
What is the incidence and severity of SARS-CoV-2 infection in infants and children?
Question 212 was prepared by the National Health Library and Knowledge Service in collaboration with the Research Subgroup of the National Immunisation Advisory Committee (NIAC).The following information resources have been selected by the National Health Library and Knowledge Service Evidence Virtual Team in response to a question from the National Immunisation Advisory Committee (NIAC). The resources are listed in our estimated order of relevance to practicing healthcare professionals confronted with this scenario in an Irish context. In respect of the evolving global situation and rapidly changing evidence base, it is advised to use hyperlinked sources in this document to ensure that the information you are disseminating to the public or applying in clinical practice is the most current, valid and accurate. For further information on the methodology used in the compilation of this document ¾ including a complete list of sources consulted ¾ please see our National Health Library and Knowledge Service Summary of Evidence Protocol.
Download Full Summary of Evidence (PDF)
Main Points
Epidemiology
- Children have a lower susceptibility to infection compared with adults (OR 0.56 (95% CI, 0.37-0.85)).
- Hospitalization rates are significantly lower in children than in adults with COVID-19. Underlying conditions are associated with higher rates of hospitalization and ICU admission.
- Deaths in children due to COVID-19 have been extremely rare (0.17 per 100,000).
Severity of Illness
- Most children infected with SARS-COV-2 present with mild symptoms or are asymptomatic, and experience a milder course of disease; only ~1% develop severe or life-threatening disease.
- Children with medical complexity, with genetic, neurologic or metabolic conditions, or with congenital heart disease may be at increased risk for severe illness from COVID-19.
- Tsankov et al report a higher risk of severe COVID-19 (relative risk ratio (RRR) 1.79 (95% CI 1.27 – 2.51)) and a higher risk of mortality (RRR 2.81 (95% CI 1.31 – 6.02)) among children with comorbidities than for healthy children. Children with obesity had a RRR of 2.87 (95% CI 1.16 – 7.07).
- Children with severe COVID-19 may develop respiratory failure, myocarditis, shock, acute renal failure, coagulopathy and multi-organ system failure.
Multisystem Inflammatory Syndrome in Children (MIS-C)
- MIS-C appears to be a relatively rare complication, occurring in less than 1% of children with confirmed SARS-CoV-2 infection.
- Although uncommon and generally treatable, MIS-C presents potentially life-altering medical sequelae, complicated by a dearth of information regarding its etiology, pathophysiology and long-term outcomes.
- Tang et al report that patients with MIS-C present with symptoms more severe than children with acute COVID-19 disease, with fever and gastrointestinal symptoms as primary manifestations and multisystem involvement, particularly the cardiovascular system.
‘Long’ COVID
- There is some emerging evidence of persisting symptoms both in children with initial symptomatic and asymptomatic COVID-19; symptoms include insomnia, respiratory symptoms including pain and chest tightness, nasal congestion, fatigue, muscle and joint pain, and concentration difficulties.
Transmission
- The role of children in transmitting the virus may be limited, with several studies suggesting that children are rarely the primary source of secondary transmission of SARS-CoV-2 in the household or in child care or school settings.
- Viner et al report a pooled odds ratio of being an infected contact in children compared with adults of 0.56 (95% CI, 0.37-0.85).
- Data that continue to be published throughout the world demonstrate that children are unlikely to contract COVID-19 from contact within schools and that household transmission is the mode of contact which is most likely to result in the spread of COVID-19.
Vaccination
- In an ongoing multinational randomized controlled trial, no vaccine-related severe adverse events have been observed among adolescents receiving the Pfizer-BioNTech COVID-19 vaccine.
Summary of Evidence
EPIDEMIOLOGY
Fewer cases of COVID-19 have been reported in children aged 0-17 years compared with adults1, 2, and evidence suggests that children have a lower susceptibility to infection compared with adults (OR 0.56 (95% CI, 0.37-0.85))38. In a retrospective cohort study of 135,000 patients in the United States, Leidman et al12 reported that incidence and positive test results among children aged 0-10 years were consistently lower than those in older age groups; and that 2.5% of children were hospitalized, 0.8% required ICU admission and less than 0.1% died, compared with 16.6%, 8.6% and 5.0% among adults aged ≥25 years.
Although in general children consistently comprise 1%-5% of total case numbers2, the true incidence of SARS-CoV-2 infection in children is not known due to the absence of widespread community or serological testing and the prioritization of testing for adults and those with severe illness1, 2; infection rates in children and adolescents also vary according to geographical location3.
Hospitalization rates are significantly lower in children than in adults with COVID-19, suggesting that children may have less severe illness from COVID-19 compared to adults1. In Britain, a prospective observational cohort study found that children and young adults represented 0.9% of all hospitalized patients1. Among almost 70,000 laboratory-confirmed cases of COVID-19 in children reported to the CDC in the United States by 20 May 2020, the hospitalization rate ranged from 2.5% to 4.1%. Among children hospitalized with COVID-19 by late July 2020, approximately 33% required intensive care and 6% required mechanical ventilation4.
In CDC surveillance of COVID-19 in the United States, underlying conditions are associated with higher rates of hospitalization (15%-22% vs. 2%-4%) and ICU admission (4%-5% vs. <1%). Age of less than 1 year has also been associated with increased rates of hospitalization, although hospitalization of infants may not reflect severity of disease4.
Deaths in children due to COVID-19 have been extremely rare, similar to the incidence seen every year with seasonal influenza: mortality seems to be consistent at around 0.01%-0.1%2, 23. In pooled analysis from 7 countries, the COVID-19-related death rate among children aged 0-19 years as of February 2021 was 0.17 per 100,0004.
Globally, the case fatality rate in children appears to be higher in low- and middle-income countries compared with high-income countries3, 6.
SEVERITY OF ILLNESS
Most children infected with SARS-COV-2 present with mild symptoms or are asymptomatic, and experience a milder course of disease; only ~1% develop severe or life-threatening disease2.
However, some children are still at risk of developing severe illness and complications from COVID-191. Current evidence suggests that children with medical complexity, with genetic, neurologic or metabolic conditions, or with congenital heart disease may be at increased risk for severe illness from COVID-19. Similar to adults, children with obesity, diabetes, asthma or chronic lung disease, sickle cell disease or immunosuppression may also be at increased risk for severe illness from COVID-191, 4, 5, 8, 17, 18, 44. Among 121 SARS-CoV-2-associated deaths in children and adolescents in the United States, 75% had at least one underlying medical condition, and 45% had at least two underlying conditions. Chronic pulmonary disease (28%), obesity (27%), neurologic and developmental conditions (22%) and cardiovascular conditions (18%) were the most frequently reported4. Among children hospitalized with COVID-19 in the United States to late July 2020, 42% had at least one underlying condition, the most common of which were obesity (38% of children >2 years), chronic pulmonary disease (18%) and prematurity (15% of children <2 years). In a systematic review of 9,335 hospitalized and outpatient children with laboratory-confirmed COVID-19 and information about comorbidities, 27% had an underlying condition, with immunosuppression (16%) and lung disease (13%) most common4. Tsankov et al8 report a higher risk of severe COVID-19 (RRR 1.79 (95% CI 1.27 – 2.51; I2 = 94%)) and a higher risk of mortality (RRR 2.81 (95% CI 1.31 – 6.02; I2 = 82%)) among children with comorbidities than for healthy children. Children with obesity had a RRR of 2.87 (95% CI 1.16 – 7.07; I2 = 36%).
In a multicenter study of paediatric patients hospitalized with acute SARS-CoV-2, Fernandes et al17identified that younger age (aOR 1.09 per 1-year decrease, 95% CI 1.02-1.16), obesity (aOR 3.39, 95% CI 1.26-9.10), increasing white blood cell count (aOR 1.11 per unit increase in 109/L, 95% CI 1.03-1.20), hypoxia (aOR 4.01, 95% CI 1.14-14.15) and bilateral infiltrates on chest radiograph (aOR 3.69, 95% CI 1.46-9.32) at admission were independent predictors of severe disease. Graff et al18 found that age 0-3 months or older than 20 years, comorbid conditions and elevated C-reactive protein were predictors of severe disease in children. Götzinger et al21 identified that age younger than 1 month (OR 5.06, 95% CI 1.72-14.87; p=0.0035), male sex (2.12, 1.06-4.21; p=0.033), pre-existing medical conditions (3.27, 1.67-6.42; p=0.0015), and presence of lower respiratory tract infection signs or symptoms at presentation (10.46, 5.16-21.23; p<0.0001) were predictors of ICU admission; and that 52% of 48 children admitted to ICU had a known comorbidity, with previous chronic pulmonary disease (13%) the most common predictor of ICU admission.
While healthcare providers should maintain a high index of suspicion for SARS-CoV-2 infection in these populations and monitor the progression of illness closely, most children appear to have asymptomatic, mild or moderate disease, and recover within 7 to 14 days of disease onset4. Although Meena et al11 report increased severity, morbidity and mortality of COVID-19 in paediatric oncology compared to the general paediatric population, most infants and children with certain underlying conditions such as cancer who are infected with SARS-CoV-2 do not usually develop severe COVID-19 illness1, 4, 11.
Why COVID-19 appears to be less common and less severe in children is uncertain. Possibilities include a less intense immune response to the virus; viral interference in the respiratory tract of young children, which may lead to a lower SARS-CoV-2 viral load; different expression of the ACE2 receptor (the receptor for SARS-CoV-2) in the respiratory tract of children; pre-existing cross-reactive antibody; a vigorous early mucosal immune response; and relatively healthier blood vessels in children than in adults. In addition, the possibility of decreased exposure and decreased rates of testing in children may be significant4.
Similar to adults, children with severe COVID-19 may develop respiratory failure, myocarditis, shock, acute renal failure, coagulopathy and multi-organ system failure. Some children with COVID-19 have developed other serious problems such as intussusception or diabetic ketoacidosis. Children infected with SARS-CoV-2 are also at risk for developing Multisystem Inflammatory Syndrome in Children (MIS-C)1.
MULTISYSTEM INFLAMMATORY SYNDROME IN CHILDREN (MIS-C)
While the incidence of MIS-C is uncertain, it appears to be a relatively rare complication, occurring in less than 1% of children with confirmed SARS-CoV-2 infection. In one report from the United States, the estimated incidence of laboratory-confirmed SARS-CoV-2 infection in individuals younger than 21 years was 32 per 100,000; and the incidence of MIS-C was 2 per 100,0005. Although uncommon and generally treatable, MIS-C presents potentially life-altering medical sequelae, complicated by a dearth of information regarding its etiology, pathophysiology and long-term outcomes34.
The first report of MIS-C was a series of 8 children in South East England. In subsequent larger case series in Britain and the United States, more than 70% of affected children were previously healthy. The most common comorbidities were obesity and asthma. Tang et al26 report that patients with MIS-C present with symptoms more severe than children with COVID-19, with fever and gastrointestinal symptoms as primary manifestations and multisystem involvement, particularly the cardiovascular system.
Radia et al27 report that patients with MIS-C were noted to have a high frequency of gastrointestinal symptoms (71%) including abdominal pain (34%) and diarrhoea (27%). Cough and respiratory distress were reported in 4.5% and 9.6% of cases, respectively. Blood parameters showed neutrophilia in 83% and a high C-reactive protein in 94% of cases. Comorbidities were reported in 20% of cases, with obesity the most frequent (7.7%). Severity of illness was high with 68% of cases requiring ICU admission, 63% inotropic support, 28% some form of respiratory support, and 4% extra-corporeal membrane oxygenation. Treatment strategies included intravenous immunoglobulin (63%) and intravenous steroids (44%). 1.5% of children died.
In a retrospective surveillance study, Abrams et al28 found that ICU admission was more likely in patients aged 6-12 years (aOR 1.9 [95% CI 1.4-2.6]) and patients aged 13-20 years (aOR 2.6 [1.8-3.8]), compared with patients aged 0-5 years. Compared with patients aged 0–5 years, patients aged 6–12 years had higher odds of shock (aOR 1.7 [1.2–2.3]) and decreased cardiac function (aOR 1.7 [1.2–2.5]); and patients aged 13–20 years had substantially higher odds of shock (aOR 2.5 [1.8–3.7]), decreased cardiac function (aOR 2.4 [1.6–3.7]), and myocarditis (aOR 2.6 [1.6–4.2]). Obesity was linked to decreased cardiac function (aOR 1.4 [1.0–1.9]. Coronary artery abnormalities were more common in male patients (aOR 1.5 [1.1-2.1]) than in female patients; and in patients with mucocutaneous lesions (aOR 2.2 [1.3-3.5]) or conjunctival injection (aOR 2.3 [1.4-3.7]).
Rates of MIS-C appear to vary by race and ethnicity, with Black and Hispanic children accounting for a disproportionately high number of cases and Asian children accounting for a disproportionately low number of cases5, 28, 29.
In a cohort study of 56 children in Brazil, Lima-Setta et al31 reported that gastrointestinal symptoms were present in 71%, shock symptoms in 59%, and severe respiratory symptoms in less than 20%. The median length of ICU stay was 6 days (IQR 5-11), and one death occurred (1.8%). Similarly, in a surveillance study of 186 patients with MIS-C in the United States, Feldstein et al32 found that organ-system involvement included the gastrointestinal system in 171 patients (92%), cardiovascular in 149 (80%), hematologic in 142 (76%), mucocutaneous in 137 (74%), and respiratory in 131 (70%). The median duration of hospitalization was 7 days (IQR 4 to 10); 148 patients (80%) received intensive care; 37 (20%) received mechanical ventilation; 90 (48%) received vasoactive support; and 4 (2%) died.
Among 95 patients with confirmed and 4 with suspected MIS-C in New York, Dufort et al33 report that all presented with subjective fever or chills; 97% had tachycardia; 80% had gastrointestinal symptoms; 60% had rash; 56% had conjunctival injection; and 27% had mucosal changes. Elevated levels of C-reactive protein, D-dimer and troponin were found in 100% of children aged 0-5, 91% of children aged 6-11 and 71% of the patients aged 13-20. 62% received vasopressor support; 53% had evidence of myocarditis; 80% were admitted to ICU; and 2 died. The median length of hospital stay was 6 days.
‘LONG’ COVID-19
In a cross-sectional study of 129 children diagnosed with COVID-19 between March and November 2020, Buonsenso et al24 found that after the initial diagnosis of COVID-19, 41.8% completely recovered; 35.7% had one or two persisting symptoms; and 22.5% had three or more persisting symptoms. Insomnia (18.6%); respiratory symptoms including pain and chest tightness (14.7%); nasal congestion (12.4%); fatigue (10.8%); muscle (10.1%) and joint (6.9%) pain; and concentration difficulties (10.1%) were the most frequently reported symptoms. These symptoms – described both in children with symptomatic and asymptomatic acute COVID-19 – were particularly frequent in those assessed more than 60 days after the initial diagnosis.
TRANSMISSION
The importance of children in transmitting the virus is difficult to establish, particularly because of the number of asymptomatic cases, but there is some evidence that their role in transmitting the virus is limited2, 13. Early studies of multiple family clusters in China, Israel and other countries have revealed that children were unlikely to be the index case. A SARS-CoV-2 positive child in a cluster in the French Alps did not transmit the virus to anyone else, despite exposure to more than 100 people2.
In the Netherlands, separate data from primary care and household studies suggests SARS-CoV-2 is mainly spread between adults and from adult family members to children2. A family-based Norwegian study has shown that while adults are most often the index case, the onward transmission of SARS-CoV-2 within a family is highest when the index case is an adult or a child aged 0-6 years, possibly due to the close contact that occurs between younger children and others in the family2. Siebach et al45 assert that based on current evidence, children are rarely the primary source of secondary transmission in the household or in child care or school settings, and are more likely to contract the virus from an adult household member. In a living systematic review, Xu et al37 cite 5 cohort studies which report an infection attack rate for students and school staff of 0.15% (95% CI = 0.00%-0.93%) and 0.70% (95% CI = 0.00%-3.56%), respectively; and 6 cross-sectional studies which estimate a SARS-CoV-2 positivity rate of 8.74% (95% CI = 2.34%-18.53%) among students, compared with 13.68% (95% CI = 1.68%-33.89%) among school staff. Viner et al38 report a pooled odds ratio of being an infected contact in children compared with adults of 0.56 (95% CI, 0.37-0.85), although with substantial heterogeneity among the studies included in their systematic review. In an epidemiological study where 1,155 contacts of 6 COVID-19 positive cases in an Irish school were screened, there was no evidence of secondary transmission of COVID-19 from children to other children or adults, with the findings mirrored in a study from Singapore2. A German study screened contacts of 137 children who attended school for at least one day when presumed infective ¾ i.e. one day before symptoms started ¾ before the child isolated. Six index cases were found to have infected 11 additional pupils, with no onward transmission identified for the other 131 children who attended school2. An Australian study in secondary schools showed a low rate of child-to-child transmission (0.3%-1.2%), with adult-to-child (1.5%) and adult-to-adult (4.4%) transmission being more common2.
However, viable SARS-CoV-2 virus has been isolated from symptomatic children with COVID-19 and there is some evidence of transmission from asymptomatic children to others2, 37. Recent evidence suggests that children have similar viral loads in their nasopharynx1, 4, 42, similar secondary infection rates, and can spread the virus to others; viral load is reported to be highest in children in the first 2 days of symptoms42. Li et al40 caution that the transmissibility of paediatric COVID-19 should not be ignored because of the relatively long incubation period (9.57 days (95% CI 7.70-11.44)), shedding duration (11.43 days), and mild clinical symptoms.
Data that continue to be published throughout the world demonstrate that children are unlikely to contract COVID-19 from contact within schools and that household transmission is the mode of contact which is most likely to result in the spread of COVID-19. Maintaining interventions including social distancing, hand washing and, when appropriate, wearing masks, appear to be effective measures to reduce in-school transmission of COVID-192.
VACCINATION
In an ongoing multinational randomized controlled trial, no vaccine-related severe adverse events have been observed among adolescents receiving the Pfizer-BioNTech COVID-19 vaccine46. In a case series of adolescents of 16 years (or older) diagnosed with perimyocarditis following vaccination with the Pfizer-BioNTech COVID-19 vaccine in Israel, although incidence of perimyocarditis during the vaccination period was elevated in comparison to previous years, all cases were mild and all patients’ symptoms resolved rapidly with no requirement for cardiovascular or respiratory support47, 48.
Irish and/or International Guidance
| Level 1 |
World Health Organization (2020) Information for Paediatric Healthcare Providers[1]
This guidance is intended to inform paediatric healthcare providers of up-to-date information about children with suspected or confirmed COVID-19 and about caring for children during the pandemic.
