
Are people who were previously infected with SARS-CoV-2 adequately protected following one dose of a COVID-19 vaccine?
The following information resources have been selected by the National Health Library and Knowledge Service Evidence Virtual Team in response to a question from the National Immunisation Advisory Committee (NIAC). The resources are listed in our estimated order of relevance to practicing healthcare professionals confronted with this scenario in an Irish context. In respect of the evolving global situation and rapidly changing evidence base, it is advised to use hyperlinked sources in this document to ensure that the information you are disseminating to the public or applying in clinical practice is the most current, valid and accurate. For further information on the methodology used in the compilation of this document ⎯ including a complete list of sources consulted please see our National Health Library and Knowledge Service Summary of Evidence Protocol.
Download Full Summary of Evidence (PDF)
Main Points
- The WHO recommends that authorized vaccines should be offered regardless of a person’s history of symptomatic or asymptomatic SARS-CoV-2 infection.
- ≤6 months after initial natural infection, available data show that symptomatic reinfection is uncommon. In the event of limited vaccine supply, persons with PCR-confirmed SARS-CoV-2 infection in the preceding 6 months may choose to delay vaccination until near the end of the 6-month period.
- Several small recently published and preprint studies show that individuals with evidence of prior SARS-CoV-2 infection mount substantially higher antibody responses to the first dose of mRNA vaccines compared with SARS-CoV-2 naive individuals; that antibody response to the first vaccine dose in individuals with pre-existing immunity is greater than or equal to the titers found in naive individuals after the second dose; and that individuals with prior exposure to SARS-CoV-2 demonstrated strong antibody responses to the first dose, but muted responses to the second dose of the vaccine. Among the limitations of these findings are small study size and short follow-up of study participants.
- There is limited evidence that immune response decreases with age.
- Individuals with a history of SARS-CoV-2 may also be more likely to experience local and systemic adverse effects (eg fevers, chills, myalgia and fatigue) after a first vaccine dose than SARS-CoV-2 naive individuals. This is not a contraindication or precaution to a second dose if receiving a vaccine given as two doses.
Summary of Evidence
The World Health Organization (WHO) recommends in respect of the AstraZeneca, Janssen, Moderna and Pfizer-BioNTech coronavirus disease 2019 (COVID-19) vaccines that vaccination should be offered regardless of a person’s history of symptomatic or asymptomatic severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection1 4. Within 6 months after an initial natural infection, available data show that symptomatic reinfection is uncommon. Given limited vaccine supply, persons with polymerase chain reaction (PCR)-confirmed SARS-CoV-2 infection in the preceding 6 months may therefore choose to delay vaccination until near the end of the 6-month period.
The European Centre for Disease Prevention and Control (ECDC) notes that among individuals who have been previously infected with SARS-CoV-2, for currently available vaccines that require a two-dose schedule, a single dose may provide sufficient immunity. The majority of European countries (n=15) currently recommend the full vaccination schedule to those individuals who were previously infected. 7 countries recommend only one dose of vaccine for vaccines that have a two-dose schedule6. Among those 7 countries, the Haute Autorité de Santé in France assert that immunocompetent people with a dated SARS-CoV-2 infection proven by a PCR or antigen test should be considered protected for at least 3 months, and more likely 6 months, by post-infectious immunity; and recommend to carry out their vaccination beyond the period of 3 months after infection, preferably with a period close to 6 months7.
Pre-vaccination viral or serologic testing to identify prior infection is not recommended. For a two-dose vaccine series with the messenger ribonucleic acid (mRNA) COVID-19 vaccines, if SARS-CoV-2 infection is diagnosed following the first vaccine dose, the second dose should still be given9. Individuals with recent, documented SARS-CoV-2 infection, including those who are diagnosed following the first vaccine dose, should have recovered from acute infection and met criteria for discontinuation of isolation precautions before receiving either the initial dose or the second dose of a two-dose series9. The Centers for Diseases Control and Prevention (CDC) and the WHO also recommend that individuals who received monoclonal antibodies or convalescent plasma for COVID-19 should delay vaccination for at least 90 days from the time of treatment. This delay also applies to receipt of the second vaccine dose of a two-dose series if antibody-based COVID-19 therapy was administered after the initial vaccine dose5, 9.
Several recently published and preprint studies suggest that after a single mRNA vaccine dose, individuals with evidence of prior SARS-CoV-2 infection mount substantially higher binding and neutralizing antibody responses compared with SARS-CoV-2 naive individuals9 – 25, 28. Krammer et al. show that the antibody response to the first mRNA vaccine dose in individuals with pre-existing immunity is equal to or even exceeds the titers found in naive individuals after the second dose10, 24; and that reactogenicity after the first vaccine dose is significantly higher in individuals who have been infected with SARS-CoV-2 in the past10. Angyal et al. report that Spike-specific T-cell response was 6-fold higher in previously infected individuals than in SARS-CoV-2 naive individuals at a median of 28 days after the first Pfizer–BioNTech mRNA vaccine dose (median 340 versus [vs.] 58 spot forming units [SFU]/106 peripheral blood mononuclear cells [PBMC], p<0.0001); that T-cell response in previously infected individuals after one Pfizer–BioNTech mRNA vaccine dose was equivalent to naive individuals receiving two Pfizer–BioNTech mRNA vaccine doses (median 158 vs. 165 SFU/106 PBMCs, p=0.65); and that anti-sSpike IgG levels following a single Pfizer–BioNTech mRNA dose in those previously infected were 6.8-fold higher compared with naive individuals following one dose (median 512.9 vs. 75.0 antibody units/ml [AU/ml], p<0.0001) and 2.9-fold higher than naive individuals given two doses 3 weeks apart (179.9 AU/ml, p=0.03)12. Callegaro et al. report that after a single Pfizer–BioNTech mRNA vaccine dose, the median titer of specific antibodies in previously infected individuals was 30,527 U/ml (interquartile range [IQR] 19,992-39,288) and 19,367.5 U/ml (IQR 14,688-31,353) in individuals with previous SARS-CoV-2 asymptomatic infection (p=0.032). Both results were far above the median titer in naive individuals after two Pfizer–BioNTech mRNA vaccine doses: 1,974.5 U/ml (IQR 895-3,455) (p<0.0001).14 Ebinger et al. report that anti-Spike IgG antibody response following a single Pfizer–BioNTech mRNA vaccine dose in persons who had recovered from confirmed prior COVID-19 infection was similar to the antibody response following two doses of vaccine in persons without prior infection16, 17. Gobbi et al. report that in previously infected individuals, neutralizing antibody titers 7 days after the first Pfizer–BioNTech mRNA vaccine dose were not significantly different from those observed in naive subjects 7 days after the second Pfizer–BioNTech mRNA vaccine dose; and suggest that, in previously infected people, a single dose of the vaccine might be sufficient to induce an effective response.18
Samanovic et al. report that in individuals naive to SARS-CoV-2, robust increases in humoral and antigen-specific antibody-secreting cell (ASC) responses following each dose of Pfizer–BioNTech mRNA vaccine have been observed; however, individuals with prior exposure to SARS-CoV-2 demonstrated strong humoral and antigen-specific ASC responses to the first Pfizer–BioNTech mRNA vaccine dose, but muted responses 6-9 days and one month after the second dose of the vaccine23. Goel et al. report that SARS-CoV-2 naive individuals benefitted from both doses of mRNA vaccine, with additional increases in antibodies and memory B cells following booster immunization. In contrast, SARS-CoV-2 recovered individuals had a significant immune response after the first dose with no increase in circulating antibodies or antigen-specific memory B cells after the second dose.19 Tré-Hardy et al. report that antibody levels of seropositive individuals were boosted by the first Moderna mRNA vaccine dose, but no additional boosting effect was observed two weeks after the second dose; and that anti-Spike antibody titers in seronegative individuals obtained two weeks after a single Moderna mRNA vaccine dose were comparable to those obtained in unvaccinated seropositive participants, while the second dose was necessary to achieve higher antibody levels, approaching those obtained for seropositive individuals two weeks after the first dose of the vaccine.24
Individuals with a history of SARS-CoV-2 may also be more likely to experience local and systemic adverse effects (eg fevers, chills, myalgia, and fatigue) after a first vaccine dose than SARS-CoV-2 naive individuals. This is not a contraindication or precaution to a second dose if receiving a vaccine given as two doses9.
Irish and/or International Guidance
| Level 1 |
World Health Organization (2021) Interim recommendations for use of the ChAdOx1-S [AstraZeneca] vaccine against COVID-19[1]
Vaccination should be offered regardless of a person’s history of symptomatic or asymptomatic SARS-CoV-2 infection. Data from clinical trials did not reveal any safety signals. Viral or serological testing for prior infection is not recommended for the purpose of decision-making about vaccination. Within 6 months after an initial natural infection, available data show that symptomatic reinfection is uncommon. Given limited vaccine supply, persons with PCR-confirmed SARS-CoV-2 infection in the preceding 6 months may therefore choose to delay vaccination until near the end of the 6-month period. However, emerging data indicate that symptomatic reinfection after natural infection may occur in settings where variants of concern with evidence of immune escape are circulating. In these settings, earlier immunization after infection may be advisable.
| Level 1 |
World Health Organization (2021) Interim recommendations for the use of the Janssen Ad26.COV2.S (COVID-19) vaccine[2]
Vaccination should be offered regardless of a person’s history of symptomatic or asymptomatic SARS-CoV-2 infection. Viral or serological testing for prior infection is not recommended for the purpose of decision-making about vaccination. Data from the pooled analyses indicate that Ad26.COV2.S is safe in people with evidence of prior SARS-CoV-2 infection. Within 6 months after an initial natural infection, available data show that symptomatic reinfection is uncommon. Given limited vaccine supply, persons with PCR-confirmed SARS-CoV-2 infection in the preceding 6 months may therefore delay vaccination until near the end of the 6-month period. However, emerging data indicate that symptomatic reinfection may occur in settings where variants of concern with evidence of immune escape are circulating. In these settings earlier immunisation after infection may be advisable.
| Level 1 |
World Health Organization (2021) Interim recommendations for use of the Moderna mRNA-1273 vaccine against COVID-19[3]
Vaccination may be offered regardless of a person’s history of symptomatic or asymptomatic SARS-CoV-2 infection. Viral or serological testing for prior infection is not recommended for the purpose of decision-making about vaccination. Available data from the phase 3 trials indicate that mRNA-1273 is safe in people with evidence of prior SARS-CoV-2 infection. Despite the potential for reinfection, currently available data indicate that symptomatic reinfection within 6 months after an initial infection is rare. Persons with PCR-confirmed SARS-CoV-2 infection in the preceding 6 months thus may choose to delay vaccination until near the end of the 6-month period.
| Level 1 |
World Health Organization (2021) Interim recommendations for use of the Pfizer–BioNTech COVID-19 vaccine, BNT162b2, under Emergency Use Listing[4]
Vaccination may be offered regardless of a person’s history of symptomatic or asymptomatic SARS-CoV-2 infection. Viral or serological testing for prior infection is not recommended for the purpose of decision-making about vaccination. Available data from the phase 2/3 trials indicate that BNT162b2 is safe in people with evidence of prior SARS-CoV-2 infection. Despite the potential for reinfection, currently available data indicate that symptomatic reinfection within 6 months after an initial infection is rare. Persons with PCR-confirmed SARS-CoV-2 infection in the preceding 6 months thus may delay vaccination until near the end of the 6-month period.
| Level 1 |
Centers for Disease Control and Prevention (United States) (March 2021) Interim Clinical Considerations for Use of COVID-19 Vaccines Currently Authorized in the United States[5]
See Section: COVID-19 VACCINATION and SARS-CoV-2 INFECTION
People should be offered vaccination regardless of their history of symptomatic or asymptomatic SARS-CoV-2 infection. Data from clinical trials indicates that currently authorized COVID-19 vaccines may be given safely to people with evidence of a prior SARS-CoV-2 infection. Viral testing to assess for acute SARS-CoV-2 infection or serologic testing to assess for prior infection is not recommended for the purposes of vaccine decision-making.
Vaccination of people with known current SARS-CoV-2 infection should be deferred until the person has recovered from the acute illness and have met criteria to discontinue isolation. This recommendation applies to people who experience SARS-CoV-2 infection before receiving any vaccine dose and to those who experience SARS-CoV-2 infection after the first dose of an mRNA vaccine but before receipt of the second dose.
| Level 1 |
European Centre for Disease Prevention and Control (2021) Recommendation of COVID-19 vaccination in individuals previously infected with SARS-CoV-2[6]
There is some evidence that among individuals who have been previously infected with SARS-CoV-2, for currently available vaccines that require a two-dose schedule, a single dose may provide sufficient immunity. The majority of countries (n=15) currently recommend the full vaccination schedule to those individuals who were previously infected. 7 countries recommend only one dose of vaccine for vaccines that have a two dose schedule. One country (Iceland) does not recommend vaccination for those previously infected. In Latvia, vaccination is not recommended to those previously infected for 90 days after infection while there is a shortage of vaccines in the country. This topic is under discussion in Portugal.
Some countries provided the timing for administering a single dose of vaccine in individuals after previous SARS-CoV-2 infection:
- Austria: one dose after 6 to 8 months following infection for all vaccines currently in use.
- Estonia: one dose from 1 week up to 6 months after recovery.
- Italy: one dose at least 3 months after infection, and preferably within 6 months of documented infection. Not valid for immunocompromised individuals.
- Slovakia: one dose after 3 months following infection for all vaccines available. Decision on choice of vaccine to be made by doctor and patient.
- Spain: one dose after 6 months in people under 55 years previously infected with the recommended vaccine according to each population group.
- Norway: one dose 3 months after recovery for all vaccines currently in use. Laboratory test required to confirm infection. Norway has a national registry for all positive laboratory tests.
Table: Recommendations for COVID-19 vaccinations in individuals previously infected with SARS-CoV-2 (n=24)

| Level 1 |
Haute Autorité de Santé (France) (2021) SARS-CoV-2 vaccination strategy – vaccination of people with a history of COVID-19[7]
Immunocompetent people with a dated SARS-CoV-2 infection — symptomatic or not — proven by PCR or antigen test should be considered protected for at least 3 months, and more likely 6 months, against infection with SARS-CoV-2 by post-infectious immunity. It is therefore recommended to carry out their vaccination beyond the period of 3 months after infection, preferably with a period close to 6 months. It seems reasonable that priority should be given to people at risk of severe disease, as defined in the vaccination strategy developed by the Haute Autorité de Santé.
In the event of prolonged symptoms after COVID-19, an appropriate medical consultation is necessary before the vaccination to judge the benefit of the vaccination on a case-by-case basis.
Pre-vaccination serologic testing is not relevant and therefore not recommended; however, in the event of positive serology performed previously, without the infection being dated, the period of 3 months to 6 months begins on the date of the serology.
At this stage of knowledge, the immune response to vaccination of people who have already been infected is of the anamnestic type, which leads to only offering a single dose to immunocompetent people who have had an infection with SARS-CoV-2 because they have already developed an immune memory during the infection. The single dose of vaccine will thus act as a booster. If the second dose of vaccine has already been administered to people with a history of infection with SARS-CoV-2, the data available to date do not show any difference in the safety profile, apart from the occurrence of reactogenicity effects.
People with proven immunosuppression (especially receiving immunosuppressive therapy) should, within 3 months of the onset of SARS-CoV-2 infection, be vaccinated by the two-dose schedule. In situations of prolonged infection, specialist advice is required for vaccination.
People with a PCR-positive SARS-CoV-2 infection after the first dose of vaccine and who have not yet received the second dose should not receive this second dose within the usual timeframe, but within 6 months and not until 3 months after infection.
Haute Autorité de Santé emphasizes that these recommendations reflect the analysis of the literature on 10 February 2021. They may therefore be updated according to the evolution of knowledge on SARS-CoV-2 infection, in particular in view of the data on the immunological response to vaccination of persons previously infected with SARS-CoV-2 and knowledge of the variants.
| Level 1 |
Federal Office of Public Health (Switzerland) Coronavirus: Frequently Asked Questions (FAQs)[8]
Should I have the vaccination even if I’ve already been infected with the new coronavirus? Yes. The vaccination is also recommended if you have already been infected with the new coronavirus. The vaccination gives an additional boost to the immune system so that you are optimally protected.
Data suggest that you are protected from renewed infection for at least 6 months. Therefore, the Federal Office of Public Health (Switzerland) recommends that you have the vaccination starting 6 months after a confirmed coronavirus infection (PCR or rapid antigen test). If it is more than 6 months since you were infected, you should have the vaccination as soon as possible. Here, one dose of vaccine is sufficient; you do not have to have a second dose.
If you’re unclear about when to get vaccinated, please ask your doctor.
There are exceptions for especially vulnerable people. For more information, please consult your doctor.
It is not recommended to have an antibody test before a vaccination, because an antibody test gives no indication of when the infection took place, or whether and for how long you are protected.
Evidence Synopsis Resources
| Level 2 |
UpToDate (2021) COVID-19: Vaccines to prevent SARS-CoV-2 infection[9]
See Section: SPECIAL POPULATIONS
History of SARS-CoV-2 infection: Eligible individuals with a history of SARS-CoV-2 infection should still receive one of [the authorized] vaccines; pre-vaccination serologic screening to identify prior infection is not recommended. For two-dose vaccine series with the mRNA COVID-19 vaccines, if SARS-CoV-2 infection is diagnosed following the first vaccine dose, the second dose should still be given.
Individuals with recent, documented SARS-CoV-2 infection including those who are diagnosed following the first vaccine dose should have recovered from acute infection and met criteria for discontinuation of isolation precautions before receiving either the initial dose or the second dose of a two-dose series. It is also reasonable for such individuals to delay any vaccine receipt for a few months after infection to allow others to get vaccinated sooner, as the risk of reinfection appears extremely low in this period. The CDC also suggests that individuals who received monoclonal antibodies or convalescent plasma for COVID-19 should delay vaccination for at least 90 days from the time of treatment. This delay also applies to receipt of the second vaccine dose of a two-dose series if antibody-based COVID-19 therapy was administered after the initial vaccine dose.
Several small studies have suggested that after a single mRNA vaccine dose, individuals with evidence of prior SARS-CoV-2 infection mount substantially higher binding and neutralizing antibody responses compared with SARS-CoV-2 naive individuals. Whether these findings translate into a durable protective response with a single vaccine dose in previously infected individuals is uncertain. Individuals with a history of SARS-CoV-2 may also be more likely to experience local and systemic adverse effects (eg fevers, chills, myalgia and fatigue) after a first vaccine dose than SARS-CoV-2 naive individuals. This is not a contraindication or precaution to a second dose if receiving a vaccine given as two doses.
Irish and/or International Literature
| Level 2 |
Krammer F et al. (Feb 2021) [Cross-Sectional Study – Preprint] Robust sSpike antibody responses and increased reactogenicity in seropositive individuals after a single dose of SARS-CoV-2 mRNA vaccine[10]
Should individuals who have already had a SARS-CoV-2 infection receive one or two shots of the currently authorized mRNA vaccines? The authors show that the antibody response to the first vaccine dose in individuals with pre-existing immunity is equal to or even exceeds the titers found in naive individuals after the second dose; and that reactogenicity is significantly higher in individuals who have been infected with SARS-CoV-2 in the past. The authors propose that changing the policy to give these individuals only one dose of vaccine would not negatively impact their antibody titers, spare them from unnecessary pain and free up many urgently needed vaccine doses.
| Level 4 |
Abu Jabal K et al. (Feb 2021) [Prospective Cohort Study] Impact of age, ethnicity, sex and prior infection status on immunogenicity following a single dose of the BNT162b2 mRNA COVID-19 vaccine: real-world evidence from healthcare workers, Israel, December 2020 to January 2021[11]
The authors describe immunogenicity 21 days after first dose of the vaccine among 514 Israeli healthcare workers by age, ethnicity, sex and prior COVID-19 infection. Immunogenicity was similar by ethnicity and sex but decreased with age. Compared with healthcare workers with no evidence of previous infection, post-vaccination IgG levels among those with previous evidence of infection were much higher (geometric mean concentration 573 vs. 61.5). IgG titres among those with previous evidence of infection were at least one order of magnitude higher than those without, regardless of whether IgG antibodies were detectable before being vaccination. Among individuals with a previously recorded positive PCR test, IgG levels post first dose of vaccine did not vary according to time from a positive test to vaccination (p = 0.165).
Unsurprisingly, vaccinating individuals with evidence of prior COVID-19 infection led to a boost response, achieving IgG titres approximately one order of magnitude higher compared with naive individuals; and was the case in the present cohort regardless of whether SARS-CoV-2 N antibodies were detectable or not immediately before vaccination, and regardless of the time interval between infection and vaccination. Although these results are based on small numbers [17 observations], they provide reassurance that the well documented rapid waning of nucleocapsid IