risk of bias.
| Level 6 |
IWU et al (2021) The occurrence of long COVID: a rapid review[28]
This rapid review aimed to synthesize evidence on the long-term effects of SARS-CoV-2 infection among survivors. Eleven studies met the authors’ inclusion criteria. All of these studies were conducted in high-income countries.
Study findings demonstrate that COVID-19 survivors can experience persistent symptoms after recovering from their initial illness, especially among previously hospitalized persons. The majority of symptoms reported were fatigue, shortness of breath, cough, and sleep disorders. Mental conditions such as depression and anxiety disorders were also reported. There is a need for a long-term follow-up of COVID-19 patients and rehabilitation services for survivors.
| Level 1 |
The authors sought to compare the two phases of long COVID, namely ongoing symptomatic COVID-19 (OSC; signs and symptoms from 4 to 12 weeks from initial infection), and post-COVID-19 syndrome (PCS; signs and symptoms beyond 12 weeks) with respect to symptomatology, abnormal functioning, psychological burden, and quality of life.
Of the 1145 studies screened, 39 were included, all describing adult cohorts with long COVID and sample sizes ranging from 32 to 1733. Studies included data pertaining to symptomatology, pulmonary functioning, chest imaging, cognitive functioning, psychological disorder, and/or quality of life. Fatigue presented as the most prevalent symptom during both OSC and PCS at 43% and 44%, respectively. Sleep disorder (36%; 33%), dyspnoea (31%; 40%), and cough (26%; 22%) followed in prevalence. Abnormal spirometry (FEV1 < 80% predicted) was observed in 15% and 11%, and abnormal chest imaging was observed in 34% and 28%, respectively. Cognitive impairments were also evident (20%; 15%), as well as anxiety (28%; 34%) and depression (25%; 32%). Decreased quality of life was reported by 40% in those with OSC and 57% with PCS.
Reported symptoms covered a wide range of body systems, with a general overlap in frequencies between the two phases. However, abnormalities in lung function and imaging seemed to be more common in OSC, while anxiety, depression, and poor quality of life seemed more frequent in PCS. In general, the quality of the evidence was moderate, and further research is needed to understand longitudinal symptomatology trajectories in long COVID.
| Level 6 |
LEVINER (2021) Recognizing the Clinical Sequelae of COVID-19 in Adults: COVID-19 Long-Haulers[30]
This review of the literature provides information to nurse practitioners working in primary care about symptoms, risk factors, and resources for disease management.
| Level 1 |
To explore existing data about post-acute COVID-19 syndrome, this meta-analysis assesses the prevalence of persistent manifestations in multiple systems and abnormalities in lung function, as well as their related risks in patients with various severities.
A total of 4,478 COVID-19 patients from 16 cohort studies were included in this meta-analysis. Fatigue or weakness (47%) were the most prevalent physical effects of post-acute COVID-19 syndrome, while psychosocial (28%) symptoms were the most common manifestations among several systems. Abnormalities in lung function of recovering patients (ie, DLCO <80% (47%, 95% CI: 32-61%)) persisted for long periods. Severe patients were more likely to present joint pain (OR 1.84, 95% CI: 1.11-3.04) and decreased lung functions compared with non-severe patients, with pooled ORs for abnormal TLC, FEV1, FVC, and DLCO of 3.05 (95% CI: 1.88-4.96), 2.72 (95% CI: 1.31-5.63), 2.52 (95% CI: 1.28-4.98), and 1.82 (95% CI: 1.32-2.50), respectively.
| Level 1 |
This systematic review and meta-analysis aimed to identify studies assessing the long-term effects of COVID-19. A total of 18,251 publications were identified, of which 15 met the authors’ inclusion criteria. The prevalence of 55 long-term effects was estimated; 21 meta-analyses were performed; and 47,910 patients were included (age 17-87 years). The included studies defined long-COVID as ranging from 14 to 110 days post-viral infection. It was estimated that 80% of the infected patients with SARS-CoV-2 developed one or more long-term symptoms. The five most common symptoms were fatigue (58%), headache (44%), attention disorder (27%), hair loss (25%), and dyspnea (24%). Multi-disciplinary teams are crucial to developing preventive measures, rehabilitation techniques, and clinical management strategies with whole-patient perspectives designed to address long COVID-19 care.

| Level 1 |
The authors aimed to evaluate the pooled prevalence of poor quality of life in post-acute COVID-19 syndrome (PCS), and conducted meta-regression to evaluate the effects of persistent symptoms and intensive care unit (ICU) admission on poor quality of life. A total of 12 studies with 4828 PCS patients were included. The authors found that among PCS patients, the pooled prevalence of poor quality of life (EQ-VAS) was (59%; 95% CI: 42%-75%). Based on individual factors in the EQ-5D-5L questionnaire, the prevalence of mobility was (36%, 10%-67%), personal care (8%, 1%-21%), usual quality (28%, 2%-65%), pain/discomfort (42%, 28%-55%), and anxiety/depression (38%, 19%-58%). The prevalence of persistent symptoms was fatigue (64%, 54%-73%), dyspnea (39.5%, 20%-60%), anosmia (20%, 15%-24%), arthralgia (24.3%, 14%-36%), headache (21%, 3%-47%), sleep disturbances (47%, 7%-89%), and mental health (14.5%, 4%-29%). Meta-regression analysis showed the poor quality of life was significantly higher among post-COVID-19 patients with ICU admission (p = 0.004) and fatigue (p = 0.0015).
The authors conclude that PCS is associated with poor quality of life, persistent symptoms including fatigue, dyspnea, anosmia, sleep disturbances, and deteriorating mental health.
| Level 1 |
MICHELEN et al (2021) Characterising long COVID: a living systematic review[34]
While it is now apparent clinical sequelae (long COVID) may persist after acute COVID-19, their nature, frequency and aetiology are poorly characterised. This living systematic review aims to regularly synthesise evidence on long COVID characteristics, to help inform clinical management, rehabilitation strategies and interventional studies to improve long-term outcomes.
A total of 39 studies were included: 32 cohort, 6 cross-sectional, and 1 case-control. Most showed high or moderate risk of bias. None were set in low-income countries, and few included children. Studies reported on 10 951 people (48% female) in 12 countries. Most included previously hospitalised people (78%, 8520/10 951). The longest mean follow-up time was 221.7 (SD: 10.9) days post COVID-19 onset. Over 60 physical and psychological signs and symptoms with wide prevalence were reported, most commonly weakness (41%; 95% CI 25% to 59%), general malaise (33%; 95% CI 15% to 57%), fatigue (31%; 95% CI 24% to 39%), concentration impairment (26%; 95% CI 21% to 32%), and breathlessness (25%; 95% CI 18% to 34%). 37% (95% CI 18% to 60%) of patients reported reduced quality of life; 26% (10/39) of studies presented evidence of reduced pulmonary function.
Long COVID is a complex condition with prolonged heterogeneous symptoms. There is an urgent need for prospective, robust, standardised, controlled studies into aetiology, risk factors and biomarkers to characterise long COVID in different at-risk populations and settings.
| Level 1 |
NASSERIE et al (2021) Assessment of the Frequency and Variety of Persistent Symptoms Among Patients With COVID-19: A Systematic Review[35]
The authors conducted a systematic review of studies examining the frequency and variety of persistent symptoms after COVID-19 infection.
Persistent symptoms were defined as those persisting for at least 60 days after diagnosis, symptom onset, or hospitalization or at least 30 days after recovery from the acute illness or hospital discharge. A total of 47 studies were deemed eligible, and 45 studies reporting 84 clinical signs or symptoms were included in the systematic review. Of 9751 total participants, 5266 (54.0%) were male; 30 of 45 studies reported mean or median ages younger than 60 years. Among 16 studies, most of which comprised participants who were previously hospitalized, the median proportion of individuals experiencing at least 1 persistent symptom was 72.5% (interquartile range [IQR], 55.0%-80.0%). Individual symptoms occurring most frequently included shortness of breath or dyspnea (26 studies; median frequency, 36.0%; IQR, 27.6%-50.0%), fatigue or exhaustion (25 studies; median frequency, 40.0%; IQR, 31.0%-57.0%), and sleep disorders or insomnia (8 studies; median 29.4%, IQR, 24.4%-33.0%). There were wide variations in the design and quality of the studies, which had implications for interpretation and often limited direct comparability and combinability. Major design differences included patient populations, definitions of time zero, follow-up lengths, and outcome definitions, including definitions of illness severity.
| Level 6 |
The authors state that current evidence supports the contention that a high proportion of COVID-19 survivors complain of symptoms months after the acute illness phase, with fatigue and reduced tolerance to physical effort the most frequently reported symptoms. Respiratory symptoms, persistent motor impairment, and mental health complications such as anxiety, depression, sleep disturbances, and post-traumatic stress are also reported among COVID-19 survivors.
| Level 1 |
In total, 12 eligible studies were included in this structured review. The majority of studies used a generic health-related quality of life (HRQoL) assessment tool. The impact of COVID-19 on HRQoL was found to be considerable in both acute COVID and long COVID patients. Higher impact on HRQoL was reported in acute COVID, females, older ages, patients with more severe disease and patients from low-income countries.
| Level 6 |
The authors describe mechanisms by which RNA viruses beyond SARS-CoV-2 are connected to long-term health consequences; and also review literature on acute COVID-19 and other virus-initiated chronic syndromes to discuss different scenarios for post-acute sequelae of COVID-19 (PASC) symptom development. Potential PASC symptoms include consequences from acute SARS-CoV-2 injury to one or multiple organs, persistent reservoirs of SARS-CoV-2 in certain tissues, re-activation of neurotrophic pathogens such as herpesviruses under conditions of COVID-19 immune dysregulation, SARS-CoV-2 interactions with host microbiome/virome communities, clotting or coagulation issues, dysfunctional brainstem/vagus nerve signalling, ongoing activity of primed immune cells, and autoimmunity due to molecular mimicry between pathogen and host proteins. The individualized nature of PASC symptoms suggests that different therapeutic approaches may be required to best manage care for specific patients with the diagnosis.
| Level 6 |
PYE et al (2021) A public health approach to estimating the need for long COVID services[39]
A literature review was conducted between October and December 2020 to identify prevalence estimates for long COVID. The prevalence estimates were applied to locally available data on the susceptible population to estimate the number of people with long COVID.
