
What is the current best evidence for virtual pulmonary rehabilitation for COVID-19 patients?
Download full Summary of Evidence (pdf)
The following information resources have been selected by the National Health Library and Knowledge Service Evidence Virtual Team in response to your question. The resources are listed in our estimated order of relevance to practicing healthcare professionals confronted with this scenario in an Irish context. In respect of the evolving global situation and rapidly changing evidence base, it is advised to use hyperlinked sources in this document to ensure that the information you are disseminating to the public or applying in clinical practice is the most current, valid and accurate. For further information on the methodology used in the compilation of this document – including a complete list of sources consulted – please see our National Health Library and Knowledge Service Summary of Evidence Protocol.
Summary of Evidence
Guidance
Many organisations have released guidance which describes pulmonary rehabilitation (PR) considerations for COVID-19 patients, some of which also outline modifications to PR using technology1, 2, 3, 4, 5, 6, 7, 8. Interestingly, guidance released in March 2020 from the American Thoracic Society (ATS) did not endorse a specific approach to PR during the pandemic and stated that there was insufficient evidence to support home PR alternatives. Interim guidance from the ATS and European Respiratory Society (ERS)1 released in August emphasised that COVID-19 survivors who had existing/on-going lung function impairment at 6–8 weeks following hospital discharge should receive a comprehensive PR programme consistent with established international standards. However, this guidance only mentions telerehabilitation in the context of patients who are considered potentially infectious, rather than as a standard mode of PR delivery. Similarly, the British Thoracic Society guidance on adapted delivery of PR to patients surviving COVID-193, which was released in September 2020, states: “There is no evidence that remotely supervised recovery programmes are beneficial for COVID-19 survivors.”
Quality of Studies
Many of the articles in the International Literature section would be considered low quality as they include editorials, abstracts, commentaries or studies with a small sample size, within which individual institutions share their experiences of delivering PR virtually15, 32, 17. Wootton et al.19 provide a very detailed report of their approach but they do acknowledge that theirs is a single‐centre report and that the number of cases is limited. Similarly, Finkelstein et al.16 describe a pilot study for remote assessment of exercise capacity (for PR specifically) using videoconferencing platforms. Salawu et al. (20) strongly advocate for the remote delivery of multidisciplinary rehabilitation, including PR and provide a proposed COVID-19 patient follow-up pathway. Many of the authors share their experience and opinions to endorse the remote provision of PR as feasible and safe when provided by experienced PR clinicians20, 19.However the need for high quality clinical research to strengthen the evidence base is also acknowledged14. Jain and Santhosh29 suggest that: “There is a need for studying the validity, feasibility, and efficacy of home-based monitoring and treatment tools, such as spirometry, accelerometers, and virtual PR, to allow a realistic consideration of their deployment and use in the near future.” A number of randomised control trials and systematic reviews have been identified and are ongoing, and may add to the evidence base regarding virtual PR in COVID-19 patients in the near future.
Multidisciplinary and Patient-Personalised Rehabilitation
A multidisciplinary approach to rehabilitation is widely recommended24, 32, 20, 30, 18. Salawu28 emphasises the importance of care provision for COVID-19 survivors post discharge by: hospital teams; physicians; occupational therapy; psychology; speech and language therapy; dietitians; and physiotherapists. Similarly, in the UK18 a multidisciplinary team of professionals developed a comprehensive pragmatic telephone screening tool, the COVID-19 Yorkshire Rehabilitation Screen (C19-YRS), and an integrated rehabilitation pathway, which spans the Acute Hospital Trust, Community Trust and Primary Care Service within the National Health Service (NHS) service model. This tool incorporates: respiratory medicine; community pulmonary rehabilitation; critical care; community rehabilitation; psychology; speech and language therapy; and dietetics18.
Sun12 emphasises the need for personalisation of rehabilitation: “As different patients have differing degrees of dysfunction, personalized plans need to be designed according to the patients’ age, sex, lifestyle, hobbies, occupation, and physical conditions. The rapid development of remote devices that can monitor patients’ real-time physical conditions post-discharge may encourage better adherence to rehabilitation training.” Relatedly, guidance from the ERS and ATS1 states that: “Experts recommended taking patient’s individual needs and preferences into consideration when decisions regarding comprehensive PR programmes are made.”
Remote Use of PR Tests and Tools
Differing assertions were found regarding the use of rehabilitation tests remotely. Sebio-Garcia et al.30 state that: “Experts in the field have recently proposed what kind of test should be used in a remote environment based on their safety and appropriateness. The short physical performance battery test (SPPB), the sit-to-stand test, the stair climbing test and the timed up and go test have thus been recommended both in those recovering from COVID-19 and also in other patients with respiratory conditions who are vulnerable and at risk.” Wootton et al.19 suggest that: “When providing rehabilitation via telehealth, clinicians need to be aware of some special considerations including the inability to complete comprehensive exercise testing, the need to closely monitor patients, and to have a low threshold for requesting medical reviews. To maximize rehabilitation via telehealth, videoconferencing is recommended as the preferred method for consultation and access to pulse oximeters was felt to be important so that some level of physiological monitoring was available when providing rehabilitation via telehealth.”Siddiq et al.14 assert that: “When the inpatient program is completed, self-management and PR counseling can be still conducted by telehealth technologies. However, during telemedicine, we cannot evaluate 6MWT, manual muscle test, grip strength, and gait. Instead, we can implement 1-min Sit-to-Stand test (1-STS) to assess exercise capacity and cardiovascular responses, five-times STS test to assess and monitor muscle strength, oxygen saturation status, and prescribed exercises to patients.” Guidance from Turkey6 suggests that: “Tele-rehabilitation, video or other visual materials can be used in the presence of eligible infrastructure and if the patient’s cognitive status is appropriate. The PR practices (bronchial hygiene techniques, other respiratory strategies, respiratory muscle strength training and training of devices used for these purposes, etc.) require an active participation of the patient, and one-on-one training should be provided by a team of specialists with the prescription PMR specialist.” Iannaccone et al.23 posit that: “In respiratory rehabilitation, telemedicine is useful for remote monitoring of the prescribed exercises that can be performed online and offline and for monitoring the status of oxygen saturation and cardiovascular parameters.”
Issues, Considerations and Proposed Actions Required for Effective and Safe Virtual PR
De Biase’s commentary on PR in older patients24 highlights the importance of investment in digital connectivity and supports. Giansanti25 points to the need to integrate dedicated devices into telemedicine processes, for example, devices being connected with tools for the 6-min tests for monitoring and with other devices for physiological monitoring. Prvu Bettger et al.36 mention the resource implications of telerehabilitation stating that: “Remote delivery of care and the necessary rapid scale-up of telehealth could be optimised if financial, infrastructure, resource, training and cybersecurity barriers were addressed.” Sheehy et al.21 state that: “It is important that processes are put in place to ensure that patients and therapists can use this method successfully, given the rehabilitation needs and comfort with technology of the individual patient. One or more in-person visits may be required as well.” Simpson and Robinson22 emphasise the advantages but also the limitations of telerehabilitation including ready availability of equipment, technical malfunctions, potential for inadvertent personal data disclosure, limited scope for physical examination; the authors emphasise that such limitations are considered carefully and communicated to patients. Interestingly, a UK survey33 conducted with PR service users found that a significant proportion of users were unwilling or unable or access Web-based healthcare, so service user acceptance is another consideration which merits further research.
On-going Studies and Trials
Many trials have been registered which address the safety and efficacy of the virtual delivery of PR, in addition to systematic reviews, some of which are included herein38, 39, 40, 41, 42, 43, 44.
Irish and International Guidance
Guidance on PR in COVID-19 patients was found from the following countries: Ireland; Britain; Turkey; the United States; and Canada.
Experts recommend identification of unmet rehabilitation needs in patients with COVID-19 who are discharged from the hospital, and consequent tailored rehabilitative interventions, accompanied by compliance with the highest biosecurity standards
“The international task force suggests that COVID-19 survivors with pre-existing/ongoing lung function impairment at 6–8 weeks following hospital discharge should receive a comprehensive PR programme consistent with established international standards, compared to no PR programme”
“Experts recommended taking patient’s individual needs and preferences into consideration when decisions regarding comprehensive PR programmes are made.”
The Discussion component of the document states: “The present study provides consensus-based suggestions for the screening and the rehabilitation process during and after a hospital admission for severe COVID-19 infection. Experts reached consensus based upon indirect evidence and non-systematic clinical observations (i.e. clinical experience) on the need for early rehabilitation during the hospital admission, the screening for treatable traits with rehabilitation in all patients at discharge and 6–8 weeks after discharge, and around the content of rehabilitation for these patients. In absence of a formal evidence-based approach, these findings provide interim guidance for referral and multidisciplinary rehabilitation in a subgroup of patients after hospital admission. Altogether, the data cast a strong claim on the need for screening and rehabilitation options for patients who have been hospitalised. Besides lung function testing (e.g. spirometry, whole-body plethysmography and carbon monoxide transfer factor), this screening should also contain at least an exercise test (cardiopulmonary exercise test, 6-min walk test or shuttle walk test), muscle strength testing and patient-reported outcome measures.”
“PR programmes are indeed well equipped to service this group of patients. Adaptations may need to be made to the rehabilitation programme if the programme typically deals with patients with obstructive lung disease, to cater more to patients with gas-exchange abnormalities. The self-management or education modules may also need to be adapted. It is expected that many patients who have suffered from severe COVID-19, and particularly those with an ICU admission, will have significant skeletal muscle weakness. Following muscle strength testing, specific skeletal muscle training programmes, typically offered with resistance training, are advised by experts. This is also the case in conventional PR.”
“An issue that is unresolved, but of importance to the organisation of rehabilitation for these patients, is the duration for which patients should be considered infectious. There is currently no consensus on how long patients should be self-isolating. Local infection prevention recommendations should be followed and this may require significant adaptation of the rehabilitation programme with, for example, the adoption of “tele-rehabilitation.”