See Section: Infections Among Children
Incidence of COVID-19 in Children
In the United States and globally, fewer cases of COVID-19 have been reported in children (age 0-17 years) compared with adults. While children comprise 22% of the US population, the most recent data show that some cases of COVID-19 in the United States reported to CDC were among children. The number and rate of cases in children in the United States have been steadily increasing since March 2020. The true incidence of SARS-CoV-2 infection in children is not known due to the absence of widespread testing and the prioritization of testing for adults and those with severe illness. Hospitalization rates in children are significantly lower than hospitalization rates in adults with COVID-19, suggesting that children may have less severe illness from COVID-19 compared to adults.
Infections and Transmission Among Children
Recent evidence suggests that compared to adults, children likely have similar viral loads in their nasopharynx, similar secondary infection rates, and can spread the virus to others.
Due to community mitigation measures and school closures, transmission of SARS-CoV-2 to and among children may have been reduced in the United States during the pandemic in the spring and early summer of 2020. This may explain the low incidence in children compared with adults. Comparing trends in paediatric infections before and after the return to child care, in-person school, youth sports and other activities may enhance our understanding about infections in children.
Severity of Illness in Children
While children infected with SARS-CoV-2 are less likely to develop severe illness compared with adults, children are still at risk of developing severe illness and complications from COVID-19. Weekly COVID-19 hospitalization surveillance data show that the rate of hospitalization among children is low compared with that of adults, but hospitalization rates among children are increasing. About 1 in 3 children hospitalized with COVID-19 in the United States were admitted to the Intensive Care Unit, similar to the rate among adults.
Current evidence suggests that children with certain underlying medical conditions and infants (age <1 year) may be at increased risk for severe illness from SARS-CoV-2 infection. Of the children who have developed severe illness from COVID-19, most have had underlying medical conditions. There is limited evidence about which underlying medical conditions in children might increase the risk for severe illness. Current evidence suggests that children with medical complexity, with genetic, neurologic or metabolic conditions, or with congenital heart disease may be at increased risk for severe illness from COVID-19. Similar to adults, children with obesity, diabetes, asthma or chronic lung disease, sickle cell disease or immunosuppression may also be at increased risk for severe illness from COVID-19.
While healthcare providers should maintain a high index of suspicion for SARS-CoV-2 infection in these populations and monitor the progression of illness closely, it appears that most infants and children with certain underlying conditions such as cancer who are infected with SARS-CoV-2 do not usually develop severe COVID-19 illness.
Hospitalization rates in the United States are higher among Hispanic/Latino children and non-Hispanic Black children compared with non-Hispanic White children. Studies of hospitalized children have found that obesity was the most prevalent underlying condition. Additional studies are needed to identify the association between SARS-CoV-2 infection and obesity to find possible clinical interventions and strategies to reduce hospitalization risk.
Similar to adults, children with severe COVID-19 may develop respiratory failure, myocarditis, shock, acute renal failure, coagulopathy and multi-organ system failure. Some children with COVID-19 have developed other serious problems such as intussusception or diabetic ketoacidosis. Children infected with SARS-CoV-2 are also at risk for developing Multisystem Inflammatory Syndrome in Children (MIS-C).
| Level 1 |
Royal College of Paediatrics and Child Health (Great Britain) (2021) COVID-19 Research Evidence Summaries[2]
See Section: Epidemiology
Can children and young people suffer from COVID-19 disease?
COVID-19 disease has been reported in children and young people of all ages, including shortly after birth. There have been far fewer confirmed cases of COVID-19 disease in children than adults: children consistently comprise 1%-5% of total case numbers in reports.
Publications about acute infection suggest that there are comparatively few children infected by SARS-CoV-2 and thus suffering from COVID-19 disease in the community. Community surveillance systems suggest teenagers are more susceptible to COVID-19 disease than younger children.
Does COVID-19 affect children and young people in the same way as adults?
Infection with SARS-CoV-2 appears to take a milder course in children than in adults: most infected children present with mild symptoms or are asymptomatic, and very few (~1%) develop severe or life-threatening disease. In the absence of widespread community or serological testing, it is difficult to ascertain the proportion with sub-clinical symptoms.
Within households, secondary attack rates in children have generally been shown to be lower than in adults, suggesting that they have a reduced susceptibility to infection. It is speculated that differences in the expression of Angiotensin Converting Enzyme 2 Receptor may play a role in altering the susceptibility of children to infection.
More recently, understanding of the innate and adaptive immune response to SARS-CoV-2 has been progressed. An Australian study has demonstrated a reduction in monocyte and dendritic cells after SARS-CoV-2 infection, which recover in convalescence. Interestingly, they also showed that there is a significant increase in CD63+ neutrophils associated with the release of pro-inflammatory mediators which has not been shown in adult studies, suggesting that there may be differences in the innate immune response to infection in adults and children.
A study in Britain has shown that children not previously infected with SARS-CoV-2 have much higher levels of cross-reactive IgG antibodies compared to young adults. Differences in antibody response to SARS-CoV-2 infection have been shown with young children having higher anti-S IgG antibodies compared to teens ¾ the S protein of SARS-CoV-2 binds to the cellular receptor for viral entry to the cell ¾ and increasing levels of anti-N IgG antibody with age. N protein release requires lysis of infected cells so lower levels of anti-N antibody may reflect the milder disease course in children. Understanding the antibody response in different age groups is important when considering how to screen for previous exposure to SARS-CoV-2 and to gain more complete understanding of the epidemiology of the disease, as demonstrated in a large serosurveillance study from the Netherlands. At this point in time the clinical utility of antibody testing is unclear.
Deaths in children due to COVID-19 have been extremely rare, similar to the incidence seen every year with seasonal influenza: mortality seems to be consistent at around 0.01%-0.1%.
What role does ethnicity have in COVID-19 infection?
The impact of ethnicity in COVID-19 infection has not been fully elucidated. However, it has been noted that a high proportion of neonates affected by COVID-19 infection are from Black, Asian or minority ethnic groups. The largest British study of children with COVID-19 in hospital found that children of Black ethnicity were over-represented compared to the population representation and that Black ethnicity was associated with an increased likelihood of requiring critical care admission. A US study 0f 135,800 children found that while children of Black and Hispanic ethnicity were less likely to have undergone testing for SARS-CoV-2 than Caucasian children, when they were tested they were more likely to be SARS-CoV-2 positive, which has been corroborated in other large series. It was found that 69% of children with Paediatric Inflammatory Multisystem Syndrome (PIMS-TS) in Britain were of Black or Asian race. The reasons for these differences are not clear.
Transmission
Are children as likely as adults to acquire COVID-19?
Evidence suggests that children may be less likely to acquire the disease. This is supported in countries that have undertaken widespread community testing, where lower case numbers in children than adults have been found. Between 16 January and 3 May 2020, 35,200 children in England were swabbed for SARS-CoV-2 and 1,408 (4%) were positive. Children under 16 years old accounted for only 1.1% of positive cases.
Can children transmit the virus?
The importance of children in transmitting the virus is difficult to establish, particularly because of the number of asymptomatic cases, but there is some evidence that their role in transmitting the virus is limited, and older index case age has been associated with an increased rate of secondary infections. Early studies of multiple family clusters in China, Israel and other countries have revealed that children were unlikely to be the index case. A SARS-CoV-2 positive child in a cluster in the French Alps did not transmit the virus to anyone else, despite exposure to more than 100 people.
In the Netherlands, separate data from primary care and household studies suggests SARS-CoV-2 is mainly spread between adults and from adult family members to children. These findings are supported by a similar study from Greece. A family-based Norwegian study has shown that while adults are most often the index case, the onward transmission of SARS-CoV-2 within a family is highest when the index case is an adult or a child aged 0-6 years, possibly due to the close contact that occurs between younger children and others in the family. An American study has analysed variables which may be associated with a higher secondary household attack rate and has found that higher living density, being a partner of the index case, having a BMI >30Kg/m2 and the index case being non-White are significantly associated with higher secondary attack rates.
In an epidemiological study where 1,155 contacts of 6 COVID-19 positive cases in an Irish school were screened, there was no evidence of secondary transmission of COVID-19 from children to other children or adults, with the findings mirrored in a study from Singapore. A German study screened contacts of 137 children who attended school for at least one day when presumed infective ¾ ie one day before symptoms started ¾ before the child isolated. 6 index cases were found to have infected 11 additional pupils, with no onward transmission identified for the other 131 children who attended school.
However, viable SARS-CoV-2 virus has been isolated from symptomatic children with COVID-19 and there is some evidence of transmission from asymptomatic children to others. Analysis of large outbreaks of COVID-19 disease in summer camps were unable to differentiate between transmission from adults to children and between children themselves, but up to 90% of exposed attendees who had not previously had COVID-19 contracted the virus. It is likely that multiple chains of contact account for the high infection rates and supports the notion of limiting contact outside classrooms and having “bubbles” for schools, to reduce the exposure of individuals to the virus.
Fastidious additional measures including daily temperature checks, face-masks at all times, desk spacing, half-day schooling and staggered arrival and departure time have been cited as interventions which may have resulted in low transmission rates in Hong Kong. This is supported by an Israeli study into a secondary school outbreak of two separate cases of COVID-19 in students, 13.2% of students and 16.6% of staff subsequently tested positive for SARS-CoV-2. Untangling the modes of transmission ¾ increased community spread due to loosening of lockdown restrictions vs. school contact ¾ was not possible but avoiding poorly ventilated closed spaces, crowded areas and close-contact settings is recommended.
An Australian study in secondary schools showed a low rate of child-to-child transmission (0.3%-1.2%), with adult-to-child (1.5%) and adult-to-adult (4.4%) transmission being more common, something which is reflected in other transmission studies. Low community prevalence levels in combination with effective contact tracing enabled a rapid response, which may explain why the levels of onward infection appear to be much lower in this study.
Public Health England collected data on transmission related to school settings during June 2020, when a limited number of school years were invited to return to school. Nationally there were 198 confirmed cases related to educational settings and 1.6 million (mainly primary school aged) children were reported to have returned to school. When the index case was a child the maximum number of secondary cases was 2, compared to 9 when the index case was a staff member. When outbreaks were reported this was significantly associated with increased rates of regional prevalence. Data that continue to be published throughout the world demonstrate that children are unlikely to contract COVID-19 from contact within schools and that household transmission is the mode of contact which is most likely to result in the spread of COVID-19. Overall this is very reassuring for children returning to school but highlights the importance of household isolation when a person within the household is positive for COVID-19. Maintaining interventions including social distancing, hand washing and, when appropriate, wearing masks, appear to be effective measures to reduce in-school transmission of COVID-19.
A US study comparing the change in overall incidence of COVID-19 in children between ongoing remote teaching and a return to in-person teaching of children of all ages found an increase in incidence 20 days after schools re-opened for in-person teaching. This was more marked for children in high school. There are several confounders within the study which may impact the results: higher starting incidence of COVID-19 in areas with in-person teaching; community rates not described; different public health policies.
Importantly for adults aged 65 years and under, living with children of any age is associated with a lower risk of dying from COVID-19 and for adults over 65 years there is no effect on mortality. There is a slight increased risk of developing COVID-19 infection for adults 65 years and under when living with children aged 12-18 years old but this is not associated with needing admission to hospital, ICU or death.
What is the duration of viral shedding in nasopharyngeal or throat swabs?
The duration of viral shedding in nasopharyngeal or throat swabs has been reported in children to range from 6-22 days, with mean reported at 12 days vs. median 8 days. Saliva has been assessed as an alternative method of SARS-CoV-2 detection but is found to be less sensitive than nasopharyngeal or throat swabs.
Neonatal
Are neonates at increased risk of severe disease?
Many case reports or series have been published investigating the outcomes of pregnant mothers with COVID-19 and their newborn babies. Mothers and their babies in general appear to do well, with few reports of neonates requiring NICU admission. Early studies suggested that neonates without comorbidities are not at an increased risk of severe disease. However, recent European and British studies have reported that age under one month and prematurity are risk factors for PICU admissions. It is noted in a series of 4 neonates infected after birth that half had additional infections and highlights the importance of screening for additional infections.
Point-of-Care Tools
| Level 2 |
BMJ Best Practice (2021) Coronavirus Disease 2019 (COVID-19)[3]
See Section: EPIDEMIOLOGY
Children
Evidence suggests that children have a lower susceptibility to infection compared with adults, with an odds ratio of 0.56 for being an infected contact compared with adults. Adolescents appear to have similar susceptibility to adults.
The mean age of children with infection is 6.5 years. Infection rates in children and adolescents vary according to geographical location.
In Britain, a prospective observational cohort study found that children and young adults represented 0.9% of all hospitalized patients at the time. The median age of children admitted to hospital was 4.6 years; 56% were male; 35% were under 12 months of age; and 42% had at least one comorbidity. In terms of ethnicity, 57% were White, 12% were South Asian, and 10% were Black. Age under 1 month, age 10 to 14 years, and Black race were risk factors for admission to critical care.
In the US, a retrospective cohort study of over 135,000 children found that the mean age of infected children was 8.8 years, and 53% were male. In terms of ethnicity, 59% were White, 15% were Black, 11% were Hispanic, and 3% were Asian. Only 4% of children tested positive for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in the study population, and clinical manifestations were typically mild. Cases in children, adolescents and young adults increased from October to December 2020; however, hospitalizations, Intensive Care Unit admissions and deaths remain low for these groups: 2.5%, 0.8%, and <0.1% respectively, based on available data.
Globally, the case fatality rate in children appears to be higher in low- and middle-income countries compared with high-income countries.
Most cases in children are from familial clusters, or children who have a history of close contact with an infected patient. It is rare for children to be the index case in household transmission clusters. In contrast to adults, children do not seem to be at higher risk for severe illness based on age or sex.
| Level 2 |
UpToDate (2021) COVID-19: Clinical manifestations and diagnosis in children[4]
See Section: EPIDEMIOLOGY
Children of all ages can get COVID-19. Those <12 to 14 years appear to be affected less commonly than adults, although typically children have a lower risk of exposure than adults and are tested less frequently than adults. In surveillance from various countries, children account for up to 15% of laboratory-confirmed cases.
Age Distribution
Children of all ages can get COVID-19. The incidence increases with increasing age. Among children <18 years in the United States, 1.2 million positive tests for SARS-CoV-2 were recorded from March to December 2020, distributed as follows according to school age-group:
| High School | 14-17 years | 38.3% |
| Middle School | 11-13 years | 18.6% |
| Elementary School | 5-10 years | 25.7% |
| Pre-School | 0-4 years | 17.4% |
Race/Ethnicity
Among adults with COVID-19, underrepresented racial and ethnic groups are disproportionately affected; children from underrepresented racial and ethnic groups also appear to be disproportionately affected by SARS-CoV-2 infection, hospitalization and mortality.
How do children get COVID-19?
In case series early in the pandemic, most cases in children resulted from household exposure, usually with an adult as the index patient. These findings should be interpreted with caution because cases were identified after implementation of strict physical distancing measures (eg school closures), limiting exposure to close contacts outside the household.
In observational studies of household transmission, the secondary attack rate among contacts <18 years of age has ranged from 4% to 57%. In a meta-analysis of 54 studies of household transmission including 77,758 participants from multiple countries, the secondary attack rate was 17% among contacts <18 years, and 28% among adult contacts. In a case-control study, factors associated with SARS-CoV-2 infection in children and adolescents included close contact with persons with COVID-19, typically a household member; having visitors to the home; and attending gatherings with persons outside the household. Healthcare-associated outbreaks and cases of possible transmission from teachers or school staff to students and among students in the school setting have also been reported. In a case-control study, inconsistent mask use at school was associated with SARS-CoV-2 infection, whereas school attendance in itself was not.
Do children transmit SARS-CoV-2 to others?
Children of all ages can transmit SARS-CoV-2 to others, but the rate of transmission by young children is uncertain. Older children and adolescents transmit SARS-CoV-2 effectively in household and community settings. Infected children appear to shed SARS-CoV-2 with nasopharyngeal loads comparable to or higher than those in adults.
- Household Transmission: Limited evidence suggests that transmission from children to household contacts occurs, although the relative frequency of transmission from young children remains uncertain. Household contact studies have identified variable rates of transmission from paediatric index cases. These variable rates may be related to different community prevalence and mitigation measures; methods of diagnosing secondary cases; timing of sample collection; and levels of adherence to infection control measures in the home.
- Transmission in Educational or Child Care Settings: Limited evidence suggests that transmission by pre-adolescent children occurs but is uncommon in educational or child care settings, particularly if the class size is small, public health measures are strictly followed, and community transmission is low. Several studies have documented transmission by adolescents in the school setting, but findings are inconsistent. Transmission by pre-symptomatic children and adolescents also appears to be uncommon in educational settings when effective case-contact testing and epidemic control strategies are implemented. In a prospective cohort from Australia, where most schools remained open during the first wave of the pandemic, among 752 contacts (649 children and 103 adults) of 12 children who attended pre-school, primary school or secondary school while infectious with COVID-19, only 3 secondary infections were identified. In the United States, resumption of in-person primary and secondary education before the emergence of more transmissible variants was associated with relatively few reports of school outbreaks when mitigation strategies such as mask-wearing and classroom cohorting were in place. Two clusters that accounted for 15 of 31 school-associated cases involved probable transmission between teachers followed by transmission from teachers to students. In surveillance in the United States from March to December 2020, the aggregate incidence of SARS-CoV-2 in countries offering in-person pre- and primary school education was similar to the incidence in countries offering online-only pre- and primary school education.
- Transmission by Asymptomatic Children: Although there is little information about transmission of SARS-CoV-2 by asymptomatic (as opposed to pre-symptomatic) children, transmission from children with confirmed asymptomatic SARS-CoV-2 to household contacts has been reported. In addition, there are reports of familiar clusters that included asymptomatic children and possible transmission from asymptomatic children to adults outside their families.
How often do children with COVID-19 require hospitalization?
In population-based surveillance in the United States, the weekly rate of COVID-19-related hospitalization among children <18 years has increased over time, with a cumulative rate of 8 per 100,000. The cumulative rate is highest among children <2 years of age: 24.8 per 100,000.
Despite the trend of increasing hospitalization, a minority of children with COVID-19 require hospitalization. Among almost 70,000 laboratory-confirmed cases of COVID-19 in children reported to the CDC in the United States by 20 May 2020, the hospitalization rate ranged from 2.5% to 4.1%. Among children hospitalized with COVID-19 by late July 2020, approximately 33% required intensive care and 6% required mechanical ventilation.
In CDC surveillance of COVID-19 in the United States, underlying conditions are associated with higher rates of hospitalization (15% to 22% vs. 2% to 4%) and ICU admission (4% to 5% vs. <1%). Age <1 year has also been associated with increased rates of hospitalization, although hospitalization of infants may not reflect severity of disease.