Findings were valuable in informing early service developments, engaging with managers and clinicians, and supporting applications for funding at a local level.
| Level 1 |
The authors conducted a systematic review to summarize what is known about long term sequelae among patients who were hospitalized for severe COVID-19 pneumonia.
12 studies were identified, with data obtained for 4693 patients: 11 studies included hospitalized patients, 8 included ICU patients, and 5 included outpatients. Follow-up time ranged from 16 days to 122 days post-hospitalization. The pooled prevalence of persistent constitutional and respiratory symptoms was: [overall] (45.6%), dyspnea (35.5%), cough (26.4%), joint pain (26.8%), myalgia (23.3%), headache (22.2%), and chest pain (20.5%). Heterogeneity across studies was high (I2>90%). Chinese studies reported a lower frequency of persistent symptoms compared with studies carried out in Western countries. There were no significant differences in long-term sequelae between ICU and non-ICU patients.
| Level 1 |
TUCCI and SAARY (2021) Persistent and Emergent Clinical Sequelae of Mild COVID-19[41]
The authors conducted a systematic review of the literature to characterize the nature and timing of persistent and emergent clinical sequelae in milder COVID-19 cases to facilitate development of post-COVID-19 screening and surveillance protocols.
Among those with mild COVID-19, sequelae were shown to emerge or persist for months following presumed recovery. Among those with no comorbidities, cardiac, hematological, and respiratory sequelae emerged after 1-2 months, and primarily cardiac abnormalities persisted at ≥3 months. Among those with minor comorbidities, persistent respiratory abnormalities, fatigue, dyspnea, and headache were common, and mental health symptoms emerged by 1-2 months post-infection.
| Level 1 |
WILLI et al (2021) COVID-19 sequelae in adults aged less than 50 years: A systematic review[42]
The authors conducted a systematic review which aimed to evaluate the available evidence of all intermediate and long-term COVID-19 sequelae affecting formerly healthy adults. Older individuals (>50 years) and children (<18 years) were excluded. A total of 31 papers were included.
Sequelae persistence since infection spanned 14 days to 3 months. Sequelae included persistent fatigue (39%–73% of assessed persons), breathlessness (39%–74%), decrease in quality of life (44%–69%), impaired pulmonary function, abnormal CT findings including pulmonary fibrosis (39%–83%), evidence of peri-/perimyo-/myocarditis (3%–26%), changes in microstructural and functional brain integrity with persistent neurological symptoms (55%), increased incidence of psychiatric diagnoses (5.8% versus 2.5%–3.4% in controls), incomplete recovery of olfactory and gustatory dysfunction (33%–36% of evaluated persons). A variety of organ systems are affected by COVID-19 in the intermediate and longer-term after recovery. Main sequelae include post-infectious fatigue, persistent reduced lung function and carditis. Careful follow-up post COVID 19 is indicated to assess and mitigate possible organ damage and preserve life quality.
| Level 6 |
WU et al (2021) Persistence of Symptoms After Discharge of Patients Hospitalized Due to COVID-19[43]
The authors conducted a literature review on the clinical manifestations of long COVID-19, defined by the persistence of symptoms beyond the acute phase of infection. The most common persistent symptoms were fatigue, cough, dyspnea, chest pains, chest tightness, joint pain, muscle pain, loss of taste or smell, hair loss, sleep difficulties, anxiety, and depression. Some of the less common persistent symptoms were skin rash, decreased appetite, sweating, inability to concentrate, and memory lapses. In addition to these general symptoms, some patients experienced dysfunctions of specific organs, mainly the lungs, heart, kidneys, and nervous system. A comprehensive understanding of the persistent clinical manifestations of COVID-19 can improve and facilitate patient management and referrals. Prompt rehabilitative care and targeted interventions of these patients may improve their recovery from physical, immune, and mental health symptoms.
Cardiovascular
| Level 6 |
CHILAZI et al (2021) COVID and Cardiovascular Disease: What We Know in 2021[44]
Early case reports described a spectrum of cardiovascular manifestations of COVID-19, including myocarditis, stress cardiomyopathy, myocardial infarction, and arrhythmia. However, in most cases, myocardial injury in COVID-19 appears to be predominantly mediated by the severity of critical illness, rather than direct injury to myocardium from viral particles. Long COVID or post-acute sequelae of SARS-CoV-2 infection has also been described. The reported symptoms span a large breadth of cardiopulmonary and neurologic complaints including fatigue, palpitations, chest pain, breathlessness, brain fog, and dysautonomia including postural tachycardia syndrome.
| Level 1 |
This systematic review characterizes the course of clinical, laboratory, and radiological findings during the primary infection period, and the complications post-recovery. Primary care findings are presented for long-COVID care.
The authors identified 29 studies across 9 countries including 37.9% Chinese and 24.1% US studies, comprising 655 patients (mean age = 45) with various ethnic backgrounds. Initial disease severity was mild for 377 patients and severe for 52 patients. The mean value for complication onset after acute recovery was 28 days. Post-recovery infectious complications are common in long-COVID-19 patients ranging from mild infections to life-threatening conditions. International thoracic and cardiovascular societies need to develop guidelines for patients recovering from COVID-19 pneumonia, while focused patient care by the primary care physician is crucial to curb preventable adverse events.
Dental/Oral Health/ENT
| Level 6 |
FRANCE (2022) Long COVID and oral health care considerations[46]
People who have recovered from the initial SARS-CoV-2 infection are at risk of developing long COVID, a prolonged suite of signs and symptoms that may interfere with daily life and the ability to undergo routine oral health care.
Long COVID includes a wide variety of symptoms, such as fatigue, shortness of breath, chest pain, risk of developing thromboembolism, and neurologic and psychiatric complications. These symptoms may arise at various times and in a wide range of patients, and they may necessitate modification of routine oral health care interventions.
Recommendations for the treatment of affected people in an oral health care setting are presented, including a thorough evaluation of the patient history and current status, understanding of how related symptoms may affect oral health care interventions, and which modifications to treatment are needed to provide safe and appropriate care.
Oral health care professionals must be aware of long COVID, an increasingly prevalent condition with a widely variable presentation and impact. Oral health care professionals should be prepared to treat these patients safely in an outpatient oral health setting.
| Level 6 |
WU et al (2022) Management of post-COVID-19 olfactory dysfunction[47]
Olfactory dysfunction is a frequent complication of SARS-CoV-2 infection. This review presents the current literature regarding the management of post-COVID-19 olfactory dysfunction (PCOD).
A systematic review of the literature was performed. While most cases of post-COVID-19 olfactory dysfunction resolve spontaneously within 2 weeks of symptom onset, patients with symptoms that persist past 2 weeks require medical management. The intervention with the greatest degree of supporting evidence is olfactory training, wherein patients are repeatedly exposed to potent olfactory stimuli. To date, no large-scale randomized clinical trials exist that examine the efficacy of pharmacologic therapies for PCOD. Limited clinical trials and prospective controlled trials suggest intranasal corticosteroids and oral corticosteroids may alleviate symptoms.
| Level 6 |
This narrative review aims to provide information on prolonged COVID-19 symptoms in recovered patients, and their implications during dental management.