“Patients recovering from a critical care stay should have an assessment at 2–3 months to further assess functional and rehabilitative needs (NICE, 2009). Residual pulmonary function defects have been found in half of the patients who recovered from SARS three months after hospital discharge, though impairment was mild, and 41% of patients had impaired exercise capacity (Ong at al. 2004). A 6-week PR course has been shown to improve function, quality of life and anxiety in elderly patients recovering from COVID-19 (Kai Liu et al, 2020) and a 6-week exercise training programme was effective in improving both the cardiorespiratory and musculoskeletal fitness in patients recovering from SARS (Lau et al, 2005). PR concepts may be engaged at this stage, though formal lung function and exercise testing may not yet be feasible (Spruit et al, 2020).”
British Thoracic Society (2020) COVID-19: information for the respiratory community[iii]
The BTS resource pack (Sept 2020) includes:
Guidance on adapted delivery of pulmonary rehabilitation to patients surviving COVID-19.
BTS guidance states under the heading Safety precautions for remotely supervised interventions: “There is no evidence that remotely supervised recovery programmes are beneficial for COVID-19 survivors.”
As outlined in the companion guidance “BTS Guidance for PR – Reopening Services for the ‘Business as Usual’ Participants” remote delivery of PR could be considered using a variety of platforms [manual- and digital-based solutions] for the COVID-19patient.
“For remotely supervised programmes:
- Written or verbal consent should be obtained.
- Confirm that the patient is aware of adverse signs and symptoms associated with exercising at home.
- Confirm the patient has a safe environment to exercise in.
- Keep regular contact with clinicians to review progress and any relapse.
- Use validated measures of breathlessness and exertion/fatigue to monitor response to exercise prescription.
- The individual will need access to any equipment required to complete the interventions effectively and safely.
- Use of a walking diary to monitor exercise progression.
- Deliver appropriate advice for any outside walking prescription in line with government policy for COVID-19 shielding and/or social distancing.
- Safety and the exercise prescription must be assessed at the time of an initial assessment
- Oxygen requirements should be established at the time of the initial assessment. Therefore, an oximeter is not mandated.”
Other resources available from BTS include:
- Checklist for COVID-19 recovery programme, for use during exercise, is available here. The link opens from the BTS website in PDF format.
- Guidance for Pulmonary Rehabilitation – Reopening Services.
- Checklist of safety precautions for remotely supervised interventions available here. The link opens from the BTS website in PDF format.
- It is advised to stop classes to reduce the risk to patients, and to enable staff redeployment to acute community settings. Consider alternative methods of rehab such as online and web‐based resources.
- This resource pack is intended to be used as a resource for professionals conducting remote assessments during the COVID-19 pandemic. The link opens from the BTS website in PDF format.
- The following resource pack has been put together to support PRwhen face-to-face PR is not possible.” The link opens from the BTS website in PDF format.
Chartered Society of Physiotherapy (UK) (2020) Remote physiotherapy delivery options[iv]
CSP provide information, including:
· Rapid implementation of remote physiotherapy delivery
· National evaluation of remote physiotherapy services
· Evaluating remote physiotherapy options
· Using digital tools to deliver physiotherapy services
Although the content does not relate specifically to virtual delivery of PR for COVID-19 patients, a case study is provided on the use of virtual methods to deliver pulmonary rehabilitation to patients with a range of chronic lung conditions.
Australian Physiotherapy Association (2020) Telehealth guidelines response to COVID-19[v]
“There is strong evidence that telehealth is effective for musculoskeletal conditions and in post-surgical rehabilitation, particularly for the following conditions:
- Osteoarthritis and other chronic joint pain conditions
- Rehabilitation following joint replacement surgery
- Clients requiring cardiac rehabilitation
- Clients requiring PR”
RECOMMENDATION 3.5
“The use of individual devices, mobilization techniques and exercises deemed appropriate for the patient by the PMR specialist should be instructed to the patient by one of the rehabilitation team members during a single session. Some or all of these practices should be performed by a PMR physician [physical medicine and rehabilitation] and available healthcare personnel (nurse, physiotherapist, occupational therapist, physiotherapy technician) depending on the existing conditions and availability of human resources and PPE at the center. General rehabilitation practices such as positioning, mobilization, ROM [range of motion], general muscle strengthening exercises in the aforementioned recommendations can be demonstrated by a physiotherapist, occupational therapist, or nurse with the prescription of a PMR specialist. Tele-rehabilitation, video or other visual materials can be used in the presence of eligible infrastructure and if the patient’s cognitive status is appropriate. The PR practices (bronchial hygiene techniques, other respiratory strategies, respiratory muscle strength training and training of devices used for these purposes, etc.) require an active participation of the patient, and one-on-one training should be provided by a team of specialists with the prescription PMR specialist.”
5. REHABILITATION APPROACH AFTER DISCHARGE in COVID-19 RECOMMENDATION
5.1 “In the post-discharge period, the rehabilitation program with a holistic approach is organized within the scope of general rehabilitation principles by evaluating the impairments in physical, functional, cognitive, psychosocial, and occupational aspects associated with COVID-19. Depending on the scope of the rehabilitation program, the place and model of application (i.e., inpatient, outpatient, hospital-centered control, home-based program, or tele-rehabilitation, etc.) should be determined.”
Released on 27th March the authors say: “We cannot endorse a specific approach to PR during the current challenges. Users are advised to inform patients that the resources below should only be used with involvement and agreement of their provider. To date, home PR alternatives have not had a robust body of evidence to suggest they are a substitute for center-based PR. A key concept is that, for the immediate future, PR is unlikely to be delivered with the patient and the provider face-to-face. The following approaches are offered as possible models to help patients initiate or continue rehabilitative programs in collaboration with a clinical team. This document is shared to help provide options in the current challenging circumstances and should not be considered an endorsement of any individual program model.”
This document provides detailed information about virtual delivery of PR for individuals with chronic lung conditions, but it clearly states: “Recommendations for patients recovering from COVID-19 but without respiratory conditions are beyond the scope of this statement.”
International Literature
The articles have been organised by category: review articles (n=9); original studies (n=5); commentaries, reports and analyses (n=7); letters and editorials (n=7); recommendations on virtual rehabilitation configuration which are not PR specific (n=4).
Review Articles
Abstract: “The COronaVIrus Disease 2019 (COVID-19), which developed into a pandemic in 2020, has become a major healthcare challenge for governments and healthcare workers worldwide. Despite several medical treatment protocols having been established, a comprehensive rehabilitation program that can promote functional recovery is still frequently ignored. An online consensus meeting of an expert panel comprising members of the Taiwan Academy of Cardiovascular and Pulmonary Rehabilitation was held to provide recommendations for rehabilitation protocols in each of the five COVID-19 stages, namely (1) outpatients with mild disease and no risk factors, (2) outpatients with mild disease and epidemiological risk factors, (3) hospitalized patients with moderate to severe disease, (4) ventilator-supported patients with clear cognitive function, and (5) ventilator-supported patients with impaired cognitive function. Apart from medications and life support care, a proper rehabilitation protocol that facilitates recovery from COVID-19 needs to be established and emphasized in clinical practice.”
Figure 1, below, taken from this article, outlines that “tele-rehabilitation or video instruction to avoid direct contact with patients if available” is recommended for patients with mild disease who are isolated at home, both those with no risk factors and also those with risk factors, such as hypertension, Diabetes Mellitus, cardiovascular disease or pulmonary diseases.

Abstract: “CONCLUSION(S): This systematic rapid living review showed an increasing evidence on rehabilitation needs due to COVID-19 outbreak during April 2020. The main novelties include: (1) the first appearance of epidemiological data on the likely high incidence of neurological complications/disabling sequelae in patients hospitalized for COVID-19; (2) rapid guidelines on the management of chronically disabled patients in the COVID-19 era; (3) advice to provide COVID-19 patients with early respiratory rehabilitation in the acute phase, and with telemonitoring and telerehabilitation in the post-acute phase. Although the overall quality of studies has increased, prospective cohort studies on disability course in COVID-19 pandemic and experimental studies on the effects of rehabilitation are still warranted.”
Excerpt from the section Studies reporting on rehabilitation approaches to COVID-19 patients: “In this category, we found one RCT reporting the greater efficacy of 6-week respiratory rehabilitation, compared to no treatment, at improving pulmonary function, endurance, QoL and anxiety in elderly patients with COVID-19.
Two practice guidelines provided recommendations for the management of adult patients with confirmed or suspected COVID-19 in the acute care setting and for the management of swallowing disorders and the assessment of acute dysphonia in the context of the COVID-19.
One qualitative descriptive study shared the early experiences from the clinical field in Northern Italy on the respiratory management of COVID-19 patients in the acute and immediate post-acute phases.
Nine expert opinions provided suggestions about acute and/or post-acute management of people with COVID-19. Some of them provide general advices, others provide specific description of rehabilitation approaches to people with mild or severe respiratory symptoms, whereas, others focus on the rehabilitation needs of specific patients subgroups like people with obesity, pre-existent reduced respiratory muscle performance, people awaiting surgery, and subjects suffering from post-intensive care syndrome secondary to COVID-19.
Key messages:
- In the acute phase, early respiratory rehabilitation was recommended for mild patients, while different views existed for the patients with severe complications;
- In the post-acute phase, telerehabilitation and telemonitoring (using wearable devices, mobile phone APPs, virtual reality) was proposed as the first option, while inpatient or outpatient rehabilitation was suggested for cases with most severe disability. Prehabilitation has also been advised to prevent complications in people undergoing surgery.”
Abstract: “The roles of physical rehabilitation and medicine are expected to increase because post recovery COVID-19 patients are experiencing cardiovascular, neurological, psychological, and cognitive sequalae. Innovative management strategies are needed to limit the spread of disease and to protect vulnerable persons. Significant evidence indicates that the use of telerehabilitation reduces hospitalizations and cardiac events compared to regular care. Actions are needed to prevent deconditioning in rehabilitation patients, and respiratory therapy practices will require close attention to reduce the dispersion of air droplets.”
Sun, T., et al. (2020) “Rehabilitation of patients with COVID-19” [Review][xii]
Abstract: Introduction: In 2020, due to severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2), coronavirus disease (COVID-19) has become a pandemic. As of 11 August 2020, the cumulative number of confirmed cases worldwide had reached 19 million, with 700,000 reported deaths, indicating this pandemic’s significant global impact.; Areas Covered: We reviewed the application of rehabilitation therapy in the clinical treatment of COVID-19 patients. A systematic search was performed using PubMed, Springer, CNKI, and Wanfang Data of database up to 1 August 2020. The search terms included the English terms and their Chinese equivalents: ‘COVID-19,’ ‘ARDS,’ ‘rehabilitation,’ ‘critically ill patients,’ ‘physiotherapy,’ ‘respiratory rehabilitation,’ ‘traditional Chinese medicine,’ and ‘psychotherapy.’; Expert Opinion: Rehabilitation research concerning patients with COVID-19 remains ongoing. Rehabilitation guidance for such patients with COVID-19 is based on previous experience. However, as different patients have differing degrees of dysfunction, personalized plans need to be designed according to the patients’ age, sex, lifestyle, hobbies, occupation, and physical conditions. The rapid development of remote devices that can monitor patients’ real-time physical conditions post-discharge may encourage better adherence to rehabilitation training.
This review, which synthesis data on adults with long-term conditions, rather than COVID-19, is included for its discussion regarding assessing exercise tolerance remotely.
Abstract: “Introduction: The coronavirus disease 2019 (COVID-19) pandemic has seen many cardiopulmonary rehabilitation services delivering programmes remotely. One area of concern is how to assess exercise capacity when a supervised exercise test is not possible. The aim of this review was to examine the relationship between functional exercise tests and recommended exercise tests for cardiopulmonary rehabilitation. Methods: A rapid narrative review was carried out. Searches were conducted by two of the study authors. The study had the following features. Participants: adults, all with long-term conditions; intervention: any/none; outcome: Duke activity status index (DASI), sit to stand (STS, 30 s, 1 min and 5 repetitions), short physical performance battery (SPPB), 4-metre gait speed (4MGS) or step test (Chester/others) AND directly compared to one of the recommended exercise tests for cardiopulmonary rehabilitation: 6-min walk test (6MWT), incremental shuttle walk test (ISWT) or cardiopulmonary exercise test (CPET) in terms of reporting agreement/correlation; Study design: primary research only, controlled trials or observational studies.; Results: Sixteen articles out of 249 screened were included (n=2271 patients). Overall, there were weak-strong correlations for the included tests with a recommended exercise test (r=0.38-0.85). There were few reported issues with feasibility or safety of the tests. However, all tests were supervised in a clinical setting. The test that had the highest correlation with the field walking test was the 4MGS with the ISWT (r=0.78) and with the 6MWT (r=0.85). Discussion: The 4MGS has the highest correlation with routine measures of exercise tolerance. However, it may be difficult to standardise in a remote assessment or to prescribe exercise from. Clinicians should strive for face-to-face standardised exercise tests where possible to be able to guide exercise prescription.”
This review includes the following information about PR using technology:
“The COVID-19 patients in isolation may benefit from PR through educational videos, instruction manuals, or telehealth. When the inpatient program is completed, self-management and PR counseling can be still conducted by telehealth technologies. However, during telemedicine, we cannot evaluate 6MWT, manual muscle test, grip strength, and gait. Instead, we can implement 1-min Sit-to-Stand test (1-STS) to assess exercise capacity and cardiovascular responses, five-times STS test to assess and monitor muscle strength, oxygen saturation status, and prescribed exercises to patients. Telehealth is cost-effective, and neither patients nor physicians require to travel, and it can serve all individuals irrespective of geographical location, although it seems to be unrealistic in developing countries. For patients who are unable to participate in a telerehabilitation program and require input for impaired balance, a face-to-face interview is considered an appropriate measure.”
The review concludes by stating that: “Further prospective clinical studies are needed to unveil which PR programs are safe and effective in COVID-19 survivors, with the goal of improving their QoL beyond their stay within an emergency care facility.”
Original Studies
In this short article the authors outline the PR programme they developed for their patients: “As well as standard care (nutrient Supplementary Material, drug therapy, oxygen, Chinese Traditional Medicine, etc.), each subject received an extra 30-min exercise session led by a trained rehabilitation therapist every day during hospitalization for 2 weeks, with a learning package in the form of audio and visual materials. Until 4 weeks of follow-up after discharge, they were required to continue the program by using the materials, which can be viewed on a tablet, mobile phone, or networked TV. The exercise protocol consisted of eight full-body low-intensity distinct sections (Supplementary Materials 1, 2), with each section being repeated six times. The entire protocol usually took 10–12 minutes to complete at the usual pace, and the training was repeated 2 times, separated by a few minutes break (Ng et al., 2011; Liu et al., 2012). To address the special needs of patients with COVID-19, an expert panel review was conducted to assess the potential clinical risk of this rehabilitation exercise. Tests were also conducted in isolation wards and home environments to study the safety in its application. To ensure safety, patients could maintain nasal cannula oxygen during training and immediately stop training if symptoms such as fatigue and asthma occurred. To keep a record of their own practice, each patient was issued a daily log (Ng et al., 2011).
The integration of video and direct supervision was enjoyable for the subjects. The first pilot study consisted of 10 subjects who took the exercise and used it for 14 days under the guidance of therapists. The purpose was to test the feasibility and usability of the program. The demographic and clinical characteristics of these patients are shown in Table 1. The subjects were 100% adherent, reported that the program was easy to master, and, ultimately, adhered to it. In addition, post-program evaluation showed initial signs of improvement in physical activity, perceptions of dyspnea, and QoL in these subjects when compared to a standard-care control group. However, this research is mainly an explanation of this exercise method, and standardized clinical research will be carried out immediately. As this exercise required very limited supplies and can be done almost everywhere, we believe that it could benefit a large portion of patients with COVID-19; therefore, we conclude that this exercise is to be recommended for COVID-19.”
The supplementary materials referenced here are available: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7273974/.
This pilot project was conducted in the US with 15 participants.
Abstract: “PR has been successfully carried out via telemedicine however initial patient assessment has been traditionally conducted in PR centers. The first step in PR is assessment of patient’s exercise capacity which allows individualized prescription of safe and effective exercise program. With COVID-19 pandemics assessment of patients in PR centers has been limited resulting in significant reduction of patients undergoing life-saving PR. The goal of this pilot study was to introduce approaches for remote assessment of exercise capacity using videoconferencing platforms and provide initial usability assessment of this approach by conducing cognitive walkthrough testing. We developed a remote assessment system that supports comprehensive physical therapy assessment necessary for prescription of a personalized exercise program tailored to individual fitness level and limitations in gait and balance of the patient under evaluation. Usability was assessed by conducting cognitive walkthrough and system usability surveys. The usability inspection of the remote exercise assessment demonstrated overall high acceptance by all study participants. Our next steps in developing user-centered interface should include usability evaluation in different subgroups of patients with varying socio-economic background, different age groups, computer skills, literacy and numeracy.”
Abstract: “Background: Guidelines for physical therapy management of patients hospitalized with COVID-19 recommend limiting physical therapists’ contact with patients when possible. Telehealth has been viewed as “electronic personal protective equipment” during the COVID-19 pandemic; although telerehabilitation has been shown to be effective with outpatients, it is unknown whether it is a viable option for hospitalized patients. Purpose: Our facility developed an algorithm for the use of a physical therapy telerehabilitation program for inpatients with COVID-19. We sought to investigate the safety and viability of the program. Methods: We conducted a retrospective chart review of patients admitted with a diagnosis of COVID-19 who received either telerehabilitation only or a combination of telerehabilitation and in-person rehabilitation. Based on the algorithm, COVID-19 inpatients were selected to receive telerehabilitation if they could ambulate independently, could use technology, had stable vital signs, required minimal supplemental oxygen, and were cognitively intact. We analyzed data of inpatients who received telerehabilitation only, which included patient education, therapeutic exercises, and breathing techniques. Results: Of 33 COVID-19 inpatients who received telerehabilitation, in-person rehabilitation, or a combination of the two, 12 patients received telerehabilitation only (age range, 33 to 65 years; all but one male). They demonstrated independence with their individualized home exercise programs in one to two sessions, did not require an in-person rehabilitation consultation, did not require increased oxygen, experienced no exacerbation of symptoms, and were discharged home.; Conclusions: Inpatient telerehabilitation appears to be a viable option for selected hospitalized patients with COVID-19 and may be a safe way of delivering inpatient rehabilitation to isolated or at-risk populations. At our hospital, the use of inpatient telerehabilitation reduced staff exposure while providing important education and services to patients. To our knowledge, no studies have investigated the use of telerehabilitation for hospitalized patients, including those with COVID-19. Our findings suggest that this innovative approach warrants further study.”
While this article does not expressly mention “PR” it does have a dedicated section on Breathing Techniques:
“At our institution, respiratory therapy traditionally performs respiratory inventions. Due to limited availability of respiratory therapists at our institution during COVID-19, physical therapists assumed responsibility for performing select, non-invasive respiratory interventions. The breathing techniques and exercises used in the telerehabilitation program were based on the PT guidelines adapted from expert consensus. Patients with a productive cough were taken through the active cycle of breathing technique (ACBT) and cough etiquette, the latter important in this population due to the risk of SARS-CoV-2 transmission by aerosol generation. Pursed-lip breathing was taught to patients who were short of breath as a form of breathing control. Straw breathing was taught as a form of positive expiratory pressure to improve ventilation in select patients (Online Resource 1).”
Abstract: “Objective: COVID-19 is a multisystem illness that has considerable long-term physical, psychological, cognitive, social and vocational sequelae in survivors. Given the scale of this burden and lockdown measures in most countries, there is a need for an integrated rehabilitation pathway using a tele-medicine approach to screen and manage these sequelae in a systematic and efficient way.; Methods: A multidisciplinary team of professionals in the UK developed a comprehensive pragmatic telephone screening tool, the COVID-19 Yorkshire Rehabilitation Screen (C19-YRS), and an integrated rehabilitation pathway, which spans the acute hospital trust, community trust and primary care service within the National Health Service (NHS) service model.; Results: The C19-YRS telephone screening tool, developed previously, was used to screen symptoms and grade their severity. Referral criteria thresholds were applied to the output of C19-YRS to inform the decision-making process in the rehabilitation pathway. A dedicated multidisciplinary COVID-19 rehabilitation team is the core troubleshooting forum for managing complex cases with needs spanning multiple domains of the health condition. Conclusion: The authors recommend that health services dealing with the COVID-19 pandemic adopt a comprehensive telephone screening system and an integrated rehabilitation pathway to manage the large number of survivors in a timely and effective manner and to enable the provision of targeted interventions.”
While this paper describes a multidisciplinary intervention it also encompasses PR, as is visible here in Figure 1:

Abstract:“International statements have suggested the PR model a an appropriate rehabilitation option for people recovering from coronavirus disease 2019 (COVID-19). In this case series, we present our COVID-19 telehealth rehabilitation programme, delivered within a PR setting, and discuss the management of our first three cases. All patients were male, with a median age of 73 years. Following hospital discharge, the patients presented with persistent limitations and/or symptoms (e.g. breathlessness, fatigue, and reduced exercise capacity) which warranted community-based rehabilitation. Patients were assessed and provided with an initial six-week rehabilitation programme supported via telehealth using a treatable traits approach. Patients demonstrated improvements in exercise capacity and breathlessness; however, fatigue levels worsened in two cases and this was attributed to the difficulties of managing returning to work and/or carer responsibilities whilst trying to recover from a severe illness. We found that PR clinicians were well prepared and able to provide an individualized rehabilitation programme for people recovering from COVID-19.”
This Australian paper provides a very detailed overview of their approach. Excerpt from Discussion portion of full text:
“When providing rehabilitation via telehealth, clinicians need to be aware of some special considerations including the inability to complete comprehensive exercise testing, the need to closely monitor patients, and to have a low threshold for requesting medical reviews. To maximize rehabilitation via telehealth, videoconferencing is recommended as the preferred method for consultation and access to pulse oximeters was felt to be important so that some level of physiological monitoring was available when providing rehabilitation via telehealth.For patients who may not have access to technology or devices, healthcare providers should consider purchase of these in rehabilitative funding models. Our patients had moderate to severe COVID‐19 with relatively short hospital stays. For patients who are recovering from longer intensive care unit (ICU) stays and who may present with post‐ICU syndrome, more intensive face‐to‐face rehabilitation may be required. A recent guideline provides expert consensus around rehabilitation, including a suggested core set of outcomes for people recovering from COVID‐19 and this should be referred to when planning future COVID‐19 rehabilitation programmes. This is a single‐centre report and the number of cases is limited; however, the case series indicates that rehabilitation via telehealth for people recovering from COVID‐19 is feasible and safe when provided by experienced PR clinicians.”
Reports, Commentaries and Analyses
“This paper proposes a model of a care pathway to mitigate against the impact on the rehabilitation services due to the response of the UK National Health Service in managing the COVID-19 crisis. The value of performing rehabilitation assessment and intervention for COVID-19 survivors alongside the mandatory medical follow-up requirements is elaborated. The issues of capacity and alternative ways of working within the rehabilitation services are explored, and tele-rehabilitation is proposed as a viable alternative to traditional face-to-face intervention. This paper advocates for a tele-rehabilitation pathway model based on the case of need. The proposal was influenced by the clinical experience of the authors, the clinical exigencies of this novel disease, and the local/regional service peculiarities.”
A detailed abstract for this paper is available here.
The authors of this UK paper strongly emphasise the importance of PR for COVID-19 patients and include dedicated sections on:
- Making a Case for Tele-Rehabilitation and Why It Should Be Considered for COVID-19 Patients
- Proposed Post-Discharge Follow-Up and Tele-Rehabilitation Pathway for COVID-19 Patients
The paper specifically mentions PR as a component of the multidisciplinary approach required and features a proposed COVID-19 Patient Follow-up Pathway.

Excerpt from the conclusion: “Patients should be offered the opportunity to participate in tele-rehabilitation programs in addition to any other input provided by community services. Tele-rehabilitation would be helpful for majority of patients who require input such as PR, psychological support, and nutrition advice. Patients unable to participate in a tele-rehabilitation program and those requiring highly specialist input for impairments such as balance deficits would require face-to-face assessment, and appropriate infection risk management will be implemented to support this.”
Sheehy, L. M. (2020) “Considerations for Postacute Rehabilitation for Survivors of COVID-19″[Report][xxi]
The objective of this report, as outlined in the abstract, is to answer the question “What rehabilitation services do survivors of COVID-19 require?”
Excerpt from the section Home-Based Rehabilitation: “If patients can be managed at home, this may be a good option, even for patients who might have been admitted to inpatient rehabilitation in the past. Isolation is easier at home, and the burden on inpatient services would be lessened. However, for this to be a viable choice, enhanced homecare services and outpatient rehabilitation must be available and able to provide a level of care on par with inpatient rehabilitation. This mode of delivery may be difficult to institute if home care staff are restricted from entering patients’ homes. However, given the right precautions, home-based care may be safer for patients who have recovered from COVID-19 and for other patients in a rehabilitation unit. Home-based therapy can be provided over the internet and telephone via telerehabilitation. Both assessment and treatment may be provided, either synchronously (ie, in real time) or asynchronously (eg, a prerecorded customized exercise plan). It is important that processes are put in place to ensure that patients and therapists can use this method successfully, given the rehabilitation needs and comfort with technology of the individual patient. One or more in-person visits may be required as well. Telerehabilitation may also be a good choice for patients being discharged from inpatient rehabilitation to continue their treatment and promote further recovery.”
The full text of this article includes a dedicated section on Innovative Approaches to Providing Rehabilitation During the COVID-19 Pandemic:
Virtual Rehabilitation
“In the context of the COVID-19 pandemic, virtual care outpatient episodes may be preferable to face-to-face interactions for multiple reasons. Firstly, to take care of patients, healthcare providers must first themselves be in good health. The healthcare population, physicians in particular, is aging. In the United States, more than 20% of physicians are older than 65 yrs. Many older healthcare practitioners will have their own long-term health conditions and may fear for their safety on exposure to COVID-19 patients. Secondly, from a patient, family, and wider societal perspective, delivering healthcare in settings where groups of people gather such as ‘waiting rooms’ is actively discouraged for fear of further community spread. In this context, it is also possible that a healthcare provider may be carrying COVID-19 asymptomatically; in such a case, the healthcare provider may then inadvertently become a ‘super spreader.’
Virtual care circumvents these issues and allows personalized consultation and treatment via telephone or live Internet connections, or via pre-recorded sessions for more generic materials. In some countries, well-developed, secure virtual care platforms already exist; in others, media such as Zoom, Skype, Facetime, and others may be suitable alternatives. However, virtual care also has many limitations, such as ready availability of equipment, technical malfunctions, potential for inadvertent personal data disclosure, limited scope for physical examination, and the process largely relies on the patient being able to attend to sessions, communicate, and interact accordingly. This may not be possible for many patients. Rehabilitation providers should start to consider the scope and limitations of virtual physical examinations and make patients expressly aware of this accordingly.”
Excerpt from the sectionTelemedicine and Remote Rehabilitation Unit: “The presence of a telemedicine and rehabilitation unit is recommended to promote protected discharge, to monitor patients in quarantine, and to ensure the continuity of care for patients with COVID-19 but also for patients that do not have COVID-19. It is also useful for sharing complex clinical cases with other hospitals or clinics in the area (hub-and-spoke system), thus avoiding unnecessary patient movements.
In the last years, the rehabilitation and functional recovery department of the San Raffaele Hospital has been increasingly using remote rehabilitation for memory and language deficits. Such remote care of patients can be expanded to help caregivers in the daily assistance of patients, for example with nutritional advice to avoid malnutrition after discharge.
In respiratory rehabilitation, telemedicine is useful for remote monitoring of the prescribed exercises that can be performed online and offline and for monitoring the status of oxygen saturation and cardiovascular parameters.”
De Biase, S., et al. (2020) “The COVID-19 rehabilitation pandemic” [Commentary][xxiv]
This commentary reviews the likely rehabilitation needs of older people both with and without COVID-19 and discusses how strategies to deliver effective rehabilitation at scale can be designed and implemented in a world living with COVID-19.
Key points
- Post-COVID-19 rehabilitation will be complex and requires specialist multidisciplinary multiagency services.
- Deconditioning and frailty as a result of self-isolation, shielding and social distancing will also require therapy services.
- Older people need access to rehabilitation services in a timely fashion that meets their personal needs and goals.
- Rehabilitation services need to prepare for a post-pandemic wave of older people in need.
Rehabilitation for people surviving COVID-19 infection:
“The workforce delivering COVID-19 rehabilitation must be able to manage the full range of consequences of COVID-19 infection: breathlessness, fatigue, muscle weakness, delirium, post-traumatic stress disorder and other mental health conditions, all of which will impact on rehabilitation outcome. Each patient will need an individualised programme, including aerobic exercise, strength training, balance training, breathlessness management, energy conservation, functional and vocational rehabilitation, and psychological support. Such a programme can be delivered effectively only by a multidisciplinary team, which needs to have access to the full range of physical and occupational therapy, medical, nursing, dietetic, psychology and speech and language staff.
Older COVID-19 survivors will not only have deficits that reflect frailty syndromes (for example falls and sarcopenia), which many older people’s services are set up to manage. They may also have substantial cardiorespiratory and neurological deficits. As a result, cardiac, pulmonary, neurology and frailty services cannot continue to work in isolation. Instead, specialist services must learn rapidly from each other now to deliver on all aspects of rehabilitation need and models of service delivery need to both combine personnel, knowledge and skills from all of these disease-specific rehabilitation services.
“Where rehabilitation is delivered is likely to change, with less emphasis on clinic or hospital-based services, and more emphasis in services delivered in or near patients own homes. This will mean changes in how rehabilitation is delivered—approaches involving travel or group work are likely to be especially vulnerable to future pandemic waves or the imposition of movement restrictions. Early investment in digital connectivity to support rehabilitation must therefore continue, particularly in rural areas; such investments will also help not only to develop a system that is resilient to future pandemic waves, but also to permanent changes in how we live if the severe acute respiratory syndrome coronavirus 2 becomes endemic. The pandemic response has brought opportunities as well as challenges—for instance highlighting how physical activity and exercise can be integrated into daily life via remote communication. This must be now be scaled up to support older people, care home residents and others who are currently (or may in future be) confined to their own homes with limited social contact. Even where face-to-face delivery of rehabilitation is able to restart, it is likely that more of this activity will need to happen remotely to enable efficient delivery of rehabilitation at scale.”
Abstract: “Recent studies published in the Telemedicine and e-Health journal stated the reality in Italy of the importance of telemedicine promotion during the coronavirus 2019 (COVID-19) pandemic. In Italy, we gradually approached the second phase of the COVID-19 pandemic. During this phase, the activities restarted according to a temporal plan. During the second phase, “social distancing” will continue and telemedicine will continue to play a pivotal role … An emerged categorization takes into consideration (1) the subjects with fragility, including those with rare diseases; (2) the experience gained during the emergency; (3) the new opportunities emerged for telemedicine boundaries; and (4) the new needs for telemedicine-based PR at home.”
Excerpt from the sectionNew Models for Pulmonary Rehabilitation Using Telemedicine: “During the pandemic, there was a lot of discussion on the treatment of those subjects with lung problems caused by the virus. A lot of space was dedicated both to the technologies used in intensive care rooms and to the home-monitoring devices (such as, e.g., the pulse oximeters). In general, a patient returning home after weeks of intubation needs a properly designed home rehabilitation program, based also on pulmonary stimulation tools suitably integrated into e-health and m-health. Looking at the science during the COVID-19 emergency, it can be observed that the viewpoint published in the Telemedicine and e-Health journal is still strongly valid.
In this viewpoint, new technological needs for pulmonary telerehabilitation were described. In particular, the need to integrate dedicated devices into telemedicine processes to exercise the respiratory acts was highlighted (Fig. 1). These devices eventually could be connected with tools for the 6-min tests for monitoring and with other devices for physiological monitoring (Fig. 2).

Fig. 2. New model for lung rehabilitation for COVID-19 patients
We must also consider that currently in the second phase, patients are still leaving hospitals after long periods of acute respiratory events. Therefore, new models, such as the already described models, could be highly useful.”
Published in June 2020, it is noteworthy that this protocol includes PR considerations but does not mention delivery of same using a virtual/telehealth/online platform.
Letters, Viewpoints and Editorials
Asly, M. and A. Hazim (2020) “Rehabilitation of post-COVID-19 patients.”[Letter][xxvii]
In this letter (from Morocco), Asly et al. outline their suggested respiratory rehabilitation for post COVID-19 patients as: “Breathing exercises aimed to improve breathing control may potentially be proposed, under assessment and monitoring of exercise tolerance. They are effective for increasing tidal volume and reducing psychological consequences (stress, anxiety and depression); Lung secretion clearance should implement, if necessary, using expiratory flow accelerator (EFA) technique …
Depending on the case, this rehabilitation can be carried out in several organisational modalities: inpatient, outpatient or at home. In the context of the COVID-19 pandemic, the use of remote monitoring and mobile intelligence technologies with wearable devices can made possible to practice intelligent and digital remote rehabilitation. Remote virtual reality exercises can be offered to these patients, the effectiveness and safety of these tools have been proven to be non-inferior to traditional approaches.”
COVID-19 is a highly infectious respiratory disease which leads to a respiratory and physical dysfunction. For patients discharged at home, post-acute care, PR is an important intervention to relive dyspnea and anxiety, to improve exercise capacity and the quality of life (QoL). Due to mandatory social distancing telemedicine could be a useful method. The aims of this study are to assess the efficacy and feasibility of a 4-week exercise training program with telemonitoring and to evaluate the impact of the program on the QoL. Method(s): A COPD assessment test (CAT) was used before and after the training program to measure QoL, performance in activities of daily living were measure through the Barthel scale. Weekly phone calls were made by a medical doctor, using the Fenix televista program to collect data on dyspnea, cough and asthenia or other symptoms. This remote care service was complemented by a respiratory rehabilitation program (sent as educational video) which consists of breathing exercises, aerobic training at mild-to-moderate intensity and muscle reinforcement. Oxygen saturation was checked. Workloads were adjusted based on the improvement/worsening of symptoms. Patients with suggestive symptoms of exacerbation detected during the phone interview were directed towards a specialist. The project is still ongoing, starting on April 2020 at Rimini Hospital (Italy). Currently 50 symptomatic patients were enrolled (post-acute severe infection). The program is well accepted, only 2 patients dropped out due to poor compliance. Method(s): A preliminary analysis of the data highlights good efficacy and feasibility of this approach to optimize a rapid recovery in COVID-19 patients.
The authors suggest: “To prevent a postpandemic wave of deferred diagnoses and unchecked disease progression, we need to strategically plan and restructure care delivery for outpatient pulmonary medicine. We describe the following three major domains that deserve consideration: before the visit, during the visit, and after the visit …
Opportunities for virtual PR should be explored, and grounds gained on enhanced telehealth reimbursement practices should be retained beyond the acute phase of the pandemic …
In addition, there is a need for studying the validity, feasibility, and efficacy of home-based monitoring and treatment tools, such as spirometry, accelerometers, and virtual PR, to allow a realistic consideration of their deployment and use in the near future.”
Sebio-Garcia, R. (2020) “Pulmonary rehabilitation: Time for an upgrade”[Editorial][xxx]
Excerpt: “Among the potential ways to extend the benefits of PR the use of telemedicine and medical technology has gained quite popularity. In a recent study published by Jimenez et al., the addition of a mHealth application with a patient-educator interaction following a PR programme of 12 weeks resulted in an increase in adherence to respiratory physiotherapy treatment compared to a control group. Technology-supported exercise interventions, with the addition of a monitoring device, such as a pedometer or a fitness tracker, have shown to be effective in improving physical activity when a target is set (for example, 10.000 steps per day). However, the success of these devices in improving or maintaining physical activity and/or exercise capacity are likely to be subject to the support of a behavioural change intervention. Therefore, a multi-disciplinary team should be monitoring and supporting the use of this technology instead of just giving it to the patient and “let him be” …
There’s an urgent need to provide an adequate response to the demands that this population is facing with the on top difficulty of adapting traditional face-to-face rehabilitation to other delivery platforms as we continue under the social distancing premises. The COVID-19 should work as a “wake-up call” for governments and healthcare systems to implement telehealth solutions including tele-rehabilitation and remote monitoring of patients in preparation for future waves with potential new periods of isolation which will compromise again the ability to deliver PR interventions at the hospital or in the community. In addition to those who are already undertaking PR, rehabilitation services will also have to provide safe alternatives for the screening, inclusion and monitoring of new patients (both COVID-19 and non-COVID19) in this context. To this matter, experts on the field have recently proposed what kind of test should be used in a remote environment based on their safety and appropriateness. The short physical performance battery test (SPPB), the sit-to-stand test, the stair climbing test and the timed up and go test have thus been recommended both in those recovering from COVID-19 and also in other patients with respiratory conditions who are vulnerable and at risk. Overall, there’s enough evidence to support the use of tele-rehabilitation as a safe, effective alternative to traditional PR not only as a short-term solution to the current situation but also to alleviate the burden on rehabilitation services and healthcare systems and increase reach to PR to more patients in need.”
This editorial references Turkish guidelines for PR of patients with COVID-19 and suggests that:
“In the near future, PMR physicians may face various problems related to rehabilitation and need to develop strategies rapidly during this time. One of these strategies is to use innovative approaches to rehabilitation during the COVID-19 outbreak. Using advanced communication techniques, telemedicine, or virtual reality in rehabilitation may be appropriate for such diseases. It is likely that we will need to diversify and improve these techniques, so that we can be more prepared for COVID-19 and similar situations which may occur in the future.
In conclusion, our goals should be focused on both to rehabilitate COVID-19 patients successfully and to protect the health of rehabilitation team members. A well and carefully designed rehabilitation program should be developed by the PMR specialty for COVID-19 patients. Nowadays, there are multifactorial, unknown problems for the management of pandemic and each country shows an extra effort to do their best in their own health care system. As PMR physicians, sharing our experiences in a network will bring light to others. Finally, in the future, we hope that the number of high-quality publications related to the rehabilitation field will increase, as the experiences with the management of COVID-19 increase.”
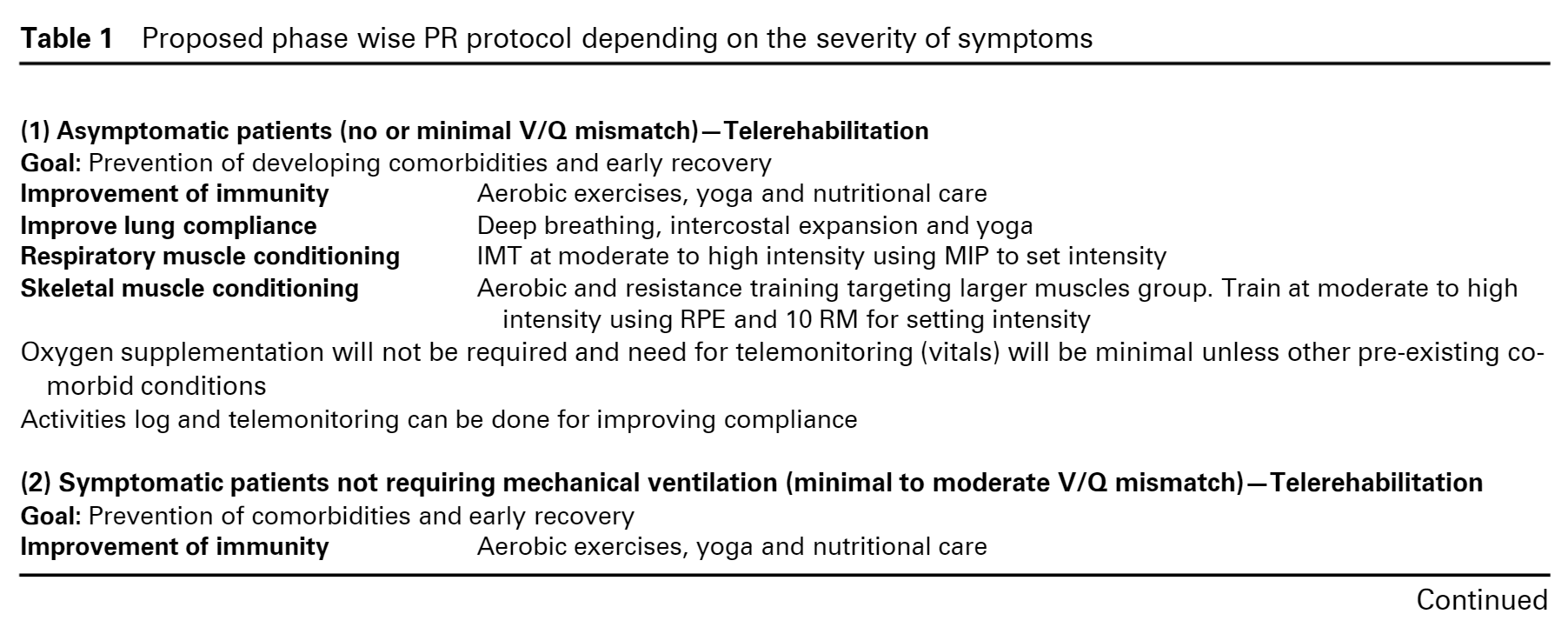
Excerpt: “PR has the potential to play a vital role in the recovery of patients infected with severe acute respiratory syndrome coronavirus 2 (SARS‐CoV‐2). However, the traditional approach to PR is not conducive to the healthcare environment in the COVID‐19 era. In this context, the approach must be modified from the perspective of both the rehabilitation programme employed as well as a focus on minimizing the possibility of viral spread by transferring the patients to the government or community‐designated isolation centres. In this pandemic era, the multidisciplinary role by members is crucial with primary role of the members being to re‐enforce the PR plan for COVID‐19 and provide awareness, education and support whenever required.
Telerehabilitation is an important component of PR in this environment as it allows access to patients who would benefit while minimizing human‐to‐human contact. During face‐to‐face treatment, healthcare professionals should employ techniques that require minimal manual handling of patients, such as remote‐controlled mechanical tilting beds, mechanical assisted limb exercisers and closed‐circuit suctioning. In the immediate post‐recovery period, patients must remain in isolation for at least 2 weeks before enrolling for supervised PR programme. During this isolation phase, patients should be advised to perform low‐to‐moderate intensity exercises as per individual capabilities or using self‐perceived exertion scales which can be easily administered from remote centres. Following the self‐isolation phase, exercise testing and prescription need to be assessed under strict protocols to minimize viral spread; properly ventilated rooms and sanitization of rehabilitation settings are essential components. Proper nutritional counselling and psychological rehabilitation are also important components of PR that should be included. Table 1 lists a proposed modified approach to PR for the COVID‐19 era. The authors of this correspondence hope that readers will find this proposed approach to be of value when considering how to alter the approach to PR.”
The authors also provide a diagram of their suggested approach which is available in full here and the types of PR which are recommended using telerehabilitation are included below:

Abstract: “Remote models of PRPR are vital with suspension of face-to-face activity during the COVID-19 pandemic. We surveyed digital access and behaviours and PR delivery preferences of current PR service users. There was significant heterogeneity in access to and confidence in using the Internet with 31% having never previously accessed the Internet, 48% confident using the Internet and 29% reporting no interest in accessing any component of PR through a Web-based app. These data have implications for the remote delivery of PR during the COVID-19 pandemic and raise questions about the current readiness of service users to adopt Web-based delivered models of PR.
This UK based survey study concludes by stating: “In conclusion, digital access and behaviour among PR service users is heterogeneous with a significant proportion unable or unwilling to access Web-based healthcare. This has implications for remote PR delivery during the COVID-19 pandemic and provides insight into the feasibility of digital PR adoption.”
Recommendations on Virtual Rehabilitation (not PR specific)
While this article does not specifically mention PR it does provide detailed guidance on the virtual delivery of rehabilitation, which may be transferrable to PR.
Excerpt: “Key themes covered in this article include selecting appropriate virtual care platforms, consenting patients for virtual care and conducting successful virtual visits. It also reviews strategies for performing virtual physical examinations and engaging learners in virtual care.”
While this article doesn’t focus exclusively on virtual delivery of PR it does outline how a regional-based rehabilitation model using a dedicated IT platform could be developed so it may be of interest. The full abstract is available here.
Excerpt: “In the COVID-19 pandemic scenario, an IT system as a network based on a dedicated IT platform would be a very useful strategy to meet the needs of very different bodies such as healthcare agencies, healthcare professionals and patients with their families. The IT strategy also includes remote assistance called telemedicine, and specifically Tele-rehabilitation, to treat selected patients able to use this approach, both for clinical conditions and personal factors, and represents an opportunity for patients and professionals to implement care services, avoid difficulties of access and reduce the infection spreading. Furthermore, the IT system could provide better monitoring and reporting of the interventions through captured data flows and the optimal allocation of available economic resources. The proposed model of the IT-based network, the bodies involved, and the expected results are briefly illustrated in Figure 1.”

While this article does not focus exclusively on PR, it highlights the resource requirements of telerehabilitation:
Summary
- “Rehabilitation services are essential: They need to continue during a pandemic and after as they are an essential component of high-value care offered for individuals across the lifespan to optimise physical and cognitive functioning to reduce disability.
- Rehabilitation care is affected: Globally, the response to COVID-19 is shifting rehabilitation services provided in all settings, introducing new burden on patients, families and healthcare workers.
- Measurement needed: A core set of measures needs to be adopted to monitor the health and functional outcomes for COVID-19 and other patients at risk for functional decline and to assess the quality, availability and accessibility of services today and as our nations recover.
- Telerehabilitation is necessary: Remote delivery of care and the necessary rapid scale-up of telehealth could be optimised if financial, infrastructure, resource, training and cybersecurity barriers were addressed.
- Collaboration can support needs in the home: Novel partnerships that include the rehabilitation community could enhance communication and delivery of safe and effective home-based rehabilitative strategies to mitigate the consequences of COVID-19 and reduced service capacity.
- Direct care providers need personal protective equipment: Rehabilitation providers in all settings should be ensured personal protective equipment and training to use it effectively.”
Abstract: “Purpose: The healthcare system and service capacity are overwhelmed by the COVID-19 pandemic. There is a substantial unmet need for rehabilitation service to all patients affected by COVID-19 directly or indirectly. This article aims to describe how to rapidly reconfigure and bring rehabilitation services back during the pandemic.; Method: The Steer committee meeting was held for the development of a strategic preparedness plan and safety management based on principles and evidence of rehabilitation, which will lead to effective mitigation of consequences resulted from COVID-19.; Results: Five measures were taken in Southwest China during the pandemic, which includes the “First contact responsibility” and management system; the full-coverage system for nosocomial infection control; the “Closed-off management” system; the full-coverage system for body temperature monitoring; the adoption of 5G-based telerehabilitation. With the implementation of these measures, the capacity and capability were enhanced to safely reopen and operate rehabilitation facilities in Southwest China.; Conclusion: Further measurement of quality of care and outcomes during and beyond the pandemic is needed in transforming the healthcare system and improving rehabilitation services. Hopefully, the positive message conveyed by this paper could encourage and support communities and the society of physical medicine and rehabilitation worldwide during this challenging time. IMPLICATIONS FOR REHABILITATION Rehabilitation services are essential and there is an unmet need posed by the COVID-19 pandemic. A feasible strategic plan and safety management measures are critical to reconfigure the capacity and capability of rehabilitation services suspended by COVID-19. The adoption of tele-rehabilitation technology has the potential to reshape public health emergency responses and the delivery of care. Measurement of quality and outcomes is of great importance to inform transformation and adaptation of rehabilitation services during and after the COVID-19 pandemic.”
On-going Trials and Reviews
A number of on-going trials and reviews were identified including:
The review question is: Which respiratory rehabilitation approaches are effective in improving the health status of COVID-19 patients? The anticipated completion date for the review is April 2021.
Koc, U. (2020) “Tele-rehabilitation Versus Home Exercise Program in COVID-19”[xl]
This study seeks to answer the question: Is Tele-rehabilitation Superior to Home Exercise Program in the PR of the Patients With COVID-19 With Post-intensive Care Syndrome?
COVID-19 could cause respiratory distress in a minority of cases and requires intensive care and mechanical ventilation. When patients recover and are discharged from hospital, physical, cognitive and emotional complications known as post-intensive care syndrome is seen in the majority of patients and requires rehabilitation. PR is a comprehensive intervention consists of assessment of patient, exercise training and education in order to improve physical and psychological condition of people with chronic respiratory disease. The patients with COVID-19 with post-intensive care syndrome will be randomized two groups: tele-rehabilitation group and home exercise group. There will not be a non-exercising control group due to the ethical issues. The exercise program of both groups will be prescribed by a physiatrist based on the physical examination and the functional capacity of the patients. Tele-rehabilitation group will perform the exercise program 3 days/week for 10 weeks. One session will include aerobic, flexibility and strengthening exercises for lower and upper extremity and breathing exercise. The trainings will start with low-intensity exercises and intensity and duration of the exercises will progress according to the condition of the patient. Intensity of the exercises will be monitored by Borg scale based on dyspnea and exertion symptoms during the sessions. Home exercise group will perform the exercises at their home on their own, 3 days/week for 10 weeks. The patients will be trained about the individualised exercise program as the first session provided at the hospital. The physiotherapist will call the patients weekly, modifications in the exercise program will be made according to the patient’s reports. Outcomes will be measured at baseline, within 1 week of completion the program, 6th months and 12th months following the rehabilitation.
This article outlines their premise that virtual reality could be used for multidisciplinary rehabilitation of patients for PICS-COV patients, which is the subject of a current Clinical Trial Although it does not focus exclusively on PR of these patients it does seek to improve their functioning and includes secondary outcomes, such as 6 minute walk test and one-repetition maximum test.
The above represents only a selection of the available clinical trial study protocols which have been registered, additional study protocols can be supplied if of interest.
Patient Information Materials
Rapidinfo4u Healthcare Repository provides a variety of patient centric resources, which could potentially be utilised in a virtual PR programme, for example:
COVID-19 patient rehabilitation booklet Information for patients[xlv]
Developed by the Leeds Teaching Hospitals NHS Trust by a group of Allied Health Professional (AHPs) who came together to develop some original work done by the Liverpool Heart and Chest Hospital into a COVID-19 patient rehabilitation booklet.
This booklet provides patients and their families information on all aspects of the COVID-19 rehabilitation process, with key areas being: breathing, exercise, diet, swallowing and speech, fatigue and post-traumatic stress.
Progressive Muscle Relaxation for Pulmonary Rehabilitation[xlvi]
University Hospital Limerick have shared a Progressive Muscle Relaxationscript forPR.
Point-of-Care Tools
What does BMJ Best Practice say?
This BMJ Best Practice topic mentions PR is mentioned in the context of Long COVID, but no specifics are given about remote delivery of same:
“Management : give advice and information on self-management including ways to self-manage symptoms (e.g., set realistic goals, antipyretic for fever, breathing techniques for chronic cough, home pulse oximetry for monitoring breathlessness, PR, staged return to exercise); who to contact if there is concern about symptoms or if there is need for support; sources of support (e.g., support groups, online forums); and how to get support from other services (e.g., social care, housing, financial support). A personalised, multidisciplinary rehabilitation plan that covers physical, psychological, and psychiatric aspects of rehabilitation is an important part of management.”
What does UpToDate say?
“For patients who have moderate to severe dyspnea (eg, Borg score >3), persistent desaturations (SpO2 ≤92 percent), continue to have a new requirement for supplemental oxygen, or have other concerning respiratory symptoms, we advise referral to a pulmonary specialist for additional investigation and consideration of PR.
“For patients with more pronounced limitations of endurance or exercise tolerance due to muscle weakness or deconditioning, we typically refer for physical therapy or rehabilitation; those with poor exercise performance due to cardiopulmonary pathology are more likely to benefit from a specialized cardiac or PR program.
“Home- or web-based rehabilitation (“tele-rehabilitation”) – For some patients, tele-rehabilitation is another option. Remote delivery of rehabilitation services may be preferable in areas of high infection prevalence to minimize the potential spread of COVID-19. However, rehabilitation-at-home models vary widely in the services provided, and are of unproven benefit in patients recovering from COVID-19.
Telerehabilitation can be delivered either synchronously (ie, in real-time) or asynchronously (eg, a pre-recorded customized exercise plan). Systems need to be established in order to use these methods successfully given the wide range of patient rehabilitation needs and varying access and patient comfort with technology. Telerehabilitation may be supplemented with one or more in-person visits.”
[i] Spruit MA, Holland AE, Singh SJ, Tonia T, Wilson KC, Troosters T. COVID-19: Interim Guidance on Rehabilitation in the Hospital and Post-Hospital Phase from a European Respiratory Society and American Thoracic Society-coordinated International Task Force. Eur Respir J. 2020 Aug 13;56(6):2002197. doi: 10.1183/13993003.02197-2020. https://pubmed.ncbi.nlm.nih.gov/32817258/ [Accessed 26th January 2021].
[ii] Irish Society of Chartered Physiotherapists (2020) ISCP Guide for Rehabilitation of inpatients with COVID 19 V1 1 02-06-2020 https://irishthoracicsociety.com/education/irish-thoracic-society-guidelines/ [Accessed 26th January 2021].
[iii] British Thoracic Society (2020) COVID-19: information for the respiratory community https://www.brit-thoracic.org.uk/covid-19/covid-19-information-for-the-respiratory-community/ [Accessed 26th January 2021].
[iv] Chartered Society of Physiotherapy (UK) (2020) Remote physiotherapy delivery options https://www.csp.org.uk/news/coronavirus/remote-service-delivery-options [Accessed 26th January 2021].
[v] Australian Physiotherapy Association (2020) Telehealth guidelines response to COVID-19 https://australian.physio/sites/default/files/APA_Telehealth-Guidelines-COVID19_FA.PDF accessed via https://australian.physio/sites/default/files/APA_Telehealth-Guidelines-COVID19_FA.PDF [Accessed 26th January 2021].
[vi] Turkish Society of Physical Medicine and Rehabilitation Specialists (TSPRM)/ Cardiopulmonary Study Group (2020)
Pulmonary rehabilitation principles in SARS-COV-2 infection (COVID-19): A guideline for the acute and subacute rehabilitation. http://www.ftrdergisi.com/uploads/pdf/pdf_4189.pdf [Accessed 26th January 2021].
[vii] American Thoracic Society (2020) Pulmonary Rehabilitation Resources in a Complex and Rapidly Changing World https://www.thoracic.org/members/assemblies/assemblies/pr/resources/pr-resources-in-a-complex-and-rapidly-changing-world-3-27-2020.pdf [Accessed 26th January 2021].
[viii] Dechman, G., et al. (2020). “Delivering pulmonary rehabilitation during the COVID-19 pandemic: A Canadian Thoracic Society position statement.” Canadian Journal of Respiratory, Critical Care, and Sleep Medicine 4(4): 232-235. https://www.tandfonline.com/doi/full/10.1080/24745332.2020.1828683 [Accessed 26th January 2021].
[ix] Cheng, Y. Y., et al. (2021). “Rehabilitation programs for patients with COronaVIrus Disease 2019: consensus statements of Taiwan Academy of Cardiovascular and Pulmonary Rehabilitation.” J Formos Med Assoc 120(1 Pt 1): 83-92. https://pubmed.ncbi.nlm.nih.gov/32863084/
[Accessed 26th January 2021].[x] De Sire, A., et al. “Systematic rapid living review on rehabilitation needs due to COVID-19: update as of April 30th, 2020.” European journal of physical and rehabilitation medicine 56(3): 354-360. https://pubmed.ncbi.nlm.nih.gov/32408729/ [Accessed 26th January 2021].
[xi] Patel, DJ. and Patel, V. (2020) A Review of the Current State of Management and Post-Recovery Rehabilitation of COVID-19. Critical Reviews in Physical and Rehabilitation Medicine. 32(2) 97-109. DOI: 10.1615/CritRevPhysRehabilMed.2020034616 [Accessed 26th January 2021].
[xii] Sun, T., et al. (2020). “Rehabilitation of patients with COVID-19.” Expert Review Of Respiratory Medicine 14(12): 1249-1256. https://pubmed.ncbi.nlm.nih.gov/32799694/ [Accessed 26th January 2021].
[xiii] Houchen-Wolloff, L., et al. (2020). “Which functional outcome measures can we use as a surrogate for exercise capacity during remote cardiopulmonary rehabilitation assessments? A rapid narrative review.” ERJ Open Research 6(4). https://pubmed.ncbi.nlm.nih.gov/33313302/
[Accessed 26th January 2021].[xiv] Siddiq, M. A. B., et al. (2020). “Pulmonary Rehabilitation in COVID-19 patients: A scoping review of current practice and its application during the pandemic.” Turkish Journal of Physical Medicine and Rehabilitation 66(4): 480-494. https://pubmed.ncbi.nlm.nih.gov/33364571/
[Accessed 26th January 2021].[xv] Chen, J. M., et al. “The Application of Eight-Segment Pulmonary Rehabilitation Exercise in People With Coronavirus Disease 2019.” Frontiers in Physiology 11.
https://pubmed.ncbi.nlm.nih.gov/32574241/ [Accessed 26th January 2021].
[xvi] Finkelstein J, Jeong IC, Doerstling M, Shen Y, Wei C, Karpatkin H. Usability of Remote Assessment of Exercise Capacity for Pulmonary Telerehabilitation Program. Stud Health Technol Inform. 2020 Nov 23;275:72-76. doi: 10.3233/SHTI200697. PMID: 33227743.
https://pubmed.ncbi.nlm.nih.gov/33227743/ [Accessed 26th January 2021].
[xvii] Rosen, K., et al. (2020). “Delivering Telerehabilitation to COVID-19 Inpatients:A Retrospective Chart Review Suggests It Is a Viable Option.” HSS journal : the musculoskeletal journal of Hospital for Special Surgery: 1-7. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7364751/ [Accessed 26th January 2021].
[xviii] Sivan, M., et al. (2020). “Development of an integrated rehabilitation pathway for individuals recovering from COVID-19 in the community.” Journal of rehabilitation medicine 52(8): jrm00089. https://pubmed.ncbi.nlm.nih.gov/32830284/ [Accessed 26th January 2021].
[xix] Wootton, S. L., et al. (2020). “COVID-19 rehabilitation delivered via a telehealth pulmonary rehabilitation model: a case series.” Respirology Case Reports 8(8): e00669. https://pubmed.ncbi.nlm.nih.gov/33042547/ [Accessed 26th January 2021].
[xx] Salawu A, Green A, Crooks MG, Brixey N, Ross DH, Sivan M. Int J Environ Res Public Health. 2020 Jul 7;17(13):4890. doi: 10.3390/ijerph17134890. PMID: 32645876; PMCID: PMC7369849. Full text available at: https://pubmed.ncbi.nlm.nih.gov/32645876/ [Accessed 26th January 2021].
[xxi] Sheehy, L. M. (2020). “Considerations for Postacute Rehabilitation for Survivors of COVID-19.” JMIR Public Health Surveill 6(2): e19462. https://pubmed.ncbi.nlm.nih.gov/32854317/ [Accessed 26th January 2021].
[xxii] Simpson, R. and L. Robinson “Rehabilitation After Critical Illness in People With COVID-19 Infection.” American journal of physical medicine and rehabilitation 99(6): 470-474. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7253039/ [Accessed 26th January 2021].
[xxiii] Iannaccone, S., et al. (2020). “Role of Rehabilitation Department for Adult Individuals With COVID-19: The Experience of the San Raffaele Hospital of Milan.” Archives of Physical Medicine and Rehabilitation 101(9): 1656-1661. https://pubmed.ncbi.nlm.nih.gov/32505489/[Accessed 26th January 2021].
[xxiv] De Biase, S., et al. “The COVID-19 rehabilitation pandemic.” Age and Ageing 49(5): 696-700. https://pubmed.ncbi.nlm.nih.gov/32470131/ [Accessed 26th January 2021].
[xxv] Giansanti, D. (2020). “The Italian Fight Against the COVID-19 Pandemic in the Second Phase: The Renewed Opportunity of Telemedicine.” Telemedicine journal and e-health : the official journal of the American Telemedicine Association 26(11): 1328-1331.
https://pubmed.ncbi.nlm.nih.gov/32579866/ [Accessed 26th January 2021].
[xxvi] Zeng, B., et al. (2020) “Expert consensus on protocol of rehabilitation for COVID-19 patients using framework and approaches of WHO International Family Classifications.” Aging Medicine 3(2): 82-94. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7338700/ [Accessed 26th January 2021].
[xxvii] Asly, M. and A. Hazim “Rehabilitation of post-covid-19 patients.” Pan African Medical Journal 36: 1-3. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7467884/pdf/PAMJ-36-168.pdf [Accessed 26th January 2021].
[xxviii] Bernardi, E., et al. (2020). “Late Breaking Abstract – Exercise rehabilitation in telemedicine for COVID-19 patients.” European Respiratory Journal. Conference: European Respiratory Society International Congress, ERS 56. https://erj.ersjournals.com/content/56/suppl_64/882 [Accessed 26th January 2021].
[xxix] Jain, S. and L. Santhosh “On treatments and tests deferred: Preparing for collateral damage from COVID-19.” Annals of the American Thoracic Society 17(11): 1371-1373. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7640720/ [Accessed 26th January 2021].
[xxx] Sebio-Garcia, R. “Pulmonary rehabilitation: Time for an upgrade.” Journal of Clinical Medicine 9(9): 1-4. https://pubmed.ncbi.nlm.nih.gov/32854317/ [Accessed 26th January 2021].
[xxxi] Tur, B. S. and D. Evcik (2020). “Is Physical Medicine and Rehabilitation needed much more for COVID-19 pandemic?” Turkish Journal of Physical Medicine and Rehabilitation 66(2): 101-103. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7401683/ [Accessed 26th January 2021].
[xxxii] Gautam, A. P., et al. (2020). “Pulmonary rehabilitation in COVID-19 pandemic era: The need for a revised approach.” Respirology (Carlton, Vic.) 25(12): 1320-1322. https://pubmed.ncbi.nlm.nih.gov/32954580/
[Accessed 26th January 2021].[xxxiii] Polgar O, Aljishi M, Barker RE, Patel S, Walsh JA, Kon SS, Man WD, Nolan CM. Digital habits of PR service-users: Implications for home-based interventions during the COVID-19 pandemic. Chron Respir Dis. 2020 Jan-Dec;17:1479973120936685. doi: 10.1177/1479973120936685. PMID: 32602361; PMCID: PMC7328358.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7328358/ [Accessed 26th January 2021].
[xxxiv] McIntyre, M., et al. (2020). “Practical Considerations for Implementing Virtual Care in Physical Medicine and Rehabilitation: For the Pandemic and Beyond.” American journal of physical medicine and rehabilitation 99(6): 464-467. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7253038/ [Accessed 26th January 2021].
[xxxv] Pinto, M., et al. “Post-acute covid-19 rehabilitation network proposal: From intensive to extensive and home-based it supported services.” International Journal of Environmental Research and Public Health 17(24): 1-14. https://pubmed.ncbi.nlm.nih.gov/33327384/ [Accessed 26th January 2021].
[xxxvi] Prvu Bettger, J., et al. (2020). “COVID-19: maintaining essential rehabilitation services across the care continuum.” BMJ global health 5(5). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7228480/ [Accessed 26th January 2021].
[xxxvii] Zhu, S., et al. (2021). “Reconfigure rehabilitation services during the Covid-19 pandemic: best practices from Southwest China.” Disability and rehabilitation 43(1): 126-132. https://pubmed.ncbi.nlm.nih.gov/33280457/ [Accessed 26th January 2021].
[xxxviii] Hong Zhang, Hui Zhang, Xiangeng Zhang, Jiaqin Yu. The effectiveness of respiratory rehabilitation for patients with coronavirus-related pneumonia (COVID-19, SARS, MERS): a systematic review and meta-analysis. PROSPERO 2020 CRD42020202011 . Available from: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42020202011[Accessed 26th January 2021].
[xxxix] Gonzalez-Gerez, J. J., et al. (2020). “Therapeutic pulmonary telerehabilitation protocol for patients affected by COVID-19, confined to their homes: study protocol for a randomized controlled trial.” Trials 21(1): 588. https://pubmed.ncbi.nlm.nih.gov/32600378/ [Accessed 26th January 2021].
[xl] Koc, U. (2020) “Tele-rehabilitation Versus Home Exercise Program in COVID-19.” ClinicalTrials.gov. https://clinicaltrials.gov/show/NCT04482634 [Accessed 26th January 2021].
[xli] McGregor, G., et al. (2021). “Rehabilitation Exercise and psycholoGical support After covid-19 InfectioN’ (REGAIN): a structured summary of a study protocol for a randomised controlled trial.” Trials 22(1). https://pubmed.ncbi.nlm.nih.gov/33407804/ [Accessed 26th January 2021].
[xlii] Smits, M., et al. (2020). “Could Virtual Reality play a role in the rehabilitation after COVID-19 infection?” BMJ open sport and exercise medicine 6(1): e000943. https://pubmed.ncbi.nlm.nih.gov/33178449/ [Accessed 26th January 2021].
[xliii] Wang D et al. (2020) Protocol for a systematic review and meta-analysis of respiratory rehabilitation following intensive care unit discharge for COVID-19 survivors. BMJ Open. 2020 Dec 8;10(12):e041184. doi: 10.1136/bmjopen-2020-041184.
Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7725092/ [Accessed 26th January 2021].
[xliv] Zhu F, Zhang M, Gao M, Zeng C, Wang D, Hong Q, Chen W. Effects of respiratory rehabilitation on patients with novel coronavirus (COVID-19) pneumonia in the rehabilitation phase: protocol for a systematic review and meta-analysis. BMJ Open. 2020 Jul 13;10(7):e039771. doi: 10.1136/bmjopen-2020-039771. https://pubmed.ncbi.nlm.nih.gov/32665352/ [Accessed 26th January 2021].
[xlv] Leeds Teaching Hospital (2020) COVID-19 patient rehabilitation booklet Information for patients. https://rapidinfo4u.healthcare/ufaqs/covid-19-patient-rehabilitation-booklet-information-for-patients/ [Accessed 26th January 2021].
[xlvi] Dept of Physiotherapy, University Hospital Limerick (2020)
A Progressive Muscle Relaxation script for Pulmonary Rehabilitation https://rapidinfo4u.healthcare/ufaqs/progressive-muscle-relaxation-for-pulmonary-rehabilitation/ [Accessed 26th January 2021].
[xlvii] BMJ Best Practice (2020). COVID-19.
https://bestpractice.bmj.com/topics/en-gb/3000168/ [Accessed 26th January 2021].
[xlviii] Coronavirus disease 2019 (COVID-19): Evaluation and management of adults following acute viral illness https://www.uptodate.com/contents/coronavirus-disease-2019-covid-19-evaluation-and-management-of-adults-following-acute-viral-illness?search=virtual%20pulmonary%20rehabilitation%20covid-19 andsource=search_result andselectedTitle=1~150 andusage_type=default anddisplay_rank=1 [Accessed 26th January 2021].
Produced by the members of the National Health Library and Knowledge Service Evidence Team†. Current as at 30 October 2020. This evidence summary collates the best available evidence at the time of writing and does not replace clinical judgement or guidance. Emerging literature or subsequent developments in respect of COVID-19 may require amendment to the information or sources listed in the document. Although all reasonable care has been taken in the compilation of content, the National Health Library and Knowledge Service Evidence Team makes no representations or warranties expressed or implied as to the accuracy or suitability of the information or sources listed in the document. This evidence summary is the property of the National Health Library and Knowledge Service and subsequent re-use or distribution in whole or in part should include acknowledgement of the service.
Maura Flynn, Librarian, Midland Regional Hospital, Tullamore, Co. Offaly [Author]. Ms. Sinead O’Neill, Health Information and Quality Authority [Editor]

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.