See Section: SEVERE DISEASE IN CHILDREN
Although severe including fatal cases of COVID-19 in children have been reported, most children appear to have asymptomatic, mild or moderate disease, and recover within 1 to 2 weeks of disease onset.
In a systematic review of 7,480 children <18 years of age with laboratory-confirmed COVID-19 infection, information about symptoms and severity was available for 1,475; among these, 15% of cases were asymptomatic, 42% mild, 39% moderate (eg clinical or radiographic evidence of pneumonia without hypoxemia), 2% severe (eg dyspnea, central cyanosis, hypoxemia), and 0.7% critical (eg acute respiratory distress syndrome, respiratory failure, shock). There were 6 deaths in the study population: .08%.
SARS-CoV-2-related death in children and adolescents is rare. In pooled analysis from 7 countries, the COVID-19-related death rate among children aged 0 to 19 years as of February 2021 was 0.17 per 100,000.
Why COVID-19 appears to be less common and less severe in children is uncertain. One possibility is that children have a less intense immune response to the virus. Cytokine release syndrome is thought to be important in the pathogenesis of severe COVID-19 infections. Other possibilities include viral interference in the respiratory tract of young children, which may lead to a lower SARS-CoV-2 viral load; different expression of the angiotensin converting enzyme 2 receptor (the receptor for SARS-CoV-2) in the respiratory tract of children; pre-existing cross-reactive antibody; a vigorous early mucosal immune response; and relatively healthier blood vessels in children than in adults. In addition, the possibility of decreased exposure and decreased rates of testing in children may be significant.
Risk Factors for Severe Disease
Although children with underlying medical conditions are at greater risk for severe disease, robust evidence associating specific underlying conditions with severe disease is limited. The following may be associated with increased risk of severe disease in children:
- medical complexity
- genetic conditions
- neurologic conditions
- metabolic conditions
- congenital heart disease
- obesity
- diabetes
- asthma or other chronic pulmonary diseases
- sickle cell disease
- immunosuppression
Down syndrome has been proposed to predispose to severe disease. Age <1 year has also been associated with increased risk of severe disease, but findings are inconsistent.
In multi-centre studies of children admitted to paediatric ICUs, most children had one or more underlying conditions. Among 121 SARS-CoV-2-associated deaths in children and adolescents [<21 years of age] in the United States, 75% had >1 underlying medical condition, and 45% had >2 underlying conditions. Chronic pulmonary disease (28%), obesity (27%), neurologic and developmental conditions (22%) and cardiovascular conditions (18%) were the most frequently reported. Among children hospitalized with COVID-19 in the United States to late July 2020, 42% had >1 underlying condition, the most common of which were obesity (38% of children >2 years), chronic pulmonary disease (18%) and prematurity (15% of children <2 years). In a systematic review of 9,335 hospitalized and outpatient children with laboratory-confirmed COVID-19 and information about comorbidities, 27% had an underlying condition, with immunosuppression (16%) and lung disease (13%) most common.
Although immune compromise has been reported as an underlying condition in children with severe COVID-19 disease, the relationship of immune compromise to severe COVID-19 has not been well established. In a review if 178 children with cancer from a single institution in the United States, 20 tested positive for SARS-CoV-2, and only one required admission (non-critical) for symptoms related to COVID-19. Disease was similarly mild in small surveys of children who developed COVID-19 while receiving immunosuppressive medications. In a single institution cross-sectional study, the seroprevalence of SARS-CoV-2 in 485 immunocompromised children was 1%, similar to that in immunocompromised children in a companion study; none of the immunocompromised children who tested positive for SARS-CoV-2 had severe disease.
In observational studies, elevated inflammatory markers at admission or during hospitalization, hypoxia at admission and gastrointestinal symptoms at admission have been associated with severe disease in children.
| Level 2 |
UpToDate (2021) COVID-19: Multisystem inflammatory syndrome (MIC-C) in children: clinical features, evaluation, and diagnosis[5]
In children, COVID-19 is usually mild. However, in rare cases, children may be severely affected, and clinical manifestations may differ from adults. In April 2020, reports from Britain documented a presentation in children similar to incomplete Kawasaki disease or toxic shock syndrome. Since then, there have been reports of similarly impacted children in other parts of the world. The condition has been termed multisystem inflammatory syndrome in children (MIS-C).
See Section: EPIDEMIOLOGY
While the incidence of MIS-C is uncertain, it appears to be a relatively rare complication of COVID-19 in children, occurring in <1% of children with confirmed SARS-CoV-2 infection. In one report from the United States, the estimated incidence of laboratory-confirmed SARS-CoV-2 infection in individuals <21 years was 32 per 100,000; and the incidence of MIS-C was 2 per 100,000.
The first report of MIS-C was a series of 8 children in South East England. In subsequent larger case series in Britain and the United States, more than 70% of affected children were previously healthy. The most common comorbidities were obesity and asthma. The median age was 8 to 11 years [range 1 to 20 years]. Rates of MIS-C appear to vary by race and ethnicity, with Black and Hispanic children accounting for a disproportionately high number of cases and Asian children accounting for a disproportionately low number of cases. Typically, cases of MIS-C peak several weeks after surges of COVID-19 in the community.
Irish and/or International Literature
Acute Disease
| Level 1 |
Kitano et al (2021) [Systematic Review] The differential impact of paediatric COVID-19 : a systematic review of fatality and ICU admission[6]
Methods: In order to evaluate the magnitude of global COVID-19 death and Intensive Care Unit (ICU) admission in children aged 0-19 years, a systematic review current to December 7, 2020 was conducted.
Results: 16,027 articles and 225 national reports from 216 countries were reviewed. Among 3,788 global paediatric COVID-19 deaths, 3,394 (91.5%) were reported from low- and middle-income countries (LMIC). 83.5% of the paediatric population from all included countries were from low- and middle-income countries. The paediatric deaths per 1,000,000 children and case fatality rate (CFR) were significantly higher in LMIC than in high-income countries (HIC) (2.77 in LMIC vs. 1.32 in HIC; p < 0.001, and 0.24% in LMIC vs. 0.01% in HIC; p < 0.001, respectively). ICU admission per 1,000,000 children was 18.80 and 1.48 in HIC and LMIC, respectively (p < 0.001). The highest deaths per 1,000,000 children and CFR were in infants <1 year: 10.03 and 0.58% in the world; 5.39 and 0.07% in HIC; and 10.98 and 1.30% in LMIC, respectively.
Conclusions: This study highlights that there may be a larger impact of paediatric COVID-19 fatality in low- and middle-income compared to high-income countries.
| Level 1 |
De Souza et al (2020) Clinical manifestations of children with COVID-19: A systematic review[7]
objective: To describe the clinical, laboratory and radiological characteristics of children with COVID-19.
Methods: Medline was searched with no language restrictions from December 1 2019 to April 6 2020. Inclusion criteria were: (a) study participants younger than 18 years old; (b) presented original data from cases of COVID-19 confirmed by RT-PCR; and (c) contained descriptions of clinical manifestations, laboratory tests, or radiological examinations.
Results: A total of 38 studies (1,124 cases) were included. From all of the cases, 1,117 had their severity classified: 14.2% were asymptomatic, 36.3% were mild, 46.0% were moderate, 2.1% were severe, and 1.2% were critical. The most prevalent symptom was fever (47.5%), followed by cough (41.5%), nasal symptoms (11.2%), diarrhea (8.1%), and nausea/vomiting (7.1%). 145 (36.9%) children were diagnosed with pneumonia and 43 (10.9%) upper airway infections were reported. Reduced lymphocyte count was reported in 12.9% of cases. Abnormalities in computed tomography were reported in 63.0% of cases. The most prevalent abnormalities reported were ground-glass opacities, patchy shadows and consolidations. Only one death was reported.
Conclusions: Clinical manifestations of children with COVID-19 differ from adult cases.
| Level 1 |
Tsankov et al (2021) Severe COVID-19 Infection and Paediatric Comorbidities: A Systematic Review and Meta-Analysis[8]
Objective: To investigate the effects of paediatric comorbidities on COVID-19 severity.
Methods: A systematic review and meta-analysis. PubMed, Embase and Medline were searched for studies on paediatric COVID-19 infection published from January 1 to October 5, 2020.
Results: 42 studies containing 275,661 children without comorbidities and 9,353 children with comorbidities were included. Severe COVID-19 was present in 5.1% of children with comorbidities, and in 0.2% without comorbidities. Random-effects analysis revealed a higher risk of severe COVID-19 among children with comorbidities than for healthy children; relative risk ratio 1.79 (95% CI 1.27 – 2.51; I2 = 94%). Children with underlying conditions also had a higher risk of COVID-19-associated mortality; relative risk ratio 2.81 (95% CI 1.31 – 6.02; I2 = 82%). Children with obesity had a relative risk ratio of 2.87 (95% CI 1.16 – 7.07; I2 = 36%). In children with severe COVID-19: 64 were obese; 58 had chronic respiratory disease; 45 had cardiovascular disease; 33 had neurologic disorders; 26 had immune disorders; 19 had metabolic disease; 12 had haematological disorders.
Conclusions: Children with comorbidities have a higher risk of severe COVID-19 and associated mortality than children without underlying disease. Additional studies are required to further evaluate this relationship.
| Level 1 |
Results: 29 studies with 4,300 paediatric patients were included in the meta-analysis. The mean age was 7.04 (95% CI: 5.06-9.08) years old. 18.9% of children were asymptomatic (95% CI: 0.121-0.266), 37.4% (95% CI: 0.280-0.474) had no radiographic abnormalities. A proportion of 0.1% patients were admitted to Intensive Care Units (0, 95% CI: 0.000-0.013) and 4 deaths were reported (0, 95% CI: 0.000-0.000).
| Level 1 |
Data show that children are less severely affected with SARS-CoV-2 than adults; however, there have been a small proportion of children who have been critically unwell. In this systematic review, the authors aimed to identify and describe which underlying comorbidities may be associated with severe SARS-CoV-2 disease and death. A total of 1,726 articles were identified and 28 studies fulfilled the inclusion criteria. The 28 studies included 5,686 participants with confirmed SARS-CoV-2 infection ranging from mild to severe disease. The authors focused on the 108 patients who suffered from severe/critical illness requiring ventilation, which included 17 deaths. Of the 108 children who were ventilated, the medical history was available for 48 patients. 36 of the 48 patients (75%) had documented comorbidities of which 11/48 (23%) had pre-existing cardiac disease. Of the 17 patients who died, the past medical history was reported in 12 cases. Of those, 8/12 (75%) had comorbidities.
Conclusion: Although only a small number of children suffer from COVID-19 disease compared to adults, children with comorbidities ¾ particularly pre-existing cardiac conditions ¾ represent a large proportion of those that became critically unwell.
| Level 1 |
Meena et al (2021) Clinical presentations and outcomes of children with cancer and COVID-19: A systematic review[11]
Information regarding the novel coronavirus disease (COVID-19) in paediatric oncology is limited. The authors conducted a systematic review of the available published literature on children with cancer affected by COVID-19. The last date of the study search was October 20, 2020, and 33 studies comprising 226 children were included for the final analysis. Data were extracted in a predefined data collection form, and the variables were extracted and analyzed. Patients with hematological malignancies were more frequent in number. Males and children on intensive treatment were more frequently affected. Fever was the most common symptom. The disease was asymptomatic/mild in 48% and severe in 9.6%. About 10% of children required intensive care, and about 32% had oxygen requirements. The percentage of children who died due to COVID-19 was 4.9%.
Consolidation, peribronchial cuffing and consolidation with ground glass opacities were common imaging findings. Hydroxychloroquine was the most frequently used drug for COVID-19. The percentage of children who died due to COVID-19 was 4.9%. The severity, morbidity and mortality of COVID-19 in paediatric oncology were more compared to the general paediatric population. This information can help in risk stratification for the management of COVID-19.
| Level 2 |
Leidman et al (2021) COVID-19 Trends Among Persons Aged 0-24 Years – United States, March 1-December 12, 2020[12]
Coronavirus disease 2019 (COVID-19) case and electronic laboratory data reported to the Centers of Disease Control and Prevention (CDC) in the United States were analyzed to describe demographic characteristics, underlying health conditions and clinical outcomes; and trends in laboratory-confirmed COVID-19 incidence and testing volume among children, adolescents and young adults (persons aged 0-24 years). This analysis provides a critical update and expansion of previously published data to include trends after autumn school re-openings, and adds preschool-aged children (0-4 years) and college-aged young adults (18-24 years).
Among children, adolescents and young adults, weekly incidence increased with age and was highest during the final week of the review period among all age groups. Time trends in weekly reported incidence for children and adolescents aged 0-17 years correlated consistently with trends observed among adults since June, with both incidence and positive test results tending to increase since September after summer declines. Reported incidence and positive test results among children aged 0-10 years were consistently lower than those in older age groups. 30,229 (2.5%) children were hospitalized, 1,973 (0.8%) required ICU admission, and 654 (<0.1%) died, compared with 16.6%, 8.6%, and 5.0% among adults aged ≥25 years. Among children, adolescents and young adults, the largest percentage of hospitalizations (4.6%) and ICU admissions (1.8%) occurred among children aged 0–4 years.
| Level 2 |
Ladhani et al (2020) COVID-19 in children: analysis of the first pandemic peak in England[13]
Objectives: To assess disease trends, testing practices, community surveillance, case-fatality and excess deaths in children as compared with adults during the first pandemic peak in England.
Participants: Children with COVID-19 between January and May 2020.
Main outcome measures: Trends in confirmed COVID-19 cases; SARS-CoV-2 positivity rates in children compared with adults; community prevalence of SARS-CoV-2 in children with acute respiratory infection (ARI) compared with adults; case-fatality rate in children with confirmed COVID-19; and excess childhood deaths compared with the previous 5 years.
Results: Children represented 1.1% (1,408/129,704) of SARS-CoV-2 positive cases between 16 January 2020 and 3 May 2020. In total, 540,305 people were tested for SARS-COV-2 and 129,704 (24.0%) were positive. In children aged <16 years, 35,200 tests were performed and 1,408 (4.0%) were positive for SARS-CoV-2, compared with 19.1%-34.9% in adults. Childhood cases increased from mid-March and peaked on 11 April before declining. Among 2,961 individuals presenting with ARI in primary care, 351 were children and 10 (2.8%) were positive, compared with 9.3%-45.5% in adults. 8 children died; 4 deaths were due to COVID-19 (case-fatality rate, 0.3%; 95% CI 0.07% to 0.7%). No evidence of excess mortality in children was reported.
Conclusions: Children accounted for a very small proportion of confirmed cases despite the large numbers of children tested. SARS-CoV-2 positivity was low even in children with ARI. These findings provide evidence against the role of children in infection and transmission of SARS-CoV-2.
| Level 2 |
OBJECTIVE: To describe the characteristics of children with COVID-19 with fatal outcomes in a tertiary referral hospital in Indonesia.
Methods: A cross-sectional study using data collected from the medical records of patients with COVID-19 admitted to Dr. Cipto Mangunkusumo Hospital, Jakarta, Indonesia from March to October 2020.
Results: During the study period, 490 patients were admitted and diagnosed with suspected and probable COVID-19. Of these patients, 50 (10.2%) were confirmed to have COVID-19, and 20 (40%) had a fatal outcome. The fatality rate was higher in patients aged ≥10 years categorized with severe disease on admission, PaO2/FiO2 ratio ≤300 mmHg and chronic underlying diseases. Among the children that died, 8 had underlying chronic kidney disease, 6 had cardiovascular disease and 8 had malignancies. The most common clinical manifestations were generalized symptoms, while acute respiratory distress syndrome (8/20) and septic shock (7/20) were the two most common causes of death. Increased procalcitonin, D-dimer, lactate dehydrogenase and presepsin levels were found in all fatal cases. One patient met the criteria of multisystem inflammatory syndrome in children (MIS-C).
Conclusion: Further studies are needed to improve understanding of the role of SARS-CoV-2 in elaborating the mechanisms leading to death in children with comorbidities.
| Level 2 |
Objective: To compare the clinical characteristics and sources of infection among children and youths with COVID-19 during the 3 waves of outbreaks in Hong Kong in 2020.
Design, setting, and participants: A cross-sectional study involving children and adolescents aged ≤18 years with COVID-19 in the 3 waves of outbreaks from January 23 through December 2, 2020.
Main outcomes and measures: Demographic characteristics, travel and contact histories, lengths of hospital stay and symptoms were captured through a central electronic database. Individuals who were infected without recent international travel were defined as having domestic infections.
Results: Among 397 children and youths with confirmed COVID-19 infection, the mean (SD) age was 9.95 (5.34) years; 220 individuals (55.4%) were male; and 154 individuals (38.8%) were asymptomatic. There were significantly more individuals who were infected without symptoms in the second wave (59 of 118 individuals [50.0%]) and third wave (94 of 265 individuals [35.5%]) than in the first wave (1 of 14 individuals [7.1%]) (p = 0.001). Significantly fewer individuals who were infected in the second and third waves compared with the first wave had fever (first wave: 10 individuals [71.4%]; second wave: 22 individuals [18.5%]; third wave: 98 individuals [37.0%]; p < 0.001) or cough (first wave: 6 individuals [42.9%]; second wave: 15 individuals [12.7%]; third wave: 52 individuals [19.6%]; p = 0.02). Among all individuals, 394 individuals (99.2%) had mild illness; 1 patient developed chilblains; 1 patient developed multisystem inflammatory syndrome in children (MIS-C); and 1 patient developed post-COVID-19 autoimmune hemolytic anemia. In all 3 waves, 204 patients with COVID-19 (51.4%) had domestic infections. Among these individuals, 186 (91.2%) reported having a contact history with another individual with COVID-19, of which most (183 individuals [90.0%]) were family members. In the third wave, 18 individuals with domestic infections had unknown contact histories. 3 schoolmates were confirmed with COVID-19 on the same day and were reported to be close contacts.
| Level 4 |
Talita et al (2021) [Cohort Study] 30-Day Outcomes of Children and Adolescents with COVID-19: An International Experience[16]
A total of 242,158 children or adolescents diagnosed with and 9,769 hospitalized with COVID-19, and 2,084,180 diagnosed with influenza were studied. Comorbidities including neurodevelopmental disorders, heart disease and cancer were more common among children and adolescents hospitalized vs. diagnosed with COVID-19. Hospitalization was observed in 0.3% to 1.3% of the COVID-19 diagnosed cohort, with undetectable (n<5 per database) 30-day fatality. 30-day outcomes including pneumonia and hypoxemia were more frequent in the COVID-19 than in the influenza cohort.
| Level 4 |
Fernandes et al (2021) Severe Acute Respiratory Syndrome Coronavirus 2 Clinical Syndromes and Predictors of Disease Severity in Hospitalized Children and Youth[17]
Objective: To characterize the demographic and clinical features of paediatric SARS-CoV-2 syndromes and identify admission variables predictive of disease severity.
METHODS: A multicenter, retrospective and prospective study of paediatric patients hospitalized with acute SARS-CoV-2 infection or multisystem inflammatory syndrome in children (MIS-C) at 8 sites in New York, New Jersey, and Connecticut.
Results: 281 hospitalized patients with SARS-CoV-2 infection were identified and divided into 3 groups based on clinical features. Overall, 143 (50.89%) had respiratory disease, 69 (24.56%) had MIS-C, and 69 (24.56%) had other manifestations including gastrointestinal illness or fever. Patients with MIS-C were more likely to identify as non-Hispanic Black compared to patients with respiratory disease (35% vs. 18%, p = 0.02). 7 patients (2%) died and 114 (41%) were admitted to the Intensive Care Unit. In multivariable analyses, obesity (OR 3.39, 95% CI 1.26-9.10, p = 0.02) and hypoxia on admission (OR 4.01; 95% CI 1.14-14.15; p = 0.03) were predictive of severe respiratory disease. Lower absolute lymphocyte count (OR 8.33 per unit decrease in 109 cells/L, 95% CI 2.32-33.33, p = 0.001) and greater C-reactive protein (OR 1.06 per unit increase in mg/dL, 95% CI 1.01-1.12, p = 0.017) were predictive of severe MIS-C. Obesity and asthma were the most commonly reported preexisting comorbidities (85/250 [34%] and 40 of 281 [14%], respectively). Nearly all patients (267/281 [95%]) recovered from their illness and were discharged home by the end of the study. In multivariable analyses of the respiratory group: younger age (aOR 1.09 per 1-year decrease, 95% CI 1.02-1.16), obesity (aOR 3.39, 95% CI 1.26-9.10), increasing white blood cell count (aOR 1.11 per unit increase in 109/L, 95% CI 1.03-1.20), hypoxia (aOR 4.01, 95% CI 1.14-14.15) and bilateral infiltrates on chest radiograph (aOR 3.69, 95% CI 1.46-9.32) at admission were independent predictors of severe disease.
| Level 4 |
Graff et al (2021) [Retrospective Cohort Study] Risk Factors for Severe COVID-19 in Children[18]
OBJECTIVE: To describe the epidemiology and identify risk factors for severe COVID-19 disease in children.
Methods: A retrospective cohort study among children with positive SARS-CoV-2 PCR from March to July 2020 at a large children’s hospital in Colorado. Risk factors for severe disease were analyzed as defined by hospital admission, requirement for respiratory support, or requirement for critical care.
Results: Among 454 patients identified with SARS-CoV-2, 191 (42.1%) were females. The median age 11 was years. 55% of all patients identified as Hispanic compared with 29% among all hospital visits in 2019 (p < 0.0001). In multivariable analyses, age 0-3 months or >20 years [adjusted odds ratio (aOR), 7.85; p < 0.0001 and aOR, 5.1; p = 0.03, respectively], preterm birth history (aOR, 3.7; p = 0.03), comorbidities [including immunocompromise (aOR, 3.5; p = 0.004), gastrointestinal condition (aOR, 2.7; p = 0.009), diabetes (aOR, 6.6; p = 0.04), asthma (aOR, 2.2; p = 0.04)], and specific symptoms at presentation were predictors for admission. Age 0-3 months or >20 years, asthma, gastrointestinal conditions and similar symptoms at presentation were also predictors for respiratory support. Elevated C-reactive protein was associated with the need for critical care with median of 17.7 mg/dL (IQR, 5.3-22.9) vs. 1.95 mg/dL (IQR, 0.7-5.5) among patients requiring critical vs. no critical care (OR, 1.2; p = 0.02).
Conclusions: Extremes of age, comorbid conditions, and elevated CRP are predictors of severe disease in children. Findings from this study can inform paediatric providers and public health officials to tailor clinical management, pandemic planning, and resource allocation.
| Level 4 |
Discharge data from 869 medical facilities that contributed inpatient and emergency department encounters to an administrative database capturing 20% of US hospitalizations were used to describe patients 18 years or younger who had an inpatient or emergency department encounter with a primary or secondary COVID-19 discharge diagnosis from March 1 through to October 31, 2020. Among 20,714 paediatric patients with COVID-19, 11,153 (53.8%) were aged 12 to 18 years. Among the 2,430 paediatric patients (11.7%) who were hospitalized with COVID-19, 756 (31.1%) experienced severe COVID-19. 3.65% of all children and adolescents who presented to hospital had severe COVID-19.
| Level 4 |
Ouldali et al (2020) Factors Associated With Severe SARS-CoV-2 Infection[20]
OBJECTIVE: To analyze the clinical spectrum of hospitalized paediatric SARS-CoV-2 infection and predictors of severe disease evolution.
Methods: A national prospective surveillance study of children hospitalized with SARS-CoV-2 infection in France. All children with confirmed SARS-CoV-2 infection in 60 hospitals from February 15 to June 1, 2020 were included in the study. The main outcome measure was the proportion of children with severe disease, defined by haemodynamic or ventilatory support requirement.
Results: 397 hospitalized children with SARS-CoV-2 infection were included in the analysis. The authors identified several clinical patterns ranging from paucisymptomatic children admitted for surveillance to lower respiratory tract infection or multisystem inflammatory syndrome in children (MIS-C). Children <90 days old accounted for 37% of cases (145 of 397), but only 4 (3%) had severe disease. Excluding children with MIS-C (n = 29) and hospitalized for a diagnosis not related to SARS-CoV-2 (n = 62), 23 of 306 (11%) children had severe disease, including 6 deaths. Factors independently associated with severity were age ≥10 years (odds ratio [OR] = 3.4, 95% confidence interval: 1.1-10.3), hypoxemia (OR = 8.9 [2.6-29.7]), C-reactive protein level ≥80 mg/L (OR = 6.6 [1.4-27.5]).
Conclusions: In contrast with preliminary reports, young age was not an independent factor associated with severe SARS-CoV-2 infection, and children <90 days old were at the lowest risk of severe disease evolution. Age ≥10 years was the only demographic factor independently associated with severity (OR = 3.4, 95% CI: 1.1-10.3).
| Level 4 |
Götzinger et al (2020) [Cohort Study] COVID-19 in children and adolescents in Europe: a multinational, multicentre cohort study[21]
OBJECTIVE: To capture key data on children and adolescents with SARS-CoV-2 infection across Europe to inform physicians and healthcare service planning during the ongoing pandemic.
Methods: A multicentre cohort study involving 82 participating healthcare institutions across 25 European countries using the well-established Paediatric Tuberculosis Network European Trials Group research network that mainly comprises paediatric infectious diseases specialists and paediatric pulmonologists. All individuals aged 18 years or younger with confirmed SARS-CoV-2 infection, detected at any anatomical site by RT-PCR between April 1 and April 24, 2020 during the initial peak of the European COVID-19 pandemic were included.
Findings: 582 individuals with PCR-confirmed SARS-CoV-2 infection were included. The median age was 5.0 years (IQR 0.5-12.0) and a sex ratio of 1.15 male to female. 145 (25%) had pre-existing medical conditions. 363 (62%) individuals were admitted to hospital. 48 (8%) individuals required ICU admission, 25 (4%) mechanical ventilation (median duration 7 days, IQR 2-11, range 1-34), 19 (3%) inotropic support, and 1 (<1%) extracorporeal membrane oxygenation. Significant risk factors for requiring ICU admission in multivariable analyses were being younger than 1 month (odds ratio 5.06, 95% CI 1.72-14.87; p=0.0035), male sex (2.12, 1.06-4.21; p=0.033), pre-existing medical conditions (3.27, 1.67-6.42; p=0.0015), and presence of lower respiratory tract infection signs or symptoms at presentation (10.46, 5.16-21.23; p<0.0001). 52% of 48 children admitted to ICU had a known comorbidity with previous chronic pulmonary disease (13%) the most common predictor of ICU admission. The most frequently used drug with antiviral activity was hydroxychloroquine (40 [7%] patients), followed by remdesivir (17 [3%] patients), lopinavir-ritonavir (6 [1%] patients), and oseltamivir (3 [1%] patients). Immunomodulatory medication used included corticosteroids (22 [4%] patients), intravenous immunoglobulin (seven [1%] patients), tocilizumab (four [1%] patients), anakinra (three [1%] patients), and siltuximab (one [<1%] patient). 4 children died (case-fatality rate 0.69%, 95% CI 0.20-1.82); at study end, the remaining 578 were alive and only 25 (4%) were still symptomatic or requiring respiratory support.
Interpretation: COVID-19 is generally a mild disease in children, including infants. However, a small proportion develop severe disease requiring ICU admission and prolonged ventilation, although fatal outcome is rare. These data also reflect the current uncertainties regarding specific treatment options, highlighting that additional data on antiviral and immunomodulatory drugs are urgently needed.
| Level 4 |
Objective: To characterise the clinical features of children and young people admitted to hospital with laboratory confirmed severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection in Britain and explore factors associated with admission to critical care, mortality and development of multisystem inflammatory syndrome in children and adolescents temporarily related to coronavirus disease 2019 (COVID-19) (MIS-C).
Design: A prospective observational cohort study with rapid data gathering and near real-time analysis.
Setting: 260 hospitals in England, Wales and Scotland between 17 January and 3 July 2020, with a minimum follow-up time of two weeks (to 17 July 2020).
Participants: 651 children and young people aged less than 19 years admitted to 138 hospitals and enrolled into the International Severe Acute Respiratory and emergency Infections Consortium (ISARIC) WHO Clinical Characterisation Protocol study with laboratory confirmed SARS-CoV-2.
Main outcome measures: Admission to critical care (high dependency or intensive care), in-hospital mortality, or meeting the WHO preliminary case definition for MIS-C.
Results: Median age was 4.6 (interquartile range 0.3-13.7) years, 35% (225/651) were under 12 months old, and 56% (367/650) were male. 57% (330/576) were White, 12% (67/576) South Asian, and 10% (56/576) Black. 42% (276/651) had at least one recorded comorbidity. A systemic mucocutaneous-enteric cluster of symptoms was identified, which encompassed the symptoms for the WHO MIS-C criteria. 18% (116/632) of children were admitted to critical care. On multivariable analysis, this was associated with age under 1 month (odds ratio 3.21, 95% CI 1.36 to 7.66; p=0.008), age 10-14 years (3.23, 1.55 to 6.99; p=0.002), and Black ethnicity (2.82, 1.41 to 5.57; p=0.003). 6 (1%) of 627 patients died in hospital, all of whom had profound comorbidity. Common comorbidities were neurological (11%; 65/614), haematological/oncological/immunological (combined category as described in supplementary methods: 8%; 48/615), and asthma (7%; 45/615). Data on prematurity ¾ defined as birth before completion of 37 weeks’ gestation ¾ were as usual routinely collected only for children aged under 1 year, and 23% (46/201) were premature. 11% (52/456) met the WHO MIS-C criteria, with the first patient developing symptoms in mid-March. Children meeting MIS-C criteria were older (median age 10.7 (8.3-14.1) vs. 1.6 (0.2-12.9) years; p<0.001) and more likely to be of non-White ethnicity (64% (29/45) vs. 42% (148/355); p=0.004). Children with MIS-C were five times more likely to be admitted to critical care (73% (38/52) vs. 15% (62/404); p<0.001). In addition to the WHO criteria, children with MIS-C were more likely to present with fatigue (51% (24/47) vs. 28% (86/302); p=0.004), headache (34% (16/47) vs. 10% (26/263); p<0.001), myalgia (34% (15/44) vs. 8% (21/270); p<0.001), sore throat (30% (14/47) vs. (12% (34/284); p=0.003), and lymphadenopathy (20% (9/46) vs. 3% (10/318); p<0.001) and to have a platelet count of less than 150 × 109/L (32% (16/50) vs. 11% (38/348); p<0.001) than children who did not have MIS-C. No deaths occurred in the MIS-C group.
Conclusions: Children and young people have less severe acute COVID-19 than adults. A systemic mucocutaneous-enteric symptom cluster was also identified in acute cases that shares features with MIS-C. This study provides additional evidence for refining the WHO MIS-C preliminary case definition. Children meeting the MIS-C criteria have different demographic and clinical features depending on whether they have acute SARS-CoV-2 infection (polymerase chain reaction positive) or are post-acute (antibody positive).
| Level 6 |
Sisk et al (2020) National Trends of Cases of COVID-19 in Children Based on US State Health Department Data[23]
In data reported to the CDC in the United States, on September 10, 2020, children represented 1.7% of total hospitalizations, and ∼2% of paediatric cases resulted in hospitalization. Children made up 0.07% of total deaths, and 0.01% of child cases resulted in death.
‘LONG’ COVID-19
| Level 2 |
Buonsenso et al (2021) [Cross-Sectional Study] Preliminary evidence on long COVID in children[24]
This cross-sectional study included all children ≤18 years diagnosed with microbiologically confirmed COVID-19 in Fondazione Policlinico Universitario A. Gemelli IRCCS, Rome, Italy. Only children with a SARS-CoV-2 infection diagnosed 30 days before the assessment were included.
129 children diagnosed with COVID-19 between March and November 2020 were enrolled (mean age of 11 ± 4.4 years; 62 (48.1%) female). 6 children with severe neurocognitive impairment were excluded. 109 children (84.5%) were interviewed by phone-call, and the remainder during outpatient assessment. During the acute phase of COVID-19 illness, 33 children (25.6%) were asymptomatic, and 96 (74.4%) had symptoms. Overall, 6 (4.7%) children were hospitalized, and 3 (2.3%) needed Paediatric Intensive Care Unit admission. After the initial diagnosis of COVID-19, 3 developed multisystem inflammatory syndrome (2.3%) and 2 myocarditis (1.6%). Patients were assessed on average 162.5 ± 113.7 days after COVID-19 microbiological diagnosis. 41.8% completely recovered; 35.7% had one or two symptoms; and 22.5% had three or more symptoms.
Insomnia (18.6%); respiratory symptoms including pain and chest tightness (14.7%); nasal congestion (12.4%); fatigue (10.8%); muscle (10.1%) and joint (6.9%) pain; and concentration difficulties (10.1%) were the most frequently reported symptoms. These symptoms ¾ described both in children with symptomatic and asymptomatic acute COVID-19 ¾ were particularly frequent in those assessed more than 60 days after the initial diagnosis.
20 out of 30 children (66.6%) assessed between 60 and 120 days after initial COVID-19 had at least one persisting symptom; 13 had one or two symptoms; 7 had three or more symptoms. 35 of 68 children (27.1%) had at least one symptom 120 days or more after diagnosis; 21 had one or two symptoms; 14 had three or more symptoms. 29 out of the 68 children assessed ≥120 days from diagnosis (42.6%) were still distressed by these symptoms.
Conclusion: There is increasing evidence that restrictive measures aimed at limiting the pandemic are having a significant impact on children’s mental health. Childhood is a delicate and fundamental period of life, critical for acquisition of social, behavioral and educational development. Evidence that COVID-19 may also have a long-term impact on children, including those with asymptomatic/paucisymptomatic COVID-19, highlights the need for paediatricians, mental health experts and policymakers to implement measures to reduce the impact of the pandemic on children’s health. Further prospective studies, not only based on surveys but with objective clinical assessment and including healthy controls that never had COVID-19 are needed to better understand the burden of long COVID in children.
| Level 4 |
Pulmonary complications in adults who recovered from SARS-CoV-2 have been reported even in minimally symptomatic patients. In this study, lung ultrasound (LUS) findings and pulmonary function of children who recovered from an asymptomatic or mildly symptomatic SARS-CoV-2 infection were evaluated. Patients younger than 18 years who recovered from SARS-CoV-2 infection at the Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico, Milan, Italy, were prospectively followed up for at least 30 days. All enrolled patients underwent LUS. Airway resistance measured by the interrupter technique test was assessed in subjects aged 4-6 years, whereas forced spirometry and measurement of diffusing capacity of the lungs for carbon monoxide were performed in subjects older than 6 years. To evaluate a possible correlation between pulmonary alterations and immune response to SARS-CoV-2, two semi-quantitative enzyme immune assays were used. 16 out of 23 eligible children were enrolled in the study. The median age of enrolled subjects was 7.5 (0.5-10.5) years, with a male to female ratio of 1.7:1. No subject presented any abnormality on LUS, airway resistance test, forced spirometry, and diffusing capacity of the lungs for carbon monoxide. On the other hand, all subjects presented IgG against SARS-CoV-2. In contrast to adults, the authors did not detect any pulmonary complications in the cohort. These preliminary observations suggest that children with an asymptomatic or mildly symptomatic SARS-CoV-2 infection might be less prone to developing pulmonary complications than adults.
MULTISYSTEM INFLAMMATORY SYNDROME IN CHILDREN (MIS-C)
| Level 1 |
Tang et al (2021) [Systematic Review] Multisystem inflammatory syndrome in children during the coronavirus disease 2019 (COVID-19) pandemic: a systematic review of published case studies[26]
OBJECTIVE: To describe the clinical features, treatment and outcomes of MIS-C.
MethodS: A systematic review of published case studies in PubMed, Web of Science, China Biology Medicine (CBM) and China National Knowledge Infrastructure (CNKI) from inception to June 17, 2020 reporting on MIS-C in children and adolescents in the context of COVID-19. Data on clinical manifestations, imaging findings, treatments and outcomes were combined using STATA version 15.
Results: 24 studies were included, with a total of 270 participants. Most cases were from Europe and the United States, and the terminology for MIS-C in different studies varied. Fever and gastrointestinal symptoms were the most commonly experienced symptoms; shock, rash, conjunctivitis, lip or oral cavity changes, hand and foot anomalies, and lymphadenopathy were also observed. Respiratory symptoms seemed relatively infrequent. 78% to 100% of patients had evidence of SARS-CoV-2 infection, and patients positive for SARS-CoV-2 by serology (86% (95% CI: 78%, 95%)) were more than those by RT-PCR (36% (95% CI: 26%, 46%)). Most patients had one or more increased inflammatory markers including C-reactive protein (CRP), procalcitonin (PCT), erythrocyte sedimentation rate (ESR), ferritin, interleukin-6 (IL-6), and D-dimer, accompanied by neutrophilia and lymphopenia. Impaired cardiac function was seen from elevated biomarkers and abnormal echocardiography. Intravenous immunoglobulin (IVIG), anticoagulants, inotropic agents and glucocorticoids were the main treatments, along with other intensive supportive care. Overall, the outcomes of MIS-C were favourable, and only one death was recorded.
CONCLUSION: Patients with MIS-C present with symptoms more severe than children with COVID-19, with fever and gastrointestinal symptoms as primary manifestations and multisystem involvement, particularly the cardiovascular system. Longer follow-up and further studies on the pathophysiology of MIS-C are urgently needed. In addition, attention should be paid to the quality of case studies to
| Level 1 |
Radia et al (2021) Multi-system inflammatory syndrome in children and adolescents (MIS-C): A systematic review of clinical features and presentation[27]
Multisystem inflammatory syndrome in children (MIS-C) is a new phenomenon reported worldwide with temporal association with COVID-19. The objective of the present systematic review is to evaluate reported cases of MIS-C in children and adolescents. From 1,726 articles, 35 documented studies related to MIS-C cases and identified 783 individual cases of MIS-C between March and June 2020; with 55% being male (n = 435) and a median age of 8.6 years (IQR, 7-10 years; range 3 months-20 years). Patients with MIS-C were noted to have a high frequency of gastrointestinal symptoms (71%) including abdominal pain (34%) and diarrhea (27%). Cough and respiratory distress were reported in 4.5% and 9.6% of cases respectively. Blood parameters showed neutrophilia in 345/418 (83%) of cases and a high C-reactive protein in 587/626 (94%). 362/619 (59%) cases were SARS-CoV-2 infection positive (serology or PCR) however only 41% demonstrated pulmonary changes on chest imaging. Comorbidities were reported in a minority of cases 156/783 (20%), with obesity the most frequent (60/783 (7.7%)). Severity of illness was high with 68% cases requiring Intensive Care Unit admission, 63% requiring inotropic support, 244/783 (28%) cases needing some form of respiratory support (138 mechanically ventilated), and 31 requiring extra-corporeal membrane oxygenation. Treatment strategies included intravenous immunoglobulin (63%) and intravenous steroids (44%). 29 cases received Infliximab, 47 received IL1 (interleukin) receptor antagonist, and 47 received IL6 receptor antagonist. 12/783 (1.5%) children died.
In contrast to acute COVID-19 infection in children, MIS-C appears to be a condition of higher severity with 68% of cases having required critical care support.
| Level 4 |
Abrams et al (2021) [Retrospective Surveillance Study] Factors linked to severe outcomes in multisystem inflammatory syndrome in children (MIS-C) in the USA: a retrospective surveillance study[28]
OBJECTIVE: Multisystem inflammatory syndrome in children (MIS-C) is a newly identified and serious health condition associated with SARS-CoV-2 infection. Clinical manifestations vary widely among patients with MIS-C, and the objective of the present study was to investigate factors associated with severe outcomes.
Methods: A retrospective surveillance study. Patients who met the US Centers for Disease Control and Prevention (CDC) case definition for MIS-C ¾ younger than 21 years; fever; laboratory evidence of inflammation; admitted to hospital; multisystem organ involvement [cardiac, renal, respiratory, haematological, gastrointestinal, dermatological, or neurological]; no alternative plausible diagnosis; and either laboratory confirmation of SARS-CoV-2 infection by RT-PCR, serology or antigen test, or known COVID-19 exposure within 4 weeks before symptom onset ¾ were reported from state and local health departments to the CDC using standard case report forms. Factors assessed for potential links to severe outcomes included pre-existing patient factors ¾ sex, age, race or ethnicity, obesity, and MIS-C symptom onset date before June 1, 2020 ¾ and clinical findings such as signs or symptoms, or laboratory markers. Logistic regression models, adjusted for all pre-existing factors, were used to estimate odds ratios between potential explanatory factors and the following outcomes: Intensive Care Unit (ICU) admission, shock, decreased cardiac function, myocarditis and coronary artery abnormalities.
Findings: 1,080 patients met the CDC case definition for MIS-C and had symptom onset between March 11 and October 10, 2020. ICU admission was more likely in patients aged 6-12 years (adjusted odds ratio 1.9 [95% CI 1.4-2.6]) and patients aged 13-20 years (2.6 [1.8-3.8]), compared with patients aged 0-5 years, and more likely in non-Hispanic Black patients, compared with non-Hispanic White patients (1.6 [1.0-2.4]). ICU admission was more likely for patients with shortness of breath (1.9 [1.2-2.9]), abdominal pain (1.7 [1.2-2.7]), and patients with increased concentrations of C-reactive protein, troponin, ferritin, D-dimer, brain natriuretic peptide (BNP), N-terminal pro B-type BNP, or interleukin-6; or reduced platelet or lymphocyte counts. Similar associations for decreased cardiac function, shock and myocarditis were found. Compared with patients aged 0–5 years, patients aged 6–12 years had higher odds of shock (aOR 1.7 [1.2–2.3]) and decreased cardiac function (1.7 [1.2–2.5]), and patients aged 13–20 years had substantially higher odds of shock (2.5 [1.8–3.7]), decreased cardiac function (2.4 [1.6–3.7]), and myocarditis (2.6 [1.6–4.2]). Obesity was linked to decreased cardiac function (1.4 [1.0–1.9]. Coronary artery abnormalities were more common in male patients (1.5 [1.1-2.1]) than in female patients; and in patients with mucocutaneous lesions (2.2 [1.3-3.5]) or conjunctival injection (2.3 [1.4-3.7]).
Conclusion: Identification of important demographic and clinical characteristics could aid in early recognition and prompt management of severe outcomes for patients with MIS-C.
| Level 4 |
Antúnez-Montes et al (2021) [Cohort Study] COVID-19 and Multisystem Inflammatory Syndrome in Latin American Children: A Multinational Study[29]
OBJECTIVE: To assess COVID-19 and Multisystem Inflammatory Syndrome (MIS-C) in Latin American children in order to appropriately plan and allocate resources to face the pandemic on a local and international level.
Methods: An ambispective multicenter cohort study from 5 Latin American countries. Children 18 years of age or younger with microbiologically confirmed SARS-CoV-2 infection or fulfilling MIS-C definition were included.
Findings: 409 children were included, with a median age of 3.0 years (interquartile range 0.6-9.0). Of these, 95 (23.2%) were diagnosed with MIS-C. 191 (46.7%) children were admitted to hospital and 52 (12.7%) required admission to a Paediatric Intensive Care Unit (PICU). 92 (22.5%) patients required oxygen support: 8 (2%) were started on continuous positive airway pressure and 29 (7%) on mechanical ventilation. 35 (8.5%) patients required inotropic support. The following factors were associated with PICU admission: preexisting medical condition (p < 0.0001), immunodeficiency (p = 0.01), lower respiratory tract infection (p < 0.0001), gastrointestinal symptoms (p = 0.006), radiologic changes suggestive of pneumonia and acute respiratory distress syndrome (p < 0.0001) and low socioeconomic conditions (p = 0.009). Death was associated with age (p < 0.0001) (the median age of the 17 children who died was 1 year), known immune-deficiency or immunosuppressive drugs (p = 0.01), PICU admission (p < 0.0001) and lower socioeconomic status (p = 0.05).
Conclusions: This study shows a generally more severe form of COVID-19 and a high number of MIS-C in Latin American children, compared with studies from China, Europe and North America; and supports current evidence of a more severe disease in Hispanic children or in people of lower socioeconomic level.
| Level 4 |
Background: Paediatric Multisystem Inflammatory Syndrome temporally associated with SARS-CoV-2 (PIMS-TS), first identified in April 2020, shares features of both Kawasaki disease (KD) and toxic shock syndrome (TSS). The surveillance describes the epidemiology and clinical characteristics of PIMS-TS in the United Kingdom and Ireland.
Methods: Public Health England initiated prospective national surveillance of PIMS-TS through the British Paediatric Surveillance Unit. Paediatricians were contacted monthly to report PIMS-TS, KD and TSS cases electronically and complete a detailed clinical questionnaire. Cases with symptom onset between 01 March and 15 June 2020 were included.
Findings: There were 216 cases with features of PIMS-TS alone, 13 with features of both PIMS-TS and KD, 28 with features of PIMS-TS and TSS and 11 with features of PIMS-TS, KD and TSS, with differences in age, ethnicity, clinical presentation and disease severity between the phenotypic groups. There was a strong geographical and temporal association between SARS-CoV-2 infection rates and PIMS-TS cases. Of those tested, 14.8% (39/264) children had a positive SARS-CoV-2 RT-PCR, and 63.6% (75/118) were positive for SARS-CoV-2 antibodies. In total 44·0% (118/268) required intensive care, which was more common in cases with a TSS phenotype. 3 of 5 children with cardiac arrest had TSS phenotype. 3 children (1·1%) died.
CONCLUSION: The strong association between SARS-CoV-2 infection and PIMS-TS emphasises the importance of maintaining low community infection rates to reduce the risk of this rare but severe complication in children and adolescents. Close follow-up will be important to monitor long-term complications in children with PIMS-TS.
| Level 4 |
Lima-Setta et al (2020) [Cohort Study] Multisystem inflammatory syndrome in children (MIS-C) during SARS-CoV-2 pandemic in Brazil: a multicenter, prospective cohort study[31]
Objective: To describe the clinical, laboratory, and radiological characteristics, as well as the outcomes of children with MIS-C.
MethodS: A multicenter, prospective cohort study, conducted in 17 paediatric Intensive Care Units in 5 states in Brazil, from March to July 2020. Patients from 1 month to 19 years who met the MIS-C diagnostic criteria were included consecutively.
Results: 56 patients were included, with the following conditions: Kawasaki-like disease (n = 26); incomplete Kawasaki disease (n = 16); acute cardiac dysfunction (n = 10); toxic shock syndrome (n = 3); and macrophage activation syndrome (n = 1). Median age was 6.2 years (IQR 2.4-10.3); 70% were boys; 59% were non-Whites; 20% had comorbidities; 48% reported a contact with COVID-19 cases; and 55% had a recent SARS-CoV-2 infection confirmed by RT-PCR and/or serology. Gastrointestinal symptoms were present in 71%, shock symptoms in 59%, and severe respiratory symptoms in less than 20%. D-Dimer was increased in 80% and cardiac dysfunction markers in more than 75%. Treatment included immunoglobulin (89%); corticosteroids, antibiotics and enoxaparin in about 50% of individuals; and oseltamivir and antifungal therapy in less than 10%. Only 11% needed invasive mechanical ventilation, with a median duration of 5 days (IQR 5-6.5). The median length of PICU stay was 6 days (IQR 5-11), and one death occurred (1.8%).
Conclusion: Most characteristics of current MIS-C patients were similar to those of other cohorts. The present results may contribute to a broader understanding of SARS-CoV-2 infection in children and its short-term consequences. Long-term multidisciplinary follow-up is needed, since it is not known whether these patients will have chronic cardiac impairment or other sequelae.
| Level 6 |
Feldstein et al (2020) Multisystem Inflammatory Syndrome in US Children and Adolescents[32]
Background: Understanding the epidemiology and clinical course of multisystem inflammatory syndrome in children (MIS-C) and its temporal association with coronavirus disease 2019 (COVID-19) is important, given the clinical and public health implications of the syndrome.
Methods: Targeted surveillance for MIS-C from March 15 to May 20, 2020, in paediatric health centers across the United States. The case definition included 6 criteria: serious illness leading to hospitalization; an age of <21 years; fever that lasted for at least 24 hours; laboratory evidence of inflammation; multisystem organ involvement; and evidence of infection with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) based on reverse-transcriptase polymerase chain reaction (RT-PCR), antibody testing, or exposure to persons with COVID-19 in the past month. Clinicians abstracted the data onto standardized forms.
Results: The authors report on 186 patients with MIS-C in 26 states. The median age was 8.3 years; 115 patients (62%) were male; 135 (73%) had previously been healthy; 131 (70%) were positive for SARS-CoV-2 by RT-PCR or antibody testing; and 164 (88%) were hospitalized after April 16, 2020. Organ-system involvement included the gastrointestinal system in 171 patients (92%), cardiovascular in 149 (80%), hematologic in 142 (76%), mucocutaneous in 137 (74%), and respiratory in 131 (70%). The median duration of hospitalization was 7 days (interquartile range, 4 to 10); 148 patients (80%) received intensive care; 37 (20%) received mechanical ventilation; 90 (48%) received vasoactive support; and 4 (2%) died. Coronary-artery aneurysms (z scores ≥2.5) were documented in 15 patients (8%), and Kawasaki’s disease-like features were documented in 74 (40%). Most patients (171 [92%]) had elevations in at least 4 biomarkers indicating inflammation. The use of immunomodulating therapies was common: intravenous immune globulin was used in 144 (77%), glucocorticoids in 91 (49%), and interleukin-6 or 1RA inhibitors in 38 (20%).
Conclusion: Multisystem inflammatory syndrome in children associated with SARS-CoV-2 led to serious and life-threatening illness in previously healthy children and adolescents.
| Level 6 |
Dufort et al (2020) Multisystem Inflammatory Syndrome in Children in New York State[33]
Background: A multisystem inflammatory syndrome in children (MIS-C) is associated with coronavirus disease 2019. The New York State Department of Health established active, state-wide surveillance to describe hospitalized patients with the syndrome.
Methods: Hospitals in New York State reported cases of Kawasaki’s disease, toxic shock syndrome, myocarditis, and potential MIS-C in hospitalized patients younger than 21 years of age and sent medical records to the Department of Health. The authors carried out descriptive analyses that summarized the clinical presentation, complications and outcomes of patients who met the New York State Department of Health case definition for MIS-C between March 1 and May 10, 2020.
Results: As of May 10, 2020, a total of 191 potential cases were reported. Of 95 patients with confirmed MIS-C (laboratory-confirmed acute or recent SARS-CoV-2 infection) and 4 with suspected MIS-C (met clinical and epidemiologic criteria), 53 (54%) were male; 31 of 78 (40%) were Black, and 31 of 85 (36%) were Hispanic. A total of 31 patients (31%) were 0 to 5 years of age, 42 (42%) were 6 to 12 years of age, and 26 (26%) were 13 to 20 years of age. All presented with subjective fever or chills; 97% had tachycardia; 80% had gastrointestinal symptoms; 60% had rash; 56% had conjunctival injection; and 27% had mucosal changes. Elevated levels of C-reactive protein, D-dimer and troponin were found in 100%, 91% and 71% of the patients, respectively. 62% received vasopressor support; 53% had evidence of myocarditis; 80% were admitted to an Intensive Care Unit; and 2 died. The median length of hospital stay was 6 days.
Conclusions: The emergence of multisystem inflammatory syndrome in children in New York State coincided with widespread SARS-CoV-2 transmission. This hyperinflammatory syndrome with dermatologic, mucocutaneous and gastrointestinal manifestations was associated with cardiac dysfunction.
| Level 6 |
Rafferty et al (2021) [Narrative Review] Multisystem inflammatory syndrome in children (MIS-C) and the coronavirus pandemic: Current knowledge and implications for public health[34]
Although children are largely spared from severe illness, a novel childhood hyperinflammatory syndrome presumed to be associated with and subsequent to SARS-CoV-2 infection has emerged with potentially severe outcomes. Multisystem inflammatory disorder in children (MIS-C) most commonly affects young, school-aged children, and is characterized by persistent fever, systemic hyperinflammation, and multisystem organ dysfunction. The majority of studies identified by the authors reported few to no comorbidities. In a case series of 186 patients, Feldstein et al reported that 73% of MIS-C patients were previously healthy. Among those who did have prior health conditions, the most common comorbidities were being overweight (10%–39%) and having a prior history of asthma (5%–18%). While uncommon and generally treatable, MIS-C presents potentially life-altering medical sequelae, complicated by a dearth of information regarding its etiology, pathophysiology and long-term outcomes.
| Level 6 |
Some clusters of children with a multisystem inflammatory syndrome (MIS-C) associated with SARS-CoV-2 infection have been reported. The authors describe the epidemiological and clinical features of children with MIS-C in Spain. Among the cases reported, 13% of children were asthmatic prior to hospitalization for MIS-C; 61% subsequently developed cardiac complications; and 1 out of 31 children died.
MIS-C is a potentially severe condition that presents in some children after SARS-CoV-2 infection. Until herd immunity or a vaccine are available, physicians should be aware of this severe condition in children during COVID-19 epidemics. More studies are necessary to clarify the physiopathology of this syndrome and its adequate treatment.
TRANSMISSION
| Level 1 |
Methods: A systematic literature review of Medline and Embase and the medRxiv/bioRxiv preprint servers to 11 May 2020 to identify published and unpublished studies on COVID-19 transmission by children.
Results: 47 articles were studied in detail. Children accounted for a small fraction of COVID-19 cases and mostly had social contacts with peers or parents, rather than older people at risk of severe disease. Data on viral loads were scarce, but indicated that children may have lower levels than adults, partly because they often have fewer symptoms. Lower viral loads in children should decrease the risk of transmission. Household transmission studies showed that children were rarely the index case and case studies suggested that children with COVID-19 seldom caused outbreaks. However, it is highly likely that children can transmit the SARS-COV-2 virus, and even asymptomatic children can have viral loads.
| Level 1 |
Xu et al (2020) [Systematic Review] What is the evidence for transmission of COVID-19 by children in schools? A living systematic review[37]
Background: It is of paramount importance to understand the transmission of SARS-CoV-2 in schools, which could support the decision-making about educational facilities closure or re-opening with effective prevention and control measures in place.
Methods: The authors conducted a systematic review and meta-analysis to investigate the extent of SARS-CoV-2 transmission in schools. A risk of bias evaluation of all included studies was performed using the Newcastle-Ottawa Scale (NOS).
Results: 2178 articles were retrieved and 11 studies included. 5 cohort studies reported a combined 22 student and 21 staff index cases that exposed 3345 contacts with 18 transmissions (overall infection attack rate (IAR): 0.08%, 95% confidence interval (CI) = 0.00%-0.86%). IARs for students and school staff were 0.15% (95% CI = 0.00%-0.93%) and 0.70% (95% CI = 0.00%-3.56%), respectively. 6 cross-sectional studies reported 639 SARS-CoV-2 positive cases in 6682 study participants tested. The SARS-CoV-2 positivity rate was estimated to be 8.74% (95% CI = 2.34%-18.53%) among students, compared to 13.68% (95% CI = 1.68%-33.89%) among school staff. Gender differences were not found for secondary infection (OR = 1.44, 95% CI = 0.50-4.14, p = 0.49) and SARS-CoV-2 positivity (OR = 0.90, 95% CI = 0.72-1.13, p = 0.36) in schools. Fever, cough, dyspnea, ageusia, anosmia, rhinitis, sore throat, headache, myalgia, asthenia and diarrhoea were all associated with the detection of SARS-CoV-2 antibodies. Overall, study quality was judged to be poor with risk of performance and attrition bias, limiting confidence in the results.
Conclusions: There is limited high-quality evidence available to quantify the extent of SARS-CoV-2 transmission in schools or to compare it to community transmission. Emerging evidence suggests lower IAR and SARS-CoV-2 positivity rate in students compared to school staff. Future prospective and adequately controlled cohort studies are necessary to confirm findings.
| Level 1 |
Viner et al (2021) [Systematic Review and Meta-Analysis] Susceptibility to SARS-CoV-2 Infection Among Children and Adolescents Compared With Adults: A Systematic Review and Meta-Analysis[38]
Importance: The degree to which children and adolescents are infected by and transmit severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is unclear. The role of children and adolescents in transmission of SARS-CoV-2 is dependent on susceptibility, symptoms, viral load, social contact patterns, and behavior.
Objective: To systematically review the susceptibility to and transmission of SARS-CoV-2 among children and adolescents compared with adults.
Data sources: PubMed and medRxiv were searched from database inception to July 28, 2020, and a total of 13,926 studies were identified, with additional studies identified through hand searching of cited references and professional contacts.
Study selection: Studies that provided data on the prevalence of SARS-CoV-2 in children and adolescents compared with adults (³20 years) derived from contact tracing or population screening were included. Single-household studies were excluded.
Data extraction and synthesis: PRISMA guidelines for abstracting data were followed, which was performed independently by 2 reviewers. Quality was assessed using a critical appraisal checklist for prevalence studies. Random-effects meta-analysis was undertaken.
Main outcomes and measures: Secondary infection rate in contact-tracing studies or prevalence or seroprevalence in population screening studies among children and adolescents compared with adults.
Results: A total of 32 studies comprising 41,640 children and adolescents and 268,945 adults met inclusion criteria, including 18 contact-tracing studies and 14 population screening studies. The pooled odds ratio of being an infected contact in children compared with adults was 0.56 (95% CI, 0.37-0.85), with substantial heterogeneity (I2 = 94.6%). Three school-based contact-tracing studies found minimal transmission from child or teacher index cases. Findings from population screening studies were heterogenous and were not suitable for meta-analysis. Most studies were consistent with lower seroprevalence in children compared with adults, although seroprevalence in adolescents appeared similar to adults.
Conclusions and relevance: In this meta-analysis, there is preliminary evidence that children and adolescents have lower susceptibility to SARS-CoV-2, with an odds ratio of 0.56 for being an infected contact compared with adults. There is weak evidence that children and adolescents play a lesser role than adults in transmission of SARS-CoV-2 at a population level. This study provides no information on the infectivity of children.
| Level 1 |
Spielberger et al (2021) [Systematic Review] Intra-Household and Close-Contact SARS-CoV-2 Transmission Among Children – a Systematic Review[39]
Introduction: Early in the pandemic, children were suspected to act as drivers of the COVID-19 spread in the population, which was based on experiences with influenza virus and other respiratory pathogens. Consequently, closures of schools and kindergartens were implemented in many countries around the world, alongside other non-pharmaceutical interventions for transmission control. Given the grave and multifaceted consequences of contact restriction measures for children, it is crucial to better understand the effect size of these incisive actions for the COVID-19 pandemic. The authors systematically reviewed the current evidence on SARS-CoV-2 transmission to and by children.
Data Sources: PubMed and preprints uploaded on medRxiv.
Study Selection: Original research articles, case reports, brief communications and commentaries were included into the analysis. Each title or abstract was independently reviewed to identify relevant articles. Studies in other languages than English were not included.
Data Extraction: Two reviewers independently reviewed the selected studies. Extracted data included citation of each study, type of healthcare setting, location of the study, characteristics of patient population, and reported outcomes.
Results: Data on transmission of SARS-CoV-2 on or by children is scarce. Several studies show a lower seropositivity of children compared to adults, suggesting a lower susceptibility of especially younger children. Most insight currently comes from household studies which indicate that children are predominantly infected by their household contacts. The contagiousness however, seems to be comparable between children and adults. After conducting the meta-analysis, the authors reported a pooled secondary attack rate for a child index of 13.40% (95%CI 5.7–21.1) compared to 12.32% (95%CI 8.3–16.4) for an adult index. Significant heterogeneity among included studies was reported.
Conclusions: Larger and systematic studies are urgently needed to better understand the age dependent patterns of SARS-CoV-2 transmission and thereby design more effective non-pharmaceutical interventions to reduce disease transmission.
| Level 1 |
Li et al (2020) [Systematic Review and Meta-Analysis] Epidemiological and Clinical Characteristics of COVID-19 in Children: A Systematic Review and Meta-Analysis[40]
This systematic review with meta-analysis aimed to evaluate the epidemiological spectrum and clinical characteristics of children infected with SARS-CoV-2. Relevant international and Chinese public databases were systematically searched to identify all case studies from January 1, 2020 to May 7, 2020. 96 studies involving 7004 cases were included. The mean age of paediatric cases was 6.48 years (95% CI 52.0-77.5), 90% had at least one household contact, and 66% presented with mild to moderate clinical syndromes. The main symptoms were fever (47%, 95% CI 41%-53%) and cough (42%, 95% CI 36%-48%). About 23% of children were asymptomatic, 27% had comorbidity, and 29% had a co-infection. The pooled mean incubation period was 9.57 days (95% CI 7.70-11.44). The shedding of SARS-CoV-2 in the upper respiratory tract lasted 11.43 days, and 75% of patients had virus particles in their stool. A total of 34% of the children had neutropenia and 26% had lymphocytosis. Interferon-alpha (81%) was the most commonly used antiviral drug in the children. The discharge and death rates were 79 and 1%. In conclusion, the transmissibility of paediatric COVID-19 should not be ignored because of the relatively long incubation period, shedding duration, and mild clinical symptoms.
| Level 1 |
Madewell et al (2020) [Systematic Review and Meta-Analysis] Household Transmission of SARS-CoV-2: A Systematic Review and Meta-analysis[41]
Importance: Crowded indoor environments such as households are high-risk settings for the transmission of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).
Objectives: To examine evidence for household transmission of SARS-CoV-2, disaggregated by several covariates, and to compare it with other coronaviruses.
Data source: PubMed, searched through October 19, 2020.
Study selection: All articles with original data for estimating household secondary attack rate were included. Case reports focusing on individual households and studies of close contacts that did not report secondary attack rates for household members were excluded.
Data extraction and synthesis: Meta-analyses were done using a restricted maximum-likelihood estimator model to yield a point estimate and 95% CI for secondary attack rate for each subgroup analyzed, with a random effect for each study. To make comparisons across exposure types, study was treated as a random effect, and exposure type was a fixed moderator. The Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) reporting guideline was followed.
Main outcomes and measures: Secondary attack rate for SARS-CoV-2, disaggregated by covariates ¾ ie household or family contact, index case symptom status, adult or child contacts, contact sex, relationship to index case, adult or child index cases, index case sex, number of contacts in household ¾ and for other coronaviruses.
Results: A total of 54 relevant studies with 77,758 participants reporting household secondary transmission were identified. Estimated household secondary attack rate was 16.6% (95% CI, 14.0%-19.3%), higher than secondary attack rates for SARS-CoV (7.5%; 95% CI, 4.8%-10.7%) and MERS-CoV (4.7%; 95% CI, 0.9%-10.7%). Household secondary attack rates were increased from symptomatic index cases (18.0%; 95% CI, 14.2%-22.1%) than from asymptomatic index cases (0.7%; 95% CI, 0%-4.9%), to adult contacts (28.3%; 95% CI, 20.2%-37.1%) than to child contacts (16.8%; 95% CI, 12.3%-21.7%), to spouses (37.8%; 95% CI, 25.8%-50.5%) than to other family contacts (17.8%; 95% CI, 11.7%-24.8%), and in households with 1 contact (41.5%; 95% CI, 31.7%-51.7%) than in households with 3 or more contacts (22.8%; 95% CI, 13.6%-33.5%).
Conclusions and relevance: The findings of this study suggest that given that individuals with suspected or confirmed infections are being referred to isolate at home, households will continue to be a significant venue for transmission of SARS-CoV-2.
| Level 2 |
Yonker et al (2020) Paediatric Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2): Clinical Presentation, Infectivity, and Immune Responses[42]
Objectives: As schools plan for re-opening, understanding the potential role children play in the coronavirus infectious disease 2019 (COVID-19) pandemic and the factors that drive severe illness in children is critical.
Study design: Children ages 0-22 years with suspected severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection presenting to urgent care clinics or being hospitalized for confirmed or suspected SARS-CoV-2 infection or multisystem inflammatory syndrome in children (MIS-C) at Massachusetts General Hospital were offered enrollment in the Massachusetts General Hospital Paediatric COVID-19 Biorepository. Enrolled children provided nasopharyngeal, oropharyngeal, and/or blood specimens. SARS-CoV-2 viral load, ACE2 RNA levels, and serology for SARS-CoV-2 were quantified.
Results: A total of 192 children (mean age, 10.2 ± 7.0 years) were enrolled. 49 children (26%) were diagnosed with acute SARS-CoV-2 infection; an additional 18 children (9%) met the criteria for MIS-C. Only 25 children (51%) with acute SARS-CoV-2 infection presented with fever; symptoms of SARS-CoV-2 infection, if present, were nonspecific. Nasopharyngeal viral load was highest in children in the first 2 days of symptoms, significantly higher than hospitalized adults with severe disease (p = .002). Age did not impact viral load, but younger children had lower angiotensin-converting enzyme 2 expression (p = .004). Immunoglobulin M (IgM) and Immunoglobulin G (IgG) to the receptor binding domain of the SARS-CoV-2 Spike protein were increased in severe MIS-C (p < .001), with dysregulated humoral responses observed.
Conclusions: This study reveals that children may be a potential source of contagion in the SARS-CoV-2 pandemic despite having milder disease or a lack of symptoms; immune dysregulation is implicated in severe postinfectious MIS-C.
| Level 6 |
Milani et al (2021) Frequency of Children vs. Adults Carrying Severe Acute Respiratory Syndrome Coronavirus 2 Asymptomatically[43]
The authors investigated the frequency of individuals carrying SARS-CoV-2 among children admitted for non-infectious conditions and without any SARS-CoV-2–associated symptoms or signs and compare it with the frequency of individuals carrying SARS-CoV-2 among a similar adult population. Children were found to be less frequently positive than adults (1 in 83 children [1.2%] vs. 12 in 131 adults [9.2%]; p = .02), with an odds ratio of 0.12 (95% CI, 0.02-0.95).
| Level 6 |
Posfay-Barbe et al (2020) COVID-19 in Children and the Dynamics of Infection in Families[44]
Since the onset of coronavirus disease (COVID-19) pandemic, children have been less affected than adults in terms of severity and frequency, accounting for <2% of the cases. In contrast to other viral respiratory infections, children do not seem to be a major vector of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) transmission, with most paediatric cases described inside familial clusters and no documentation of child-to-child or child-to-adult transmission. The aim of the present study was to describe the clinical presentation of the first 40 paediatric cases of COVID-19 in our city and the dynamics of their familial clusters.
Methods: From March 10 to April 10, 2020, all patients <16 years old with SARS-CoV-2 infection were identified by means of the Geneva University Hospital’s surveillance network (Switzerland). The network notifies the institution’s paediatric infectious diseases specialists about results of nasopharyngeal specimens tested for SARS-CoV-2 by reverse-transcription polymerase chain reaction. This study was approved by the Regional Ethics Committee. After informed oral parental consent and its documentation in the medical charts, chart reviews were used to retrieve clinical data, and parents were called for patients and household contacts (HHCs) follow-up. HHCs were considered suspect if they had fever or acute respiratory symptoms, as per the Swiss Federal Office for Public Health’s case definition. Categorical data were compared using the χ2 test, with p values <.05 considered significant. Statistics were performed using SPSS version 23.0.
Results: Among a total of 4310 patients with SARS-CoV-2, 40 were <16 years old (0.9%). One patient for which telephone follow-up was not possible was excluded because of the inability to evaluate clinical evolution and HHC symptoms. The median follow-up of the households was 18 days (interquartile range [IQR]: 14–28).
Clinical Presentation, Diagnosis, and Management: Of note, 29 (74%) patients were previously healthy; the most frequently reported comorbidities were asthma (10%), diabetes (8%), obesity (5%), premature birth (5%), and hypertension (3%). 7 patients (18%) were hospitalized to the ward for a median duration of 3 days (IQR: 2–4); reasons for admission were surveillance for nonhypoxemic viral pneumonia (n= 2), fever without source (n = 2), apparent life-threatening event (n = 1), and sepsis-like event (n = 1); one paucisymptomatic child admitted because both parents had severe COVID-19 (n = 1). No patient required ICU admission or SARS-CoV-2–specific therapies. The others 32 patients were managed as outpatients. All patients had a complete resolution of symptoms by day 7 after diagnosis. In only 8% (3/39) of households did the study child develop symptoms before any other HHC. 85% (75/88) of adult household contacts developed symptoms at some point, compared with 43% (10/23) of paediatric HHCs (P < .001)
| Level 6 |
Siebach et al (2021) COVID-19 in childhood: Transmission, clinical presentation, complications and risk factors[45]
Children less than 18 years of age account for an estimated 2%-5% of reported SARS-CoV-2 cases globally. Lower prevalence of coronavirus disease 2019 (COVID-19) among children, in addition to higher numbers of mild and asymptomatic cases, continues to provide challenges in determining appropriate prevention and treatment courses. The authors summarize the current evidence on the transmission, clinical presentation, complications and risk factors in regard to SARS-CoV-2 in children, and highlight crucial gaps in knowledge going forward. Based on current evidence, children are rarely the primary source of secondary transmission in the household or in child care or school settings, and are more likely to contract the virus from an adult household member. The rate of secondary household transmission to children was significantly lower than to adults (16.8% vs. 28.3%). Higher transmission rates are observed in older children (³10 years) compared with younger children (≤9 years); in one study of 59,000 household contacts, when stratified by age, the infection rate was 18.6% for index cases aged 10-19 years, and 5.3% for index cases aged 5-9 years. While increasing incidence of COVID-19 in neonates raises the suspicion of vertical transmission, it is unlikely that breast milk is a vehicle for transmission from mother to infant. The vast majority of clinical cases of COVID-19 in children are mild, but there are rare cases that have developed complications such as multisystem inflammatory syndrome in children (MIS-C), which often presents with severe cardiac symptoms requiring intensive care. Childhood obesity is associated with a higher risk of infection and a more severe clinical presentation. Although immediate mortality rates among children are low, long-term respiratory, and developmental implications of the disease remain unknown in this young and vulnerable population.
VACCINATION
| Level 2 |
Frenck et al (2021) [Randomzed Controlled Trial] Safety, Immunogenicity, and Efficacy of the BNT162b2 Covid-19 Vaccine in Adolescents[46]
Until very recently, vaccines against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) had not been authorized for emergency use in persons younger than 16 years of age. Safe, effective vaccines are needed to protect this population, facilitate in-person learning and socialization, and contribute to herd immunity.
Methods: In an ongoing multinational, placebo-controlled, observer-blinded trial, the authors randomly assigned participants in a 1:1 ratio to receive two injections, 21 days apart, of 30 ug of BNT162b2 or placebo. Noninferiority of the immune response to BNT162b2 in 12 to 15 year-old participants was an immunogenicity objective. Safety (reactogenicity and adverse events) and efficacy against confirmed coronavirus disease 2019 (COVID-19; onset, >7 days after dose 2) in the 12- to 15-year-old cohort were assessed.
Conclusion: No vaccine-related severe adverse events were observed. The geometric mean ratio of SARS-CoV-2 50% neutralizing titers after dose 2 in 12- to 15-year-old participants relative to 16- to 25-year-old participants was 1.76 (95% CI, 1.47 to 2.10).
| Level 5 |
Snapiri et al (2021) [Case Series] Transient Cardiac Injury in Adolescents Receiving the BNT162b2 mRNA COVID-19 Vaccine[47]
Objective: BNT162b2 [Pfizer-BioNTech] is approved for the vaccination of adolescents over 16 years of age in Israel. In clinical trials, systemic adverse events were scarce ¾ although the pre-tested cohort of the adolescent age group was relatively small. The objective of the current study is to raise awareness for potential adverse reactions.
Methods: A case series of patients diagnosed with perimyocarditis following vaccination. Patients were compiled from 3 paediatric medical centers in Israel and data regarding cases were collected. Incidence of perimyocarditis during the vaccination period was also compared with previous years.
Results: All patients were males 16-18 years old, of Jewish descent, who presented with chest pain that began 1-3 days following vaccination. In 6 of the 7 patients, symptoms began following the second vaccine dose and in 1 patient following the first vaccine dose.
Conclusion: All cases were mild and none required cardiovascular or respiratory support. The incidence of perimyocarditis during the vaccination period was elevated in comparison to previous years.
| Level 6 |
Marshall et al (2021) Symptomatic Acute Myocarditis in Seven Adolescents Following Pfizer-BioNTech COVID-19 Vaccination[48]
Reports from 7 cases of acute myocarditis or myopericarditis among adolescent males who developed chest pain within 4 days of receiving the Pfizer-BioNTech vaccine and were hospitalized found that 6 of 7 patients had negative SARS-CoV-2 nucleocapsid antibody assays, and all patients’ symptoms resolved rapidly. 3 patients were treated with non-steroid anti-inflammatory drugs and 4 received intravenous immune globulin and corticosteroids. Diagnostic evaluations for other myocarditis etiologies, including respiratory pathogens from nasopharyngeal swabs, and diagnostics for other infectious agents, were all negative.
| Level 8: UNCLASSIFIED |
The Pfizer-BioNTech covid-19 vaccine has shown 100% efficacy against SARS-CoV-2 in 12 to 15 year olds in the preliminary results of a phase 3 trial.
Pfizer announced the results in a press release: “We plan to submit these data to the FDA as a proposed amendment to our emergency use authorisation in the coming weeks and to other regulators around the world, with the hope of starting to vaccinate this age group before the start of the next school year.”
The phase 3 trial included 2260 children in the United States. A total of 18 cases of COVID-19 were observed in the placebo group (n=1129), and none in the vaccinated group (n=1131).
Other Sources of Evidence
Table 3 – Total number of COVID-19 cases by age group, entire pandemic (to 13 January 2021)
| Age Group | Total Population | Cases Wave 1 | Cases Wave 3 | Increase in % | Cases per 100,000 by age group Wave 1 | Cases per 100,000 by age group Wave 3 |
| 0-4 | 315,200 | 119 | 3,835 | 3,122 | 38 | 1216 |
| 5-14 | 693,700 | 252 | 9,459 | 3,653 | 36 | 1363 |
| 15-24 | 618,100 | 1,582 | 28,490 | 1,784 | 256 | 4609 |
| 25-34 | 620,000 | 3,707 | 28,259 | 662 | 598 | 4557 |
| 35-44 | 776,900 | 3,919 | 24,613 | 528 | 504 | 3168 |
| 45-54 | 661,600 | 4,111 | 23,236 | 465 | 621 | 3512 |
| 55-64 | 539,700 | 2,958 | 17,838 | 503 | 548 | 3305 |
| 65-74 | 404,100 | 1,661 | 8,789 | 429 | 411 | 2174 |
| 75-84 | 214,900 | 2,136 | 6,235 | 191 | 994 | 2901 |
| 85 | 77,300 | 2,200 | 4,781 | 117 | 2,846 | 6184 |
Source: Department of Health (2021), HPSC (2020). CSO (2019) population estimates. Statistics on COVID-19 Wave 1 measured as of midnight on Friday 8th of May. The number of cases = 22,645. Statistics wave 3 cases include cases reported as of midnight on Wednesday 13th January 2021. The number of cases = 155,575, excluding 40 cases where age was not identified.
Table 3 presents the total number and rate of COVID-19 cases by age group for the entire period of the pandemic up to 11 January 2021. As of 8 May 2020, the greatest number (2,200 cases) of people in the older population infected by COVID-19 were aged >85 years. In comparison, in the Third Wave, by 13 January 2021, the age cohort between 15-24 held the highest number of infections with 28,490 cases, closely followed by the 25-34-year-old cohort, with 28,259 cases.
When expressed as per 100,000 of each age group’s population, the >85 years has the highest rate of confirmed cases COVID-19 in the Third Wave. The second highest case by 100,000 population is concentrated on the 15 to 34 group. Conversely, the rate of confirmed COVID-19 cases was lower for the very young population aged 0-4 and 5-14 years at 38 cases and 36 respectively per 100,000 people. By January 2021, these numbers had increased 335% in each of those age cohorts, again another indication younger people are the most affected people in the Third Wave of COVID-19.
Table 4 – Total number of COVID-19 hospitalizations by age group, Waves 1 and 3 (to 13 January 2021)
| Age Group | Total Population | Cases Hospitalized (n) Wave 1 | Cases Hospitalized (n) Wave 3 | % of diagnosed hospitalized by age group Wave 1 | % of diagnosed hospitalized by age group Wave 3 |
| 0-4 | 315,200 | 18 | 82 | 15.1 | 2.13 |
| 5-14 | 693,700 | 17 | 74 | 6.7 | 0.78 |
| 15-24 | 618,100 | 65 | 298 | 4.1 | 1.04 |
| 25-34 | 620,000 | 179 | 518 | 4.8 | 1.83 |
| 35-44 | 776,900 | 240 | 614 | 6.1 | 2.49 |
| 45-54 | 661,600 | 404 | 924 | 9.8 | 3.97 |
| 55-64 | 539,700 | 436 | 1,085 | 14.7 | 6.08 |
| 65-74 | 404,100 | 524 | 1,409 | 31.5 | 16 |
Source: HPSC (2020, 2021).
Table 4 shows the total number of hospitalizations per age group. Younger people are less likely to be hospitalized. This number suggests the elderly are much more vulnerable to the virus and face high risks of health complications. Comparing the First and Third Waves, it is possible to observe the % of diagnosed hospitalized by age group has declined in all age cohorts, except among those 85+. However, it must be noted that young people do get coronavirus infections requiring hospitalization and may develop severe and lasting symptoms, particularly if they are living with obesity, diabetes or hypertension.
Table 5 -Total number and rate of COVID-19 deaths by age group, Wave 1 and 3 (to 18 January 2021)
| Age Group | Total Population | Total Deaths (n) Wave 1 | Total Deaths (n) Wave 3 | Increase in % | Total deaths per 100,000 of population age group Wave 1 | Total deaths per 100,000 of population age group Wave 3 |
| 0-24 | 1,627,000 | 2 | <5 | 150 | 0 | 0.3 |
| 25-34 | 620,000 | 5 | 7 | 40 | 1 | 1.12 |
| 35-44 | 776,900 | 10 | 14 | 40 | 1 | 1.8 |
| 45-54 | 661,600 | 21 | 45 | 114 | 3 | 6.8 |
| 55-64 | 539,700 | 51 | 117 | 129 | 9 | 21.6 |
| 65-74 | 404,100 | 176 | 397 | 125 | 44 | 98.2 |
| 75-84 | 214,900 | 411 | 896 | 118 | 191 | 416 |
| 85 | 77,300 | 527 | 1,136 | 115 | 682 | 1469 |
Source: HPSC (2020, 2021). CSO (2019) population estimates. Statistics on COVID-19 cases reported as of midnight on Wednesday 18th January 2020. The number of cases = 2,616, excluding 4 cases where age was not identified.
Table 5 compares the total number and rate of COVID-19 deaths by age group. As of 18 January 2021, the highest number of deaths associated to COVID-19 were among people aged >85 years-old, with 1136 deaths, and those aged between 75-84 years, with 896 deaths. These numbers are also associated with the rate of hospitalization, since hospitalization numbers are higher for those over 65 (see Table 3). In comparison, there were far fewer deaths among the younger population aged between 0-24, less than 5 deaths since March 2020. Despite the high number of cases among young adults (see Table 3), this group displays a very low number of hospitalization and deaths. The total number of deaths expressed per 100,000 of the population age group again suggests the population over 65 is at a greater risk of death when contracting COVID-19 than other age groups.
Overall, these results make it clear that cases increased by a greater proportion among younger people (15-34) in the Third Wave, but in the same period the mortality rates have increased relatively equally for the majority of age groups, except for the 25-44 cohorts (see Table 4). In addition, the total number of deaths among confirmed cases in the First Wave was 5.78%. In the Third Wave, the mortality rates among confirmed cases decreased threefold to 1.76% (HPSC 2020, 2021). This reduction can be plausibly explained by the spread of the virus among young adults, who face less risks of contracting severe forms of or dying from COVID-19.
Produced by the members of the National Health Library and Knowledge Service Evidence Team†. Current as at 10 May 2021. This evidence summary collates the best available evidence at the time of writing and does not replace clinical judgement or guidance. Emerging literature or subsequent developments in respect of COVID-19 may require amendment to the information or sources listed in the document. Although all reasonable care has been taken in the compilation of content, the National Health Library and Knowledge Service Evidence Team makes no representations or warranties expressed or implied as to the accuracy or suitability of the information or sources listed in the document. This evidence summary is the property of the National Health Library and Knowledge Service and subsequent re-use or distribution in whole or in part should include acknowledgement of the service.
† Julia Reynolds, Librarian, Mayo University Hospital [Author]; Ronan Hegarty, Librarian, Naas General Hospital [Author]; Siobhan McCarthy, Health Intelligence Unit, Strategic Planning and Transformation [Author]; Brendan Leen, Area Library Manager, HSE South [Author, Editor]; NIAC Subgroup Contributors: Dr. Peter O’Reilly; Dr. Philippa White; Dr. Grace Kenny.

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
The following PICO(T) was used as a basis for the evidence summary:
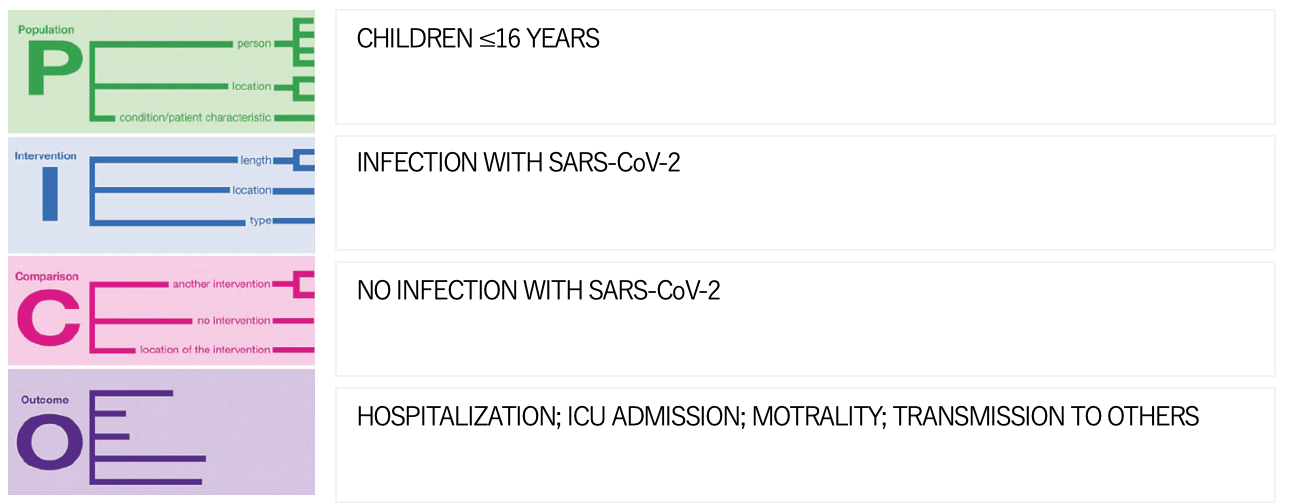
The following search strategy was used:
| 1 exp Coronavirinae/ (50999) 2 COVID-19.ab,ti. (115210) 3 coronavirus.ab,ti. (57105) 4 “corona virus”.ab,ti. (2013) 5 (Wuhan adj3 virus).ab,ti. (113) 6 (“2019-nCoV” or “2019 ncov”).ab,ti. (1263) 7 “severe acute respiratory syndrome coronavirus 2”.ab,ti. (12277) 8 (“2019” and (new or novel) and coronavirus).ab,ti. (9717) 9 1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 (147731) |
The following schema was used to grade the levels of evidence included:
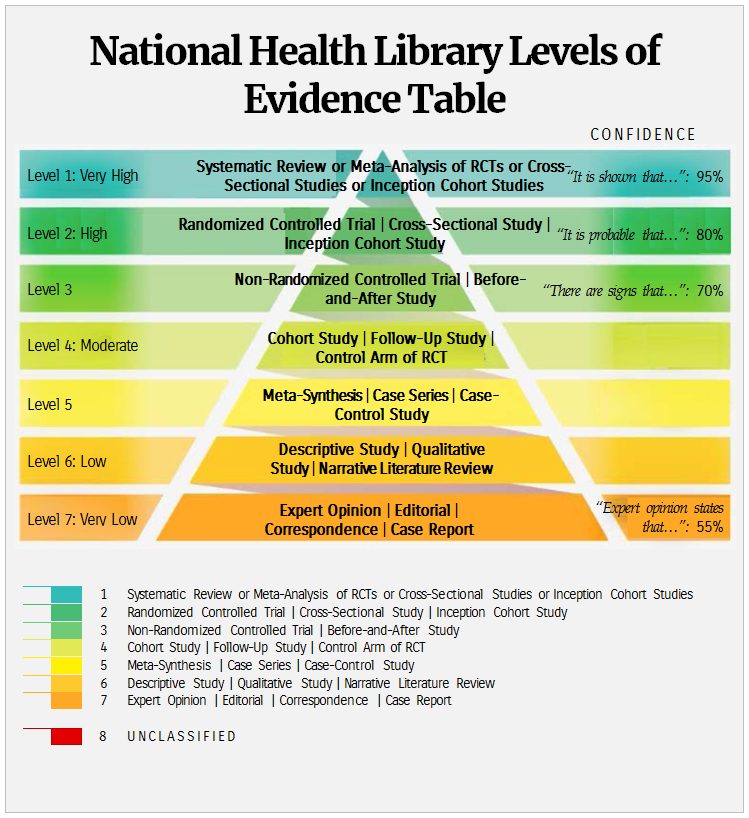
References
[1] World Health Organization (2020) Information for Paediatric Healthcare Providers. https://www.cdc.gov/coronavirus/2019-ncov/hcp/paediatric-hcp.html. Accessed 20 May 2021.
[2]Royal College of Paediatrics and Child Health (Great Britain) (2021) COVID-19 Research Evidence Summaries. https://www.rcpch.ac.uk/resources/COVID-19-research-evidence-summaries. Accessed 20 May 2021.
[3] BMJ Best Practice (2021) Coronavirus Disease 2019 (COVID-19). https://bestpractice.bmj.com/topics/en-us/3000168. Accessed 20 May 2021.
[4]UpToDate (2021) COVID-19: Clinical manifestations and diagnosis in children. https://www.uptodate.com/contents/COVID-19-clinical-manifestations-and-diagnosis-in-children. Accessed 20 May 2021.
[5]UpToDate (2021) COVID-19: Multisystem inflammatory syndrome (MIC-C) in children: clinical features, evaluation, and diagnosis
[6] Kitano T, Kitano M, Krueger C, Jamal H, Al Rawahi H, Lee-Krueger R, Sun RD, Isabel S, García-Ascaso MT, Hibino H, Camara B, Isabel M, Cho L, Groves HE, Piché-Renaud PP, Kossov M, Kou I, Jon I, Blanchard AC, Matsuda N, Mahood Q, Wadhwa A, Bitnun A, Morris SK. The differential impact of paediatric COVID-19 between high-income countries and low- and middle-income countries: A systematic review of fatality and ICU admission in children worldwide. PLoS One. 2021 Jan 29;16(1):e0246326. doi: 10.1371/journal.pone.0246326. PMID: 33513204; PMCID: PMC7845974.
[7] De Souza TH, Nadal JA, Nogueira RJN, Pereira RM, Brandão MB. Clinical manifestations of children with COVID-19: A systematic review. Paediatr Pulmonol. 2020 Aug;55(8):1892-1899. doi: 10.1002/ppul.24885. Epub 2020 Jun 15. PMID: 32492251; PMCID: PMC7300659.
[8] Tsankov BK, Allaire JM, Irvine MA, Lopez AA, Sauvé LJ, Vallance BA, Jacobson K. Severe COVID-19 Infection and Paediatric Comorbidities: A Systematic Review and Meta-Analysis. Int J Infect Dis. 2021 Feb;103:246-256. doi: 10.1016/j.ijid.2020.11.163. Epub 2020 Nov 20. PMID: 33227520; PMCID: PMC7679116.
[9] Liu C, He Y, Liu L, Li F, Shi Y. Children with COVID-19 behaving milder may challenge the public policies: a systematic review and meta-analysis. BMC Paediatr. 2020 Sep 1;20(1):410. doi: 10.1186/s12887-020-02316-1. PMID: 32873269; PMCID: PMC7459157.
[10] Williams N, Radia T, Harman K, Agrawal P, Cook J, Gupta A. COVID-19 Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection in children and adolescents: a systematic review of critically unwell children and the association with underlying comorbidities. Eur J Paediatr. 2021 Mar;180(3):689-697. doi: 10.1007/s00431-020-03801-6. Epub 2020 Sep 10. PMID: 32914200; PMCID: PMC7483054.
[11] Meena JP, Kumar Gupta A, Tanwar P, Ram Jat K, Mohan Pandey R, Seth R. Clinical presentations and outcomes of children with cancer and COVID-19: A systematic review. Paediatr Blood Cancer. 2021 Jun;68(6):e29005. doi: 10.1002/pbc.29005. Epub 2021 Mar 15. PMID: 33719167.
[12] Leidman E, Duca LM, Omura JD, Proia K, Stephens JW, Sauber-Schatz EK. COVID-19 Trends Among Persons Aged 0-24 Years – United States, March 1-December 12, 2020. MMWR Morb Mortal Wkly Rep. 2021 Jan 22;70(3):88-94. doi: 10.15585/mmwr.mm7003e1. PMID: 33476314; PMCID: PMC7821770.
[13] Ladhani SN, Amin-Chowdhury Z, Davies HG, Aiano F, Hayden I, Lacy J, Sinnathamby M, de Lusignan S, Demirjian A, Whittaker H, Andrews N, Zambon M, Hopkins S, Ramsay ME. COVID-19 in children: analysis of the first pandemic peak in England. Arch Dis Child. 2020 Dec;105(12):1180-1185. doi: 10.1136/archdischild-2020-320042. Epub 2020 Aug 12. PMID: 32796006; PMCID: PMC7431771.
[14] Dewi R, Kaswandani N, Karyanti MR, Setyanto DB, Pudjiadi AH, Hendarto A, Djer MM, Prayitno A, Yuniar I, Indawati W, Prawira Y, Handryastuti S, Sjakti HA, Hidayati EL, Muktiarti D, Soebadi A, Puspaningtyas NW, Muhaimin R, Rahmadhany A, Octavius GS, Puspitasari HA, Jasin MR, Tartila T, Putri ND. Mortality in children with positive SARS-CoV-2 polymerase chain reaction test: Lessons learned from a tertiary referral hospital in Indonesia. Int J Infect Dis. 2021 Apr 20;107:78-85. doi: 10.1016/j.ijid.2021.04.019. Epub ahead of print. PMID: 33857609; PMCID: PMC8056472.
[15] Chua GT, Wong JSC, Lam I, Ho PPK, Chan WH, Yau FYS, Rosa Duque JS, Ho ACC, Siu KK, Cheung TWY, Lam DSY, Chan VCM, Lee KP, Tsui KW, Wong TW, Yau MM, Yau TY, Chan KCC, Yu MWL, Chow CK, Chiu WK, Chan KC, Wong WHS, Ho MHK, Tso WWY, Tung KTS, Wong CS, Kwok J, Leung WH, Yam JC, Wong ICK, Tam PKH, Chan GCF, Chow CB, To KKW, Lau YL, Yuen KY, Ip P, Kwan MYW. Clinical Characteristics and Transmission of COVID-19 in Children and Youths During 3 Waves of Outbreaks in Hong Kong. JAMA Netw Open. 2021 May 3;4(5):e218824. doi: 10.1001/jamanetworkopen.2021.8824. PMID: 33938934; PMCID: PMC8094012.
[16] Talita DS, Vizcaya D, Pistillo A, Casajust P, Sena AG, Lai LYH, Prats-Uribe A, Ahmed WU, Alshammari TM, Alghoul H, Alser O, Burn E, You SC, Areia C, Blacketer C, DuVall S, Falconer T, Fernandez-Bertolin S, Fortin S, Golozar A, Gong M, Tan EH, Huser V, Iveli P, Morales DR, Nyberg F, Posada JD, Recalde M, Roel E, Schilling LM, Shah NH, Shah K, Suchard MA, Zhang L, Zhang Y, Williams AE, Reich CG, Hripcsak G, Rijnbeek P, Ryan P, Kostka K, Prieto-Alhambra D. 30-Day Outcomes of Children and Adolescents With COVID-19: An International Experience. Paediatrics. 2021 May 28:e2020042929. doi: 10.1542/peds.2020-042929. Epub ahead of print. PMID: 34049958.
[17] Fernandes DM, Oliveira CR, Guerguis S, Eisenberg R, Choi J, Kim M, Abdelhemid A, Agha R, Agarwal S, Aschner JL, Avner JR, Ballance C, Bock J, Bhavsar SM, Campbell M, Clouser KN, Gesner M, Goldman DL, Hammerschlag MR, Hymes S, Howard A, Jung HJ, Kohlhoff S, Kojaoghlanian T, Lewis R, Nachman S, Naganathan S, Paintsil E, Pall H, Sy S, Wadowski S, Zirinsky E, Cabana MD, Herold BC; Tri-State Paediatric COVID-19 Research Consortium. Severe Acute Respiratory Syndrome Coronavirus 2 Clinical Syndromes and Predictors of Disease Severity in Hospitalized Children and Youth. J Paediatr. 2021 Mar;230:23-31.e10. doi: 10.1016/j.jpeds.2020.11.016. Epub 2020 Nov 14. PMID: 33197493; PMCID: PMC7666535.
[18] Graff K, Smith C, Silveira L, Jung S, Curran-Hays S, Jarjour J, Carpenter L, Pickard K, Mattiucci M, Fresia J, McFarland EJ, Dominguez SR, Abuogi L. Risk Factors for Severe COVID-19 in Children. Paediatr Infect Dis J. 2021 Apr 1;40(4):e137-e145. doi: 10.1097/INF.0000000000003043. PMID: 33538539.
[19] Preston LE, Chevinsky JR, Kompaniyets L, Lavery AM, Kimball A, Boehmer TK, Goodman AB. Characteristics and Disease Severity of US Children and Adolescents Diagnosed With COVID-19. JAMA Netw Open. 2021 Apr 1;4(4):e215298. doi: 10.1001/jamanetworkopen.2021.5298. PMID: 33835179; PMCID: PMC8035649.
[20] Ouldali N, Yang DD, Madhi F, Levy M, Gaschignard J, Craiu I, Guiddir T, Schweitzer C, Wiedemann A, Lorrot M, Romain AS, Garraffo A, Haas H, Rouget S, de Pontual L, Aupiais C, Martinot A, Toubiana J, Dupic L, Minodier P, Passard M, Belot A, Levy C, Béchet S, Jung C, Sarakbi M, Ducrocq S, Danekova N, Jhaouat I, Vignaud O, Garrec N, Caron E, Cohen R, Gajdos V, Angoulvant F; investigator group of the PANDOR study. Factors Associated With Severe SARS-CoV-2 Infection. Paediatrics. 2021 Mar;147(3):e2020023432. doi: 10.1542/peds.2020-023432. Epub 2020 Dec 15. PMID: 33323493.
[21] Götzinger F, Santiago-García B, Noguera-Julián A, Lanaspa M, Lancella L, Calò Carducci FI, Gabrovska N, Velizarova S, Prunk P, Osterman V, Krivec U, Lo Vecchio A, Shingadia D, Soriano-Arandes A, Melendo S, Lanari M, Pierantoni L, Wagner N, L’Huillier AG, Heininger U, Ritz N, Bandi S, Krajcar N, Roglić S, Santos M, Christiaens C, Creuven M, Buonsenso D, Welch SB, Bogyi M, Brinkmann F, Tebruegge M; ptbnet COVID-19 Study Group. COVID-19 in children and adolescents in Europe: a multinational, multicentre cohort study. Lancet Child Adolesc Health. 2020 Sep;4(9):653-661. doi: 10.1016/S2352-4642(20)30177-2. Epub 2020 Jun 25. PMID: 32593339; PMCID: PMC7316447.
[22] Swann OV, Holden KA, Turtle L, Pollock L, Fairfield CJ, Drake TM, Seth S, Egan C, Hardwick HE, Halpin S, Girvan M, Donohue C, Pritchard M, Patel LB, Ladhani S, Sigfrid L, Sinha IP, Olliaro PL, Nguyen-Van-Tam JS, Horby PW, Merson L, Carson G, Dunning J, Openshaw PJM, Baillie JK, Harrison EM, Docherty AB, Semple MG; ISARIC4C Investigators. Clinical characteristics of children and young people admitted to hospital with COVID-19 in United Kingdom: prospective multicentre observational cohort study. BMJ. 2020 Aug 27;370:m3249. doi: 10.1136/bmj.m3249. PMID: 32960186; PMCID: PMC7488201.
[23] Sisk B, Cull W, Harris JM, Rothenburger A, Olson L. National Trends of Cases of COVID-19 in Children Based on US State Health Department Data. Paediatrics. 2020 Dec;146(6):e2020027425. doi: 10.1542/peds.2020-027425. Epub 2020 Sep 29. PMID: 32994175.
[24] Buonsenso D, Munblit D, De Rose C, Sinatti D, Ricchiuto A, Carfi A, Valentini P. Preliminary evidence on long COVID in children. Acta Paediatr. 2021 Apr 9. doi: 10.1111/apa.15870. Epub ahead of print. PMID: 33835507.
[25] Bottino I, Patria MF, Milani GP, Agostoni C, Marchisio P, Lelii M, Alberzoni M, Dell’Era L, Castellazzi ML, Senatore L, Madini B, Pensabene MC, Rocchi A. Can Asymptomatic or Non-Severe SARS-CoV-2 Infection Cause Medium-Term Pulmonary Sequelae in Children? Front Paediatr. 2021 May 13;9:621019. doi: 10.3389/fped.2021.621019. PMID: 34084763; PMCID: PMC8168403.
[26] Tang Y, Li W, Baskota M, Zhou Q, Fu Z, Luo Z, Shi Y, Chen Y, Liu E. Multisystem inflammatory syndrome in children during the coronavirus disease 2019 (COVID-19) pandemic: a systematic review of published case studies. Transl Paediatr. 2021 Jan;10(1):121-135. doi: 10.21037/tp-20-188. PMID: 33633944; PMCID: PMC7882293.
[27] Radia T, Williams N, Agrawal P, Harman K, Weale J, Cook J, Gupta A. Multi-system inflammatory syndrome in children & adolescents (MIS-C): A systematic review of clinical features and presentation. Paediatr Respir Rev. 2021 Jun;38:51-57. doi: 10.1016/j.prrv.2020.08.001. Epub 2020 Aug 11. PMID: 32891582; PMCID: PMC7417920.
[28] Abrams JY, Oster ME, Godfred-Cato SE, Bryant B, Datta SD, Campbell AP, Leung JW, Tsang CA, Pierce TJ, Kennedy JL, Hammett TA, Belay ED. Factors linked to severe outcomes in multisystem inflammatory syndrome in children (MIS-C) in the USA: a retrospective surveillance study. Lancet Child Adolesc Health. 2021 May;5(5):323-331. doi: 10.1016/S2352-4642(21)00050-X. Epub 2021 Mar 10. PMID: 33711293; PMCID: PMC7943393.
[29] Antúnez-Montes OY, Escamilla MI, Figueroa-Uribe AF, Arteaga-Menchaca E, Lavariega-Saráchaga M, Salcedo-Lozada P, Melchior P, de Oliveira RB, Tirado Caballero JC, Redondo HP, Montes Fontalvo LV, Hernandez R, Chavez C, Campos F, Uribe F, Del Aguila O, Rios Aida JA, Buitrago AP, Betancur Londoño LM, Mendoza Vega LF, Hernández CA, Sali M, Higuita Palacio JE, Gomez-Vargas J, Yock-Corrales A, Buonsenso D. COVID-19 and Multisystem Inflammatory Syndrome in Latin American Children: A Multinational Study. Paediatr Infect Dis J. 2021 Jan;40(1):e1-e6. doi: 10.1097/INF.0000000000002949. PMID: 33055501.
[30] Flood J, Shingleton J, Bennett E, Walker B, Amin-Chowdhury Z, Oligbu G, Avis J, Lynn RM, Davis P, Bharucha T, Pain CE, Jyothish D, Whittaker E, Dwarakanathan B, Wood R, Williams C, Swann O, Semple MG, Ramsay ME, Jones CE, Ramanan AV, Gent N, Ladhani SN. Paediatric multisystem inflammatory syndrome temporally associated with SARS-CoV-2 (PIMS-TS): Prospective, national surveillance, United Kingdom and Ireland, 2020. Lancet Reg Health Eur. 2021 Apr;3:100075. doi: 10.1016/j.lanepe.2021.100075. Epub 2021 Mar 22. PMID: 34027512; PMCID: PMC8132575.
[31] Lima-Setta F, Magalhães-Barbosa MC, Rodrigues-Santos G, Figueiredo EADN, Jacques ML, Zeitel RS, Sapolnik R, Borges CTDS, Lanziotti VS, Castro REV, Bellinat APN, Silva TPD, Oliveira FRC, Reis BCSD, Castro NAASR, Macedo JHGC, Scarlato ACCP, Riveiro PM, Mota ICFD, Lorenzo VB, Lucena NML, Azevedo ZMA, Cunha AJLA, Prata-Barbosa A; Brazilian Research Network in Paediatric Intensive Care (BRnet-PIC). Multisystem inflammatory syndrome in children (MIS-C) during SARS-CoV-2 pandemic in Brazil: a multicenter, prospective cohort study. J Paediatr (Rio J). 2021 May-Jun;97(3):354-361. doi: 10.1016/j.jped.2020.10.008. Epub 2020 Nov 9. PMID: 33186512; PMCID: PMC7649656.
[32] Feldstein LR, Rose EB, Horwitz SM, Collins JP, Newhams MM, Son MBF, Newburger JW, Kleinman LC, Heidemann SM, Martin AA, Singh AR, Li S, Tarquinio KM, Jaggi P, Oster ME, Zackai SP, Gillen J, Ratner AJ, Walsh RF, Fitzgerald JC, Keenaghan MA, Alharash H, Doymaz S, Clouser KN, Giuliano JS Jr, Gupta A, Parker RM, Maddux AB, Havalad V, Ramsingh S, Bukulmez H, Bradford TT, Smith LS, Tenforde MW, Carroll CL, Riggs BJ, Gertz SJ, Daube A, Lansell A, Coronado Munoz A, Hobbs CV, Marohn KL, Halasa NB, Patel MM, Randolph AG; Overcoming COVID-19 Investigators; CDC COVID-19 Response Team. Multisystem Inflammatory Syndrome in U.S. Children and Adolescents. N Engl J Med. 2020 Jul 23;383(4):334-346. doi: 10.1056/NEJMoa2021680. Epub 2020 Jun 29. PMID: 32598831; PMCID: PMC7346765.
[33] Dufort EM, Koumans EH, Chow EJ, Rosenthal EM, Muse A, Rowlands J, Barranco MA, Maxted AM, Rosenberg ES, Easton D, Udo T, Kumar J, Pulver W, Smith L, Hutton B, Blog D, Zucker H; New York State and Centers for Disease Control and Prevention Multisystem Inflammatory Syndrome in Children Investigation Team. Multisystem Inflammatory Syndrome in Children in New York State. N Engl J Med. 2020 Jul 23;383(4):347-358. doi: 10.1056/NEJMoa2021756. Epub 2020 Jun 29. PMID: 32598830; PMCID: PMC7346766.
[34] Rafferty MS, Burrows H, Joseph JP, Leveille J, Nihtianova S, Amirian ES. Multisystem inflammatory syndrome in children (MIS-C) and the coronavirus pandemic: Current knowledge and implications for public health. J Infect Public Health. 2021 Apr;14(4):484-494. doi: 10.1016/j.jiph.2021.01.008. Epub 2021 Jan 18. PMID: 33743370; PMCID: PMC7813487.
[35] Moraleda C, Serna-Pascual M, Soriano-Arandes A, Simó S, Epalza C, Santos M, Grasa C, Rodríguez M, Soto B, Gallego N, Ruiz Y, Urretavizcaya-Martínez M, Pareja M, Sanz-Santaeufemia FJ, Fumadó V, Lanaspa M, Jordan I, Prieto L, Belda S, Toral-Vázquez B, Rincón E, Gil-Villanueva N, Méndez-Echevarría A, Castillo-Serrano A, Rivière JG, Soler-Palacín P, Rojo P, Tagarro A; EPICO-AEP Working Group. Multi-inflammatory Syndrome in Children Related to Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) in Spain. Clin Infect Dis. 2021 May 4;72(9):e397-e401. doi: 10.1093/cid/ciaa1042. PMID: 32710613; PMCID: PMC7454331.
[36] Ludvigsson JF. Children are unlikely to be the main drivers of the COVID-19 pandemic – A systematic review. Acta Paediatr. 2020 Aug;109(8):1525-1530. doi: 10.1111/apa.15371. Epub 2020 Jun 17. PMID: 32430964; PMCID: PMC7280674.
[37] Xu W, Li X, Dozier M, He Y, Kirolos A, Lang Z, Mathews C, Siegfried N, Theodoratou E; UNCOVER. What is the evidence for transmission of COVID-19 by children in schools? A living systematic review. J Glob Health. 2020 Dec;10(2):021104. doi: 10.7189/jogh.10.021104. PMID: 33437465; PMCID: PMC7774027.
[38] Viner RM, Mytton OT, Bonell C, Melendez-Torres GJ, Ward J, Hudson L, Waddington C, Thomas J, Russell S, van der Klis F, Koirala A, Ladhani S, Panovska-Griffiths J, Davies NG, Booy R, Eggo RM. Susceptibility to SARS-CoV-2 Infection Among Children and Adolescents Compared With Adults: A Systematic Review and Meta-analysis. JAMA Paediatr. 2021 Feb 1;175(2):143-156. doi: 10.1001/jamapaediatrics.2020.4573. Erratum in: JAMA Paediatr. 2021 Feb 1;175(2):212. PMID: 32975552; PMCID: PMC7519436.
[39] Spielberger BD, Goerne T, Geweniger A, Henneke P, Elling R. Intra-Household and Close-Contact SARS-CoV-2 Transmission Among Children – a Systematic Review. Front Paediatr. 2021 Apr 9;9:613292. doi: 10.3389/fped.2021.613292. PMID: 33898355; PMCID: PMC8062727.
[40] Li B, Zhang S, Zhang R, Chen X, Wang Y, Zhu C. Epidemiological and Clinical Characteristics of COVID-19 in Children: A Systematic Review and Meta-Analysis. Front Paediatr. 2020 Nov 2;8:591132. doi: 10.3389/fped.2020.591132. PMID: 33224909; PMCID: PMC7667131.
[41] Madewell ZJ, Yang Y, Longini IM Jr, Halloran ME, Dean NE. Household Transmission of SARS-CoV-2: A Systematic Review and Meta-analysis. JAMA Netw Open. 2020 Dec 1;3(12):e2031756. doi: 10.1001/jamanetworkopen.2020.31756. PMID: 33315116; PMCID: PMC7737089.
[42] Yonker LM, Neilan AM, Bartsch Y, Patel AB, Regan J, Arya P, Gootkind E, Park G, Hardcastle M, St John A, Appleman L, Chiu ML, Fialkowski A, De la Flor D, Lima R, Bordt EA, Yockey LJ, D’Avino P, Fischinger S, Shui JE, Lerou PH, Bonventre JV, Yu XG, Ryan ET, Bassett IV, Irimia D, Edlow AG, Alter G, Li JZ, Fasano A. Paediatric Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2): Clinical Presentation, Infectivity, and Immune Responses. J Paediatr. 2020 Dec;227:45-52.e5. doi: 10.1016/j.jpeds.2020.08.037. Epub 2020 Aug 20. PMID: 32827525; PMCID: PMC7438214.
[43] Milani GP, Bottino I, Rocchi A, Marchisio P, Elli S, Agostoni C, Costantino G. Frequency of Children vs. Adults Carrying Severe Acute Respiratory Syndrome Coronavirus 2 Asymptomatically. JAMA Paediatr. 2021 Feb 1;175(2):193-194. doi: 10.1001/jamapaediatrics.2020.3595. PMID: 32926119; PMCID: PMC7490740.
[44] Posfay-Barbe KM, Wagner N, Gauthey M, Moussaoui D, Loevy N, Diana A, L’Huillier AG. COVID-19 in Children and the Dynamics of Infection in Families. Paediatrics. 2020 Aug;146(2):e20201576. doi: 10.1542/peds.2020-1576. Epub 2020 May 26. PMID: 32457213.
[45] Siebach MK, Piedimonte G, Ley SH. COVID-19 in childhood: Transmission, clinical presentation, complications and risk factors. Paediatr Pulmonol. 2021 Jun;56(6):1342-1356. doi: 10.1002/ppul.25344. Epub 2021 Mar 15. PMID: 33721405; PMCID: PMC8137603.
[46] Frenck R, Klein N, Kitchin N, Gurtman A, Absalon J, Lockhart S, Perez J, Walter E, Senders S, Bailey R, Swanson K, Ma H, Xu X, Koury K, Kalina W, Cooper D, Jennings T, Brandon D, Thomas S, Tureci O, Tresnan D, Mather S, Dormitzer P, Sahin U, Jansen K, Gruber W, C4591001 Clinical Trial Group. Safety, Immunogenicity, and Efficacy of the BNT162b2 Covid-19 Vaccine in Adolescents. New England Journal of Medicine (NEJM) 2021 May 27: doi: 10.1056/NEJMoa2107456 PMID:34043894.
[47] Snapiri O, Danziger C, Shirman N, Weissbach A, Lowenthal A, Ayalon I, Adam D, Yarden-Bilavsky Y, Bilavsky E. Transient Cardiac Injury in Adolescents Receiving the BNT162b2 mRNA COVID-19 Vaccine. Paediatric Infectious Disease Journal. 2021 June 2; doi: 10.1097/INF.0000000000003235. PMID: 34077949.
[48] Marshall M, Ferguson I, Lewis P, Jaggi P, Gagliardo C, Collins J, Shaughnessya R, Carona R, Fuss C, Corbin K, Emuren L, Faherty E, Hall E, Di Pentima C, Oster M, Paintsil E, Siddiqui S, Timchak D, Guzman-Cottrill J. Symptomatic Acute Myocarditis in Seven Adolescents Following Pfizer-BioNTech COVID-19 Vaccination. Paediatrics. 2021 June 4: doi: 10.1542/peds.2021-052478 PMID: 34088762
[49] Mahase E, COVID-19 Pfizer reports 100% vaccine efficacy in children aged 12 to 15. British Medical Journal (BMJ). 2021 Apr 1;373:n881. doi: 10.1136/bmj.n881. PMID: 33795232.
[50]PublicPolicy.ie (2021) The Pandemic One Year on: Trends and Statistics Between Three Waves of the COVID-19 Pandemic in Ireland. https://publicpolicy.ie/papers/the-pandemic-one-year-on-trends-and-statistics-between-three-waves-of-the-COVID-19-pandemic-in-ireland/.