Although COVID-19 is an infectious disease primarily affecting the lungs, its multi-organ involvement is responsible for several prolonged symptoms, including oral implications. In recovered patients with prolonged COVID-19 symptoms, considerations for providing dental treatment has to be made as they can present with an assortment of symptoms. These prolonged post-COVID-19 symptoms can affect the delivery of required dental treatment. The authors’ recommendations can be a useful starting point to aid dental teams providing adequate care for such recovered patients.
| Level 6 |
Patients with COVID-19 have become known to present with different oral symptoms. However, xerostomia remains poorly recognized compared with taste dysfunction. For better understanding of COVID-19 symptomatology, xerostomia associated withCOVID-19 was characterized and its possible pathogenesis was speculated by means of a narrative literature review. Results indicate that xerostomia is one of the prevalent and persistent oral symptoms associated with COVID-19. In contrast to taste dysfunction, the prevalence and persistence of xerostomia do not necessarily depend on ethnicity, age, gender, and disease severity of patients. COVID-19 xerostomia is pathogenically related to viral cellular entry-relevant protein expression, renin-angiotensin system disturbance, salivary gland inflammation, zinc deficiency, cranial neuropathy, intercurrent taste dysfunction, comorbidities, and medications. Despite a close association with COVID-19, xerostomia, dry mouth and hyposalivation tend to be overlooked (in contrast to ageusia, dysgeusia and hypogeusia). Although mouth dryness per se is not life-threating, it has an impact on the oral health-related quality of life.
Endocrinology
| Level 6 |
BANSAL et al (2022) COVID-19 and chronic fatigue syndrome: An endocrine perspective[50]
Patients recovering from COVID-19 may have persistent debilitating symptoms requiring long-term support through individually tailored cardiopulmonary and psychological rehabilitation programs. Clinicians need to be aware about the likely long-term complications and their diagnostic assessments to help identify any occult problems requiring additional help. Endocrinological evaluations should be considered as part of the armamentarium in the management of such individuals with diligent cognizance about the involvement of the hypothalamo-pituitary-adrenal (HPA) axis, adrenal and thyroid function. The authors review the literature and potential pathophysiological mechanisms involved in and related to post COVID-19 symptoms with an emphasis on endocrine function.
| Level 6 |
COVID-19 affects multiple endocrine organ systems during the disease course. Available limited data suggest that most of the biochemical endocrine dysfunctions observed during the acute phase of COVID-19 tend to improve after recovery. The authors performed a literature review on the effects of COVID-19 on the endocrine system and subsequent long-term sequelae on endocrine functions. A set of recommendations is presented regarding the endocrine follow-up of post-acute COVID-19 patients.
Endothelial Dysfunction
| Level 6 |
The authors sought to review current literature on the role of endothelial dysfunction in coronavirus disease-2019 (COVID-19) infection in terms of pathophysiology, laboratory features and markers, clinical phenotype in adults and children, as well as long COVID-19.
Accumulating evidence suggests that endothelial dysfunction may be a common denominator of severe COVID-19 in adults and children, as well as long COVID-19, implicating mutual pathophysiological pathways. This narrative review summarizes the up-to-date knowledge of endothelial dysfunction caused by COVID-19, including novel aspects of long COVID-19 and pediatric disease. This knowledge is important in order not only to understand the multi-systemic attack of COVID-19, but also to improve patient management and prognosis.
Fatigue
| Level 1 |
The objective in this systematic review and meta-analysis was to quantify the proportion of individuals experiencing fatigue and cognitive impairment 12 or more weeks following COVID-19 diagnosis, and to characterize the inflammatory correlates and functional consequences of post-COVID-19 syndrome.
Primary research articles which evaluated individuals at least 12 weeks after confirmed COVID-19 diagnosis and specifically reported on fatigue, cognitive impairment, inflammatory parameters, and/or functional outcomes were selected.
A significant proportion of individuals experience persistent fatigue and/or cognitive impairment following resolution of acute COVID-19. The frequency and debilitating nature of the foregoing symptoms provides the impetus to characterize the underlying neurobiological substrates and how to best treat these phenomena.
| Level 6 |
SANDLER et al (2021) Long COVID and Post-infective Fatigue Syndrome: A Review[54]
Fatigue is a dominant feature of both acute and convalescent coronavirus disease 2019 (COVID-19) (sometimes termed “long-COVID”), with up to 46% of patients reporting fatigue that lasts from weeks to months. The investigators of the international Collaborative on Fatigue Following Infection (COFFI) conducted a systematic review of post-COVID fatigue and a narrative review on fatigue after other infections, and made recommendations for clinical and research approaches to assessing fatigue after COVID-19. In the majority of COVID-19 cohort studies, persistent fatigue was reported by a significant minority of patients, ranging from 13% to 33% at 16-20 weeks post-symptom onset. Data from the prospective cohort studies in COFFI and others indicate that fatigue is also a prevalent outcome from many acute systemic infections, notably infectious mononucleosis, with a case rate for clinically significant post-infective fatigue after exclusion of recognized medical and psychiatric causes, ranging from 10%-35% at 6 months. To better characterize post-COVID fatigue, the COFFI investigators recommend the following: application of validated screening questionnaires for case detection; standardized interviews encompassing fatigue, mood, and other symptoms; and investigative approaches to identify end-organ damage and mental health conditions.
Gastrointestinal
| Level 1 |
YUSUF et al (2021) Global prevalence of prolonged gastrointestinal symptoms in COVID-19 survivors and potential pathogenesis: A systematic review and meta-analysis[55]
This study aimed to determine the cumulative prevalence of prolonged gastrointestinal (GI) symptoms, including nausea, vomiting, diarrhea, lack of appetite, abdominal pain, and dysgeusia, in survivors of both mild and severe COVID-19 worldwide and to discuss the potential pathogenesis.
The global prevalence of prolonged nausea was 3.23% (95% CI: 0.54%-16.53%) among 527 COVID-19 survivors. Vomiting persisted in 93 of 2,238 COVID-19 survivors (3.19%, 95% CI: 1.62%-6.17%) and prolonged diarrhea was found in 34 of 1,073 survivors (4.12%, 95% CI: 1.07%-14.64%). A total of 156 patients among 2,238 COVID-19 survivors (4.41%, 95% CI: 1.91%-9.94%) complained of persistent decreased or loss of appetite. The cumulative prevalence of prolonged abdominal pain was 1.68% (95% CI: 0.84%-3.32%), whereas persistent dysgeusia was identified in 130 cases among 1,887 COVID-19 survivors (7.04%, 95% CI: 5.96%-8.30%). Data was insufficient to assess the relationship between COVID-19 severity and the occurrence of all prolonged GI symptoms.
Headache
| Level 1 |
The aim of this pooled analysis was to synthesize the prevalence of post-COVID headache in hospitalized and non-hospitalized patients recovering from SARS-CoV-2 infection. Random effects models were used for meta-analytical pooled prevalence of post-COVID headache. Data synthesis was categorized at hospital admission or symptoms’ onset, and at 30, 60, 90, and ≥180 days afterwards.
From 9573 studies identified, 28 peer-reviewed studies and 7 preprints were included. The sample was 28,438 COVID-19 survivors (12,307 females; mean age: 46.6, SD: 17.45 years). The methodological quality was high in 45% of the studies. The overall prevalence of post-COVID headache was 47.1% (95% CI 35.8-58.6) at onset or hospital admission, 10.2% (95% CI 5.4-18.5) at 30 days, 16.5% (95% CI 5.6-39.7) at 60 days, 10.6% (95% CI 4.7-22.3) at 90 days, and 8.4% (95% CI 4.6-14.8) at ≥180 days after onset/hospital discharge. Headache as a symptom at the acute phase was more prevalent in non-hospitalized (57.97%) than in hospitalized (31.11%) patients. Time trend analysis showed a decreased prevalence from the acute symptoms’ onset to all post-COVID follow-up periods which was maintained afterwards.
Mental Health
| Level 1 |
BOURMISTROVA et al (2022) Long-term effects of COVID-19 on mental health: A systematic review[57]
A systematic review was conducted to investigate the effect of COVID-19 infection on long-term mental health outcomes. Three databases (PubMed, Medline (Ovid) and Cochrane library) were searched between 1st October 2019 and 29th August 2021 to identify all published studies reporting symptoms of generalised anxiety, depression, post-traumatic stress disorder (PTSD), or sleep disturbance in participants at least one month after COVID-19 infection. The prevalence and mean symptom score of each were assessed.
Eight hundred and eighty five studies were found, of which 33 were included in the review involving a total of 6743 participants. The studies’ risk of bias were typically fair quality. Sleep disturbances (primarily insomnia) were most commonly reported as mild. PTSD prevalence was similar to anxiety and depression.
The overall effect of the pandemic has been linked with worsening psychiatric symptoms. However, the long-term effect from direct COVID-19 infection has been associated with no or mild symptoms. Studies exhibited the long-term prevalence of anxiety, depression, PTSD, and sleep disturbances to be comparable to general population levels.
| Level 1 |
Although depressive symptoms in the acute phase of COVID-19 have been well characterized, the frequency of depression following recovery of the acute phase remains unknown. The authors conducted a systematic review in which frequency and factors associated with depression in post-COVID-19 syndrome were recorded and qualitatively assessed through narrative synthesis.
The frequency of depressive symptoms +12 weeks following SARS-CoV-2 infection ranged from 11% to 28%. The frequency of clinically-significant depression and/or severe depressive symptoms ranged from 3% to 12%. The severity of acute COVID-19 was not associated with the frequency of depressive symptoms. Future research should endeavour to produce a standardized classification of post-COVID-19 syndrome, and as well as include unexposed control groups.
| Level 1 |
COVID-19 impacts multiple organ systems and is associated with high rates of morbidity and mortality. This systematic review aims to synthesize available literature on psychiatric and cognitive characteristics of community-dwelling survivors of COVID-19 infection.
Thirty-three studies met inclusion/exclusion criteria for review. Emerging findings link COVID-19 to cognitive deficits, particularly attention, executive function, and memory. Psychiatric symptoms occur at high rates in COVID-19 survivors, including anxiety, depression, fatigue, sleep disruption, and to a lesser extent posttraumatic stress. Symptoms appear to endure, and severity of acute illness is not directly predictive of severity of cognitive or mental health issues. The course of cognitive and psychiatric sequelae is limited by lack of longitudinal data at this time. Although heterogeneity of study design and sociocultural differences limit definitive conclusions, emerging risk factors for psychiatric symptoms include female sex, perceived stigma related to COVID-19, infection of a family member, social isolation, and prior psychiatry history.
The extant literature elucidates treatment targets for cognitive and psychosocial interventions. Research using longitudinal, prospective study designs is needed to characterize cognitive and psychiatric functioning of COVID-19 survivors over the course of illness and across illness severity. Emphasis on delineating the unique contributions of premorbid functioning, viral infection, co-morbidities, treatments, and psychosocial factors to cognitive and psychiatric sequelae of COVID-19 is warranted.
Musculoskeletal
| Level 1 |
The aim of this systematic review and meta-analysis was to synthesize the prevalence of post-coronavirus disease (COVID) pain symptoms of musculoskeletal origin in hospitalized or nonhospitalized patients recovered from SARS-CoV-2 infection. Studies or preprints reporting data on post-COVID pain symptoms such as myalgias, arthralgias, or chest pain after SARS-CoV-2 infection and collected by personal, telephonic, or electronical interview were included. Random-effects models were used for meta-analytical pooled prevalence of each post-COVID musculoskeletal pain symptom. Data synthesis was categorized at onset or hospital admission and at 30, 60, and 90, and ≥180 days after. From a total of 12,123 studies identified, 27 peer-reviewed studies and 6 preprints were included. The sample included 14,639 hospitalized and 11,070 nonhospitalized COVID-19 patients. The methodological quality of almost 70% studies was fair. The overall prevalence of post-COVID myalgia, joint pain, and chest pain ranged from 5.65% to 18.15%, 4.6% to 12.1%, and 7.8% to 23.6%, respectively, at different follow-up periods during the first year post-infection. Time trend analysis showed a decrease prevalence of musculoskeletal post-COVID pain from the symptom’s onset to 30 days after, an increase 60 days after, but with a second decrease ≥180 days after.
This meta-analysis shows that almost 10% of individuals infected by SARS-CoV-2 will suffer from musculoskeletal post-COVID pain symptomatology at some time during the first year after the infection.
Neurological
| Level 1 |
Molecular imaging techniques such as positron emission tomography (PET) and single-photon emission computed tomography (SPECT) have been used to shed light on how COVID-19 affects the human brain. The authors provide a systematic review that summarizes the current literature according to five predominant topics: 1. case reports suggest reversible cortical and subcortical metabolic alterations in rare cases with concomitant, para- or post-infectious encephalitis; 2. imaging findings in single patients with first manifestations of Parkinsonism in the context of COVID-19 resemble those in neurodegenerative Parkinsonism (loss of nigrostriatal integrity), but scarceness of data and a lack of follow-up preclude further etiological conclusions; 3. several case reports and a small number of systematic studies addressed focal symptoms and lesions, most notably hyposmia, with variable results, although some studies found regional hypometabolism of regions related to olfaction; 4. a case series and several systematic studies in inpatients with COVID-19-related encephalopathy consistently found a frontoparietal-dominant neocortical dysfunction that proved to be grossly reversible in the majority of cases until 6 months; 5. studies in “post-COVID-19 syndrome” provided controversial results. In patients with a high level of self-reported complaints such as fatigue, memory impairment, hyposmia, and dyspnea, some authors found extensive areas of limbic and subcortical hypometabolism, while others found no metabolic alterations on PET and no or only minor cognitive impairments on neuropsychological assessment.
| Level 1 |
In this meta-analysis, the authors report the characteristics of patients who experience neurological or neuropsychiatric symptoms at least 12 weeks after COVID-19 infection. They determine the pooled prevalence of these symptoms in community, hospital, ICU admitted groups 12- weeks post infection.
Of the patients included, 41% were male with average age of 56.5 years. Hypertension was the most frequent comorbidity in both the hospitalised and community groups, followed by diabetes. Anosmia, ageusia and headache were key features of acute phase COVID-19 (50.9%, 44.6%, 47.9% respectively). The symptoms of post COVID-19 syndrome were not similarly distributed, post exertional malaise (73.3%), fatigue (43.5%), brain fog (35.1%), memory issues (31.4%), headache (20.2%) and anosmia (11.4%) were most frequent. Generally, the frequency of neurological and neuropsychiatric symptoms in the hospitalised cohort was lower than in the community. In cohorts where 20% or more patients were admitted to the ICU, all neurological and neuropsychiatric symptoms were more prevalent than those in community. There was a notable increase in the prevalence of neurological symptoms after 26 weeks compared to the 12-26-week period. Cohort studies that employ risk factor analysis and 12- 26 week follow up are required to verify the trends identified.
| Level 6 |
AL-RAMADAN et al (2021) Acute and Post-Acute Neurological Complications of COVID-19[63]
Accumulating evidence indicates that COVID-19 patients commonly develop neurological symptoms such as headache, altered mental status, anosmia, and myalgia. The authors have summarized the most common neurological complications and reported neurological case studies associated with COVID-19, and neurological side effects associated with COVID-19 treatments. Additionally, the post-acute COVID-19 syndrome and long-term neurological complications were discussed.
| Level 6 |
The authors report that COVID-19 viral caustive agent, SARS-CoV-2, has a high affinity for human angiotensin-converting enzyme 2 receptor on type II pneumocytes. This receptor is also expressed in neurons and glial cells. Based on the foregoing and other not so clear mechanisms, it is stated that SARS-CoV-2 has tropism for the nervous system, being evident through the neurological manifestations observed in patients with mild, moderate and severe phenotype of the disease such as anosmia, ageusia, headache, cerebrovascular accidents, Guillain-Barré syndrome, seizures, and encephalopathy. This can generate severe sequelae and even fatal outcomes in those affected.
Neurological complications caused by COVID-19 are frequent and represent a risk that compromises the functional capacity and the life of patients. The suspicion of these conditions, the strict control of metabolic alterations and cardiovascular risk factors, the effective and safe treatment of these entities, are a current challenge throughout the pandemic. The rehabilitation process in these patients is a challenge. This is due to the limitations generated by multi-organ damage, as well as risk of brain death.
| Level 6 |
A systematic overview of current reviews of neurological symptoms of COVID-19 was conducted. The implications of these findings are discussed in relation to the potential effect on neurological services and the similarities in the experience of patients with COVID-19 and those with other neurological disorders. A total of 45 systematic reviews were identified within seven databases, published between 11 April 2020 and 15 October 2020, following a search in June 2020, updated on 20 October 2020.
The results indicate that COVID-19 exhibits two types of neurological symptoms: life-threatening symptoms such as Guillain-Barre Syndrome (GBS) and encephalitis, and less devastating symptoms such as fatigue and myalgia. Many of these so-called lesser symptoms appear to be emerging as longer-term for some sufferers and have been recently labelled long COVID. When compared, these less devastating symptoms are very similar to other neurological conditions such as chronic fatigue syndrome (CFS) and functional neurological disorder (FND).
Respiratory
| Level 1 |
Knowledge on the sequelae of Coronavirus Disease 2019 (COVID-19) remains limited due to the relatively recent onset of this pathology. However, the literature on other types of coronavirus infections prior to COVID-19 reports that patients may experience persistent symptoms after discharge. To determine the prevalence of respiratory symptoms in survivors of hospital admission after COVID-19 infection, a living systematic review was performed in order to identify studies which reported the persistence of respiratory symptoms in COVID-19 patients after discharge. Of the 1,154 reports returned by the initial search, 9 articles were found, in which 1,816 patients were included in the data synthesis. In the pooled analysis, a prevalence of 0.52 was found (CI 0.38-0.66, p < 0.01, I 2 = 97%), 0.37 (CI 0.28-0.48, p < 0.01, I 2 = 93%), 0.16 (CI 0.10-0.23, p < 0.01, I 2 = 90%) and 0.14 (CI 0.06-0.24, p < 0.01, I 2 = 96%) for fatigue, dyspnoea, chest pain, and cough, respectively. Fatigue, dyspnoea, chest pain, and cough were the most prevalent respiratory symptoms found in 52%, 37%, 16% and 14% of patients between 3 weeks and 3 months, after discharge in survivors of hospital admission by COVID-19, respectively.
Rheumatology
| Level 6 |
SAPKOTA et al (2022) Long COVID from rheumatology perspective – a narrative review[67]
Long-term sequelae of acute COVID-19, commonly referred to as long COVID, has affected millions of patients worldwide. Long COVID patients display persistent or relapsing and remitting symptoms that include fatigue, breathlessness, cough, myalgia, arthralgia, sleep disturbance, cognitive impairment and skin rashes. Due to the shared clinical features, laboratory and imaging findings, long COVID could mimic rheumatic disease, posing a diagnostic challenge. Our comprehensive literature review will help rheumatologist to be aware of long COVID manifestations and differentiating features from rheumatic diseases to ensure a timely and correct diagnosis is reached.
Sexual Health
| Level 6 |
Symptoms of long COVID are highly prevalent and involve almost all systems of the human body, with a plethora of clinical manifestations which range from minor nuisances to life-threatening conditions. Brain fog and fatigue are the most common complaints, although other neuropsychiatric complications, including sensory dysfunctions, anxiety, depression, and cerebrovascular events have also been reported. The respiratory and cardiovascular systems are also affected, with dyspnea, pulmonary fibrosis, endothelial dysfunction, and myocarditis occurring in some COVID long haulers. A subset of patients might develop endocrine manifestations, including onset of diabetes, thyroid dysfunction, and hypogonadism. Overall, long COVID features many complications which can impair erectile function by multiple pathogenetic mechanisms, and which could require tailored treatment: careful investigation and management from the sexual medicine expert are therefore much needed, and future research on this topic is warranted.
CONCLUSION: in COVID-19 long haulers, several complications can adversely affect erectile function which, upon future tailored studies, could be used as biomarker for the severity of the long COVID disease and for its follow-up.
Thrombosis
| Level 1 |
This systematic review and meta-analysis was conducted to better understand the incidence of thrombosis, bleeding, and mortality rates among patients discharged after COVID-19 hospitalization.
Twenty articles were included in the meta-analysis. They provided a total of 19,461 patients discharged after COVID-19 hospitalization. The weighted pooled incidence of overall thrombosis among the patients was 1.3% (95 CI, 0. 6-2; I2 90.5), with a pooled incidence of venous thrombosis of 0.7% (95 CI, 0. 4-1; I2 73.9), and a pooled incidence of arterial thrombosis of 0.6% (95 CI, 0. 2-1; I2 88.1). The weighted pooled incidences of bleeding and mortality were 0.9% (95 CI, 0. 1-1.9; I2 95.1) and 2.8% (95 CI, 0. 6-5; I2 98.2), respectively.
The incidences of thrombosis and bleeding in patients discharged after COVID-19 hospitalization are comparable to those of medically ill patients.
Paediatric
| Level 1 |
Data on the long-term impact of SARS-CoV-2 infection in children and young people (CYP) are conflicting. Evidence on long-term post-COVID symptoms in CYP examining prevalence, risk factors, type and duration were assessed.
Twenty two studies were included in this meta-analysis, including 23,141 CYP. Median duration of follow-up was 125 days (IQR 99-231). Pooled risk difference in post-COVID cases compared to controls (5 studies) were significantly higher for cognitive difficulties (3% (95% CI 1, 4)), headache (5% (1, 8)), loss of smell (8%, (2, 15)), sore throat (2% (1, 2)), and sore eyes (2% (1, 3)), but not abdominal pain, cough, fatigue, myalgia, insomnia, diarrhoea, fever, dizziness or dyspnoea. Pooled prevalence of symptoms in post-COVID participants in 17 studies ranged from 15% (diarrhoea) to 47% (fatigue). Age was associated with higher prevalence of all symptoms except cough. Higher study quality was associated with lower prevalence of all symptoms, except loss of smell and cognitive symptoms.
The frequency of the majority of reported persistent symptoms was similar in SARS-CoV-2 positive cases and controls. This systematic review and meta-analysis highlights the critical importance of a control group in studies on CYP post SARS-CoV-2 infection.
| Level 6 |
The few studies that have documented long-term physical symptoms in children show that fatigue, difficulty in concentrating (brain fog), sleep disturbances, and sensory problems are the most reported outcomes. Most studies examining the impact of COVID-19 in pediatric populations have focused on initial clinical presentation, and symptoms, which are similar to those in adult populations. In addition, COVID-19 has had a moderate impact on children and adolescents’ social environment, which may exacerbate current and future physiological, psychological, behavioral, and academic outcomes.
There are limited studies reporting long physical symptoms of COVID-19 in the pediatric population. However, pediatric COVID-19 cases are underreported due to low rates of testing and symptomatic infection, which calls for more longitudinal studies. Children who have experienced COVID-19 illness should be monitored for long physiological, psychological, behavioral, and academic outcomes.
| Level 6 |
Compared to adults, post-COVID-19 symptoms are uncommon and have not been thoroughly evaluated in children. This review summarizes the literature in terms of persistent symptoms in children and adolescents after SARS-CoV-2 infection.
Children were less likely to develop long COVID when compared to adults. Older children and those who had symptomatic COVID-19 had a higher probability for long COVID.
Families and health care providers need to be aware of a new constellation of long COVID symptoms in the pediatric population. More evidence and time are needed to better understand the potential effects of long COVID-19 in children and adolescents. In comparison to adults, children are less likely to have persistent COVID-19 symptoms.
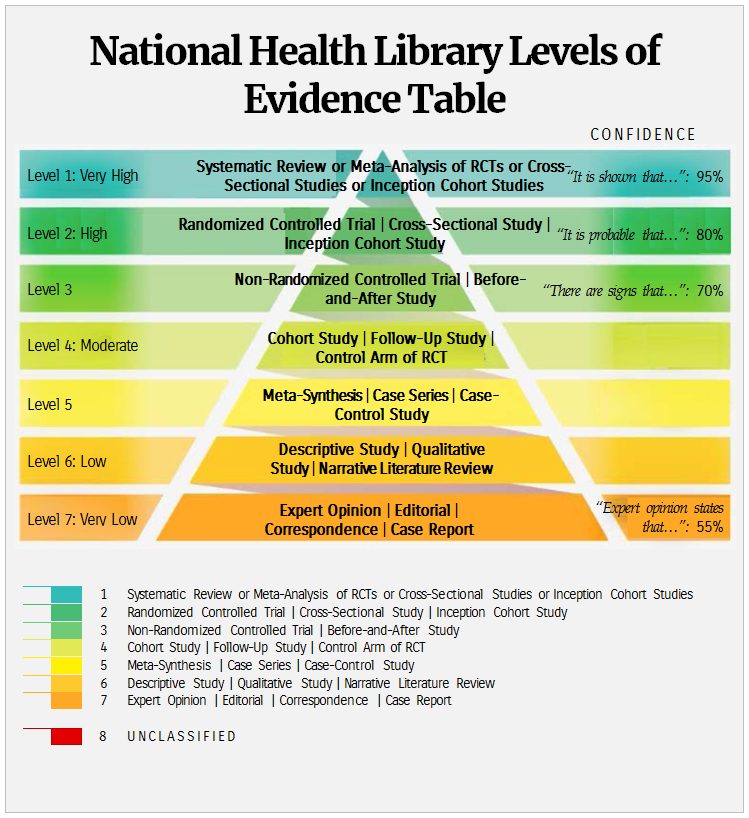
References
[1] World Health Organisation (2021) Living guidance for clinical management of COVID-19. https://www.who.int/publications/i/item/WHO-2019-nCoV-clinical-2021-2. Accessed 24/03/2022.
[2] Centers for Disease Control and Prevention (2021) Post-COVID conditions: information for Healthcare Providers https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-care/post-COVID-conditions.html. Accessed 24/03/2022.
[3] Centers for Disease Control and Prevention (2021) Evaluating and Caring for Patients with Post-COVID Conditions: Interim Guidance. https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-care/post-COVID-index.html. Accessed 24/03/2022.
[4] National Institute of Health and Care Excellence (Great Briain) (2021) COVID-19 rapid guideline: managing the long-term effects of COVID-19. Published: 18 December 2020 Last updated: 11 November 2021. https://www.nice.org.uk/guidance/ng188. Accessed 24/03/2022.
[5] Scottish Intercollegiate Guidelines Newtork (2021) Managing the long-term effects of COVID-19. https://www.sign.ac.uk/our-guidelines/managing-the-long-term-effects-of-COVID-19/. Accessed 24/03/2022.
[6] BMJ Best Practice (2022) Coronavirus disease 2019 (COVID-19): Complications – post-COVID-19 syndrome (Long COVID). https://bestpractice.bmj.com/topics/en-gb/3000201/complications#referencePop1133. Accessed 24/03/2022.
[7] UpToDate (2022) COVID-19: Evaluation and management of adults following acute viral illness: persistent symptoms. https://www.uptodate.com/contents/COVID-19-evaluation-and-management-of-adults-following-acute-viral-illness? Accessed 24/03/2022.
[8] Alkodaymi MS, Omrani OA, Fawzy NA, Shaar BA, Almamlouk R, Riaz M, Obeidat M, Obeidat Y, Gerberi D, Taha RM, Kashour Z, Kashour T, Berbari EF, Alkattan K, Tleyjeh IM. Prevalence of post-acute COVID-19 syndrome symptoms at different follow-up periods: A systematic review and meta-analysis. Clin Microbiol Infect. 2022 Feb 3:S1198-743X(22)00038-6. doi: 10.1016/j.cmi.2022.01.014. Epub ahead of print. PMID: 35124265; PMCID: PMC8812092.
[9] d’Ettorre G, Gentilini Cacciola E, Santinelli L, De Girolamo G, Spagnolello O, Russo A, Tarsitani L, Ciccozzi M, Mastroianni CM, d’Ettorre G, Ceccarelli G. COVID-19 sequelae in working age patients: A systematic review. J Med Virol. 2021 Oct 16:10.1002/jmv.27399. doi: 10.1002/jmv.27399. Epub ahead of print. PMID: 34655247; PMCID: PMC8661973.
[10] Han Q, Zheng B, Daines L, Sheikh A. Long-Term Sequelae of COVID-19: A Systematic Review and Meta-Analysis of One-Year Follow-Up Studies on Post-COVID Symptoms. Pathogens. 2022 Feb 19;11(2):269. doi: 10.3390/pathogens11020269. PMID: 35215212; PMCID: PMC8875269.
[11] Macpherson K, Cooper K, Harbour J, Mahal D, Miller C, Nairn M. Experiences of living with long COVID and of accessing healthcare services: a qualitative systematic review. BMJ Open. 2022 Jan 11;12(1):e050979. doi: 10.1136/bmjopen-2021-050979. PMID: 35017239; PMCID: PMC8753091.
[12] Nguyen NN, Hoang VT, Dao TL, Dudouet P, Eldin C, Gautret P. Clinical patterns of somatic symptoms in patients suffering from post-acute long COVID: a systematic review. Eur J Clin Microbiol Infect Dis. 2022 Feb 10:1–31. doi: 10.1007/s10096-022-04417-4. Epub ahead of print. PMID: 35142947; PMCID: PMC8830952.
[13] Pierce JD, Shen Q, Cintron SA, Hiebert JB. Post-COVID-19 Syndrome. Nurs Res. 2022 Mar-Apr 01;71(2):164-174. doi: 10.1097/NNR.0000000000000565. PMID: 34653099.
[14] Van Kessel SAM, Olde Hartman TC, Lucassen PLBJ, van Jaarsveld CHM. Post-acute and long-COVID-19 symptoms in patients with mild diseases: a systematic review. Fam Pract. 2022 Jan 19;39(1):159-167. doi: 10.1093/fampra/cmab076. PMID: 34268556; PMCID: PMC8414057.
[15] Yelin D, Moschopoulos CD, Margalit I, Gkrania-Klotsas E, Landi F, Stahl JP, Yahav D. ESCMID rapid guidelines for assessment and management of long COVID. Clin Microbiol Infect. 2022 Feb 16:S1198-743X(22)00092-1. doi: 10.1016/j.cmi.2022.02.018. Epub ahead of print. PMID: 35182760; PMCID: PMC8849856.
[16] Ahmad MS, Shaik RA, Ahmad RK, Yusuf M, Khan M, Almutairi AB, Alghuyaythat WKZ, Almutairi SB. “LONG COVID”: an insight. Eur Rev Med Pharmacol Sci. 2021 Sep;25(17):5561-5577. doi: 10.26355/eurrev_202109_26669. PMID: 34533807.
[17] Aiyegbusi OL, Hughes SE, Turner G, Rivera SC, McMullan C, Chandan JS, Haroon S, Price G, Davies EH, Nirantharakumar K, Sapey E, Calvert MJ; TLC Study Group. Symptoms, complications and management of long COVID: a review. J R Soc Med. 2021 Sep;114(9):428-442. doi: 10.1177/01410768211032850. Epub 2021 Jul 15. PMID: 34265229; PMCID: PMC8450986.
[18] Akbarialiabad H, Taghrir MH, Abdollahi A, Ghahramani N, Kumar M, Paydar S, Razani B, Mwangi J, Asadi-Pooya AA, Malekmakan L, Bastani B. Long COVID, a comprehensive systematic scoping review. Infection. 2021 Dec;49(6):1163-1186. doi: 10.1007/s15010-021-01666-x. Epub 2021 Jul 28. PMID: 34319569; PMCID: PMC8317481.
[19] Anaya JM, Rojas M, Salinas ML, Rodríguez Y, Roa G, Lozano M, Rodríguez-Jiménez M, Montoya N, Zapata E; Post-COVID study group, Monsalve DM, Acosta-Ampudia Y, Ramírez-Santana C. Post-COVID syndrome. A case series and comprehensive review. Autoimmun Rev. 2021 Nov;20(11):102947. doi: 10.1016/j.autrev.2021.102947. Epub 2021 Sep 10. PMID: 34509649; PMCID: PMC8428988.
[20] Cabrera Martimbianco AL, Pacheco RL, Bagattini ÂM, Riera R. Frequency, signs and symptoms, and criteria adopted for long COVID-19: A systematic review. Int J Clin Pract. 2021 Oct;75(10):e14357. doi: 10.1111/ijcp.14357. Epub 2021 Jun 2. PMID: 33977626; PMCID: PMC8236920.
[21] Cha C, Baek G. Symptoms and management of long COVID: A scoping review. J Clin Nurs. 2021 Dec 15. doi: 10.1111/jocn.16150. Epub ahead of print. PMID: 34913540.
[22] Chen Chen, Spencer Haupert, Lauren Zimmermann, Xu Shi, Lars G. Fritsche, Bhramar Mukherjee Global Prevalence of Post-Acute Sequelae of COVID-19 (PASC) or Long COVID: A Meta-Analysis and Systematic Review. medRxiv 2021.11.15.21266377; doi: https://doi.org/10.1101/2021.11.15.21266377[23]Simon Décary, Michèle Dugas, Théo Stefan, Léa Langlois, Becky Skidmore, Anne Bhéreur, Annie LeBlanc, Alberta Health Services, Stephanie Hastings, Branden Manns, Lynora Saxinger. Care Models for Long COVID: A Rapid Systematic Review. medRxiv 2021.11.17.21266404; doi: https://doi.org/10.1101/2021.11.17.21266404
[24] Fernández-de-Las-Peñas C, Palacios-Ceña D, Gómez-Mayordomo V, Florencio LL, Cuadrado ML, Plaza-Manzano G, Navarro-Santana M. Prevalence of post-COVID-19 symptoms in hospitalized and non-hospitalized COVID-19 survivors: A systematic review and meta-analysis. Eur J Intern Med. 2021 Oct;92:55-70. doi: 10.1016/j.ejim.2021.06.009. Epub 2021 Jun 16. PMID: 34167876; PMCID: PMC8206636.
[25] Garg M, Maralakunte M, Garg S, Dhooria S, Sehgal I, Bhalla AS, Vijayvergiya R, Grover S, Bhatia V, Jagia P, Bhalla A, Suri V, Goyal M, Agarwal R, Puri GD, Sandhu MS. The Conundrum of ‘Long-COVID-19’: A Narrative Review. Int J Gen Med. 2021 Jun 14;14:2491-2506. doi: 10.2147/IJGM.S316708. PMID: 34163217; PMCID: PMC8214209.
[26] Hayes LD, Ingram J, Sculthorpe NF. More Than 100 Persistent Symptoms of SARS-CoV-2 (Long COVID): A Scoping Review. Front Med (Lausanne). 2021 Nov 1;8:750378. doi: 10.3389/fmed.2021.750378. PMID: 34790680; PMCID: PMC8591053.
[27] Iqbal FM, Lam K, Sounderajah V, Clarke JM, Ashrafian H, Darzi A. Characteristics and predictors of acute and chronic post-COVID syndrome: A systematic review and meta-analysis. EClinicalMedicine. 2021 May 24;36:100899. doi: 10.1016/j.eclinm.2021.100899. PMID: 34036253; PMCID: PMC8141371.
[28] Iwu CJ, Iwu CD, Wiysonge CS. The occurrence of long COVID: a rapid review. Pan Afr Med J. 2021 Jan 20;38:65. doi: 10.11604/pamj.2021.38.65.27366. PMID: 33889231; PMCID: PMC8028365.
[29] Jennings G, Monaghan A, Xue F, Mockler D, Romero-Ortuño R. A Systematic Review of Persistent Symptoms and Residual Abnormal Functioning following Acute COVID-19: Ongoing Symptomatic Phase vs. Post-COVID-19 Syndrome. J Clin Med. 2021 Dec 16;10(24):5913. doi: 10.3390/jcm10245913. PMID: 34945213; PMCID: PMC8708187.
[30] Leviner S. Recognizing the Clinical Sequelae of COVID-19 in Adults: COVID-19 Long-Haulers. J Nurse Pract. 2021 Sep;17(8):946-949. doi: 10.1016/j.nurpra.2021.05.003. Epub 2021 May 7. PMID: 33976591; PMCID: PMC8103144.
[31] Long Q, Li J, Hu X, Bai Y, Zheng Y, Gao Z. Follow-Ups on Persistent Symptoms and Pulmonary Function Among Post-Acute COVID-19 Patients: A Systematic Review and Meta-Analysis. Front Med (Lausanne). 2021 Sep 3;8:702635. doi: 10.3389/fmed.2021.702635. PMID: 34540862; PMCID: PMC8448290.
[32] Lopez-Leon S, Wegman-Ostrosky T, Perelman C, Sepulveda R, Rebolledo PA, Cuapio A, Villapol S. More than 50 long-term effects of COVID-19: a systematic review and meta-analysis. Sci Rep. 2021 Aug 9;11(1):16144. doi: 10.1038/s41598-021-95565-8. PMID: 34373540; PMCID: PMC8352980.
[33] Malik P, Patel K, Pinto C, Jaiswal R, Tirupathi R, Pillai S, Patel U. Post-acute COVID-19 syndrome (PCS) and health-related quality of life (HRQoL)-A systematic review and meta-analysis. J Med Virol. 2022 Jan;94(1):253-262. doi: 10.1002/jmv.27309. Epub 2021 Sep 7. PMID: 34463956; PMCID: PMC8662132.
[34] Michelen M, Manoharan L, Elkheir N, Cheng V, Dagens A, Hastie C, O’Hara M, Suett J, Dahmash D, Bugaeva P, Rigby I, Munblit D, Harriss E, Burls A, Foote C, Scott J, Carson G, Olliaro P, Sigfrid L, Stavropoulou C. Characterising long COVID: a living systematic review. BMJ Glob Health. 2021 Sep;6(9):e005427. doi: 10.1136/bmjgh-2021-005427. PMID: 34580069; PMCID: PMC8478580.
[35] Nasserie T, Hittle M, Goodman SN. Assessment of the Frequency and Variety of Persistent Symptoms Among Patients With COVID-19: A Systematic Review. JAMA Netw Open. 2021 May 3;4(5):e2111417. doi: 10.1001/jamanetworkopen.2021.11417. PMID: 34037731; PMCID: PMC8155823.
[36] Patrucco F, Zeppegno P, Baricich A, Gramaglia CM, Balbo PE, Falaschi Z, Carriero A, Cuneo D, Pirisi M, Bellan M. Long-lasting consequences of Coronavirus disease 19 pneumonia: a systematic review. Minerva Med. 2021 Dec 3. doi: 10.23736/S0026-4806.21.07594-7. Epub ahead of print. PMID: 34856780.
[37] Poudel AN, Zhu S, Cooper N, Roderick P, Alwan N, Tarrant C, Ziauddeen N, Yao GL. Impact of COVID-19 on health-related quality of life of patients: A structured review. PLoS One. 2021 Oct 28;16(10):e0259164. doi: 10.1371/journal.pone.0259164. PMID: 34710173; PMCID: PMC8553121.
[38] Proal AD, VanElzakker MB. Long COVID or Post-acute Sequelae of COVID-19 (PASC): An Overview of Biological Factors That May Contribute to Persistent Symptoms. Front Microbiol. 2021 Jun 23;12:698169. doi: 10.3389/fmicb.2021.698169. PMID: 34248921; PMCID: PMC8260991.
[39] Pye A, Roberts SR, Blennerhassett A, Iqbal H, Beenstock J, Iqbal Z. A public health approach to estimating the need for long COVID services. J Public Health (Oxf). 2021 Oct 14:fdab365. doi: 10.1093/pubmed/fdab365. Epub ahead of print. PMID: 34651183.
[40] Soriano-Moreno AN, Soriano-Moreno DR, Pacheco-Barrios N, Lescano AG, Checkley W. A Systematic Review of the Frequency of Persistent Constitutional and Respiratory Symptoms Related to COVID-19: A New Long COVID Syndrome? Am J Respir Crit Care Med. 2021; 203:A3795. https://doi.org/10.1164/ajrccm-conference.2021.203.1_MeetingAbstracts.A3795
[41] Tucci V, Saary J. Persistent and Emergent Clinical Sequelae of Mild COVID-19. Aerosp Med Hum Perform. 2021 Dec 1;92(12):962-969. doi: 10.3357/AMHP.5892.2021. PMID: 34986935.
[42] Willi S, Lüthold R, Hunt A, Hänggi NV, Sejdiu D, Scaff C, Bender N, Staub K, Schlagenhauf P. COVID-19 sequelae in adults aged less than 50 years: A systematic review. Travel Med Infect Dis. 2021 Mar-Apr;40:101995. doi: 10.1016/j.tmaid.2021.101995. Epub 2021 Feb 22. PMID: 33631340; PMCID: PMC7898978.
[43] Wu L, Wu Y, Xiong H, Mei B, You T. Persistence of Symptoms After Discharge of Patients Hospitalized Due to COVID-19. Front Med (Lausanne). 2021 Nov 22;8:761314. doi: 10.3389/fmed.2021.761314. PMID: 34881263; PMCID: PMC8645792.
[44] Chilazi M, Duffy EY, Thakkar A, Michos ED. COVID and Cardiovascular Disease: What We Know in 2021. Curr Atheroscler Rep. 2021 May 13;23(7):37. doi: 10.1007/s11883-021-00935-2. PMID: 33983522; PMCID: PMC8117457.
[45] Sarfraz Z, Sarfraz A, Barrios A, Garimella R, Dominari A, Kc M, Pandav K, Pantoja JC, Retnakumar V, Cherrez-Ojeda I. Cardio-Pulmonary Sequelae in Recovered COVID-19 Patients: Considerations for Primary Care. J Prim Care Community Health. 2021 Jan-Dec;12:21501327211023726. doi: 10.1177/21501327211023726. PMID: 34096390; PMCID: PMC8188976.
[46] France K, Glick M. Long COVID and oral health care considerations. J Am Dent Assoc. 2022 Feb;153(2):167-174. doi: 10.1016/j.adaj.2021.08.007. Epub 2021 Oct 29. PMID: 34756590; PMCID: PMC8553648.
[47] Wu TJ, Yu AC, Lee JT. Management of post-COVID-19 olfactory dysfunction. Curr Treat Options Allergy. 2022 Jan 4:1-18. doi: 10.1007/s40521-021-00297-9. Epub ahead of print. PMID: 35004126; PMCID: PMC8723803.
[48] Chakraborty T, Jamal RF, Battineni G, Teja KV, Marto CM, Spagnuolo G. A Review of Prolonged Post-COVID-19 Symptoms and Their Implications on Dental Management. Int J Environ Res Public Health. 2021 May 12;18(10):5131. doi: 10.3390/ijerph18105131. PMID: 34066174; PMCID: PMC8151698.
[49] Tsuchiya H. Characterization and Pathogenic Speculation of Xerostomia Associated with COVID-19: A Narrative Review. Dent J (Basel). 2021 Nov 10;9(11):130. doi: 10.3390/dj9110130. PMID: 34821594; PMCID: PMC8625834.
[50] Bansal R, Gubbi S, Koch CA. COVID-19 and chronic fatigue syndrome: An endocrine perspective. J Clin Transl Endocrinol. 2022 Mar;27:100284. doi: 10.1016/j.jcte.2021.100284. Epub 2021 Dec 3. PMID: 34877261; PMCID: PMC8641402.
[51] Pal R, Joshi A, Bhadada SK, Banerjee M, Vaikkakara S, Mukhopadhyay S. Endocrine Follow-up During Post-Acute COVID-19: Practical Recommendations Based on Available Clinical Evidence. Endocr Pract. 2022 Feb 11:S1530-891X(22)00044-1. doi: 10.1016/j.eprac.2022.02.003. Epub ahead of print. PMID: 35158058; PMCID: PMC8832848.
[52] Gavriilaki, Eleni, Eftychidis, Ioannis and Papassotiriou, Ioannis. “Update on endothelial dysfunction in COVID-19: severe disease, long COVID-19 and pediatric characteristics” Journal of Laboratory Medicine, vol. 45, no. 6, 2021, pp. 293-302.
[53] Ceban F, Ling S, Lui LMW, Lee Y, Gill H, Teopiz KM, Rodrigues NB, Subramaniapillai M, Di Vincenzo JD, Cao B, Lin K, Mansur RB, Ho RC, Rosenblat JD, Miskowiak KW, Vinberg M, Maletic V, McIntyre RS. Fatigue and cognitive impairment in Post-COVID-19 Syndrome: A systematic review and meta-analysis. Brain Behav Immun. 2021 Dec 29;101:93-135. doi: 10.1016/j.bbi.2021.12.020. Epub ahead of print. PMID: 34973396; PMCID: PMC8715665.
[54] Sandler CX, Wyller VBB, Moss-Morris R, Buchwald D, Crawley E, Hautvast J, Katz BZ, Knoop H, Little P, Taylor R, Wensaas KA, Lloyd AR. Long COVID and Post-infective Fatigue Syndrome: A Review. Open Forum Infect Dis. 2021 Sep 9;8(10):ofab440. doi: 10.1093/ofid/ofab440. PMID: 34631916; PMCID: PMC8496765.
[55] Yusuf F, Fahriani M, Mamada SS, Frediansyah A, Abubakar A, Maghfirah D, Fajar JK, Maliga HA, Ilmawan M, Emran TB, Ophinni Y, Innayah MR, Masyeni S, Ghouth ASB, Yusuf H, Dhama K, Nainu F, Harapan H. Global prevalence of prolonged gastrointestinal symptoms in COVID-19 survivors and potential pathogenesis: A systematic review and meta-analysis. F1000Res. 2021 Apr 19;10:301. doi: 10.12688/f1000research.52216.1. PMID: 34131481; PMCID: PMC8171196.
[56] Fernández-de-Las-Peñas C, Navarro-Santana M, Gómez-Mayordomo V, Cuadrado ML, García-Azorín D, Arendt-Nielsen L, Plaza-Manzano G. Headache as an acute and post-COVID-19 symptom in COVID-19 survivors: A meta-analysis of the current literature. Eur J Neurol. 2021 Nov;28(11):3820-3825. doi: 10.1111/ene.15040. Epub 2021 Aug 8. PMID: 34327787; PMCID: PMC8444899.
[57] Bourmistrova NW, Solomon T, Braude P, Strawbridge R, Carter B. Long-term effects of COVID-19 on mental health: A systematic review. J Affect Disord. 2022 Feb 15;299:118-125. doi: 10.1016/j.jad.2021.11.031. Epub 2021 Nov 16. PMID: 34798148; PMCID: PMC8758130.
[58] Renaud-Charest O, Lui LMW, Eskander S, Ceban F, Ho R, Di Vincenzo JD, Rosenblat JD, Lee Y, Subramaniapillai M, McIntyre RS. Onset and frequency of depression in post-COVID-19 syndrome: A systematic review. J Psychiatr Res. 2021 Dec;144:129-137. doi: 10.1016/j.jpsychires.2021.09.054. Epub 2021 Sep 30. PMID: 34619491; PMCID: PMC8482840.
[59] Vanderlind WM, Rabinovitz BB, Miao IY, Oberlin LE, Bueno-Castellano C, Fridman C, Jaywant A, Kanellopoulos D. A systematic review of neuropsychological and psychiatric sequalae of COVID-19: implications for treatment. Curr Opin Psychiatry. 2021 Jul 1;34(4):420-433. doi: 10.1097/YCO.0000000000000713. PMID: 34016818; PMCID: PMC8183238.
[60] Fernández-de-Las-Peñas C, Navarro-Santana M, Plaza-Manzano G, Palacios-Ceña D, Arendt-Nielsen L. Time course prevalence of post-COVID pain symptoms of musculoskeletal origin in patients who had survived to severe acute respiratory syndrome coronavirus 2 infection: a systematic review and meta-analysis. Pain. 2021 Sep 23. doi: 10.1097/j.pain.0000000000002496. Epub ahead of print. PMID: 34561390.
[61] Meyer PT, Hellwig S, Blazhenets G, Hosp JA. Molecular imaging findings on acute and long-term effects of COVID-19 on the brain: A systematic review. J Nucl Med. 2022 Feb 17:jnumed.121.263085. doi: 10.2967/jnumed.121.263085. Epub ahead of print. PMID: 35177424.
[62] Premraj L, Kannapadi NV, Briggs J, Seal SM, Battaglini D, Fanning J, Suen J, Robba C, Fraser J, Cho SM. Mid and long-term neurological and neuropsychiatric manifestations of post-COVID-19 syndrome: A meta-analysis. J Neurol Sci. 2022 Jan 29;434:120162. doi: 10.1016/j.jns.2022.120162. Epub ahead of print. PMID: 35121209; PMCID: PMC8798975.
[63] Al-Ramadan A, Rabab’h O, Shah J, Gharaibeh A. Acute and Post-Acute Neurological Complications of COVID-19. Neurol Int. 2021 Mar 9;13(1):102-119. doi: 10.3390/neurolint13010010. PMID: 33803475; PMCID: PMC8006051.
[64] Camargo-Martínez W, Lozada-Martínez I, Escobar-Collazos A, Navarro-Coronado A, Moscote-Salazar L, Pacheco-Hernández A, Janjua T, Bosque-Varela P. Post-COVID 19 neurological syndrome: Implications for sequelae’s treatment. J Clin Neurosci. 2021 Jun;88:219-225. doi: 10.1016/j.jocn.2021.04.001. Epub 2021 Apr 8. PMID: 33992187; PMCID: PMC8031003.
[65] Wildwing T, Holt N. The neurological symptoms of COVID-19: a systematic overview of systematic reviews, comparison with other neurological conditions and implications for healthcare services. Ther Adv Chronic Dis. 2021 Jan 28;12:2040622320976979. doi: 10.1177/2040622320976979. PMID: 33796241; PMCID: PMC7970685.
[66] Cares-Marambio K, Montenegro-Jiménez Y, Torres-Castro R, Vera-Uribe R, Torralba Y, Alsina-Restoy X, Vasconcello-Castillo L, Vilaró J. Prevalence of potential respiratory symptoms in survivors of hospital admission after coronavirus disease 2019 (COVID-19): A systematic review and meta-analysis. Chron Respir Dis. 2021 Jan-Dec;18:14799731211002240. doi: 10.1177/14799731211002240. PMID: 33729021; PMCID: PMC7975482.
[67] Sapkota HR, Nune A. Long COVID from rheumatology perspective – a narrative review. Clin Rheumatol. 2022 Feb;41(2):337-348. doi: 10.1007/s10067-021-06001-1. Epub 2021 Nov 30. PMID: 34845562; PMCID: PMC8629735.
[68] Sansone A, Mollaioli D, Limoncin E, Ciocca G, Bắc NH, Cao TN, Hou G, Yuan J, Zitzmann M, Giraldi A, Jannini EA. The Sexual Long COVID (SLC): Erectile Dysfunction as a Biomarker of Systemic Complications for COVID-19 Long Haulers. Sex Med Rev. 2021 Nov 20:S2050-0521(21)00085-8. doi: 10.1016/j.sxmr.2021.11.001. Epub ahead of print. PMID: 34933829; PMCID: PMC8604714.
[69] Rungjirajittranon T, Owattanapanich W, Leelakanok N, Sasijareonrat N, Suwanawiboon B, Chinthammitr Y, Ruchutrakool T. Thrombotic and Hemorrhagic Incidences in Patients After Discharge from COVID-19 Infection: A Systematic Review and Meta-Analysis. Clin Appl Thromb Hemost. 2021 Jan-Dec;27:10760296211069082. doi: 10.1177/10760296211069082. PMID: 34907791; PMCID: PMC8689619.
[70] Behnood SA, Shafran R, Bennett SD, Zhang AXD, O’Mahoney LL, Stephenson TJ, Ladhani SN, De Stavola BL, Viner RM, Swann OV. Persistent symptoms following SARS-CoV-2 infection amongst children and young people: A meta-analysis of controlled and uncontrolled studies. J Infect. 2022 Feb;84(2):158-170. doi: 10.1016/j.jinf.2021.11.011. Epub 2021 Nov 20. PMID: 34813820; PMCID: PMC8604800.
[71] Borel M, Xie L, Kapera O, Mihalcea A, Kahn J, Messiah SE. Long-term physical, mental and social health effects of COVID-19 in the pediatric population: a scoping review. World J Pediatr. 2022 Feb 3:1–11. doi: 10.1007/s12519-022-00515-7. Epub ahead of print. PMID: 35118594; PMCID: PMC8812346.
[72] Thallapureddy K, Thallapureddy K, Zerda E, Suresh N, Kamat D, Rajasekaran K, Moreira A. Long-Term Complications of COVID-19 Infection in Adolescents and Children. Curr Pediatr Rep. 2022 Feb 1:1-7. doi: 10.1007/s40124-021-00260-x. Epub ahead of print. PMID: 35127274; PMCID: PMC8803461.
Produced by the members of the Health Library Ireland | Evidence service†. Current as at 14 March 2022. This evidence summary collates the best available evidence at the time of writing and does not replace clinical judgement or guidance. Emerging literature or subsequent developments in respect of COVID-19 may require amendment to the information or sources listed in the document. Although all reasonable care has been taken in the compilation of content, the Health Library Ireland | Evidence service makes no representations or warranties expressed or implied as to the accuracy or suitability of the information or sources listed in the document. This evidence summary is the property of Health Library Ireland and subsequent re-use or distribution in whole or in part should include acknowledgement of the service.
Emma Quinn, Librarian, St. Luke’s General Hospital, Kilkenny [Author]; Helen Clark, Librarian, Sligo University Hospital [Author]; Brendan Leen, Area Library Manager, HSE South [Editor]; Siobhan McCarthy, Information Specialist, Health Intelligence Unit, Strategic Planning and Transformation [Editor]

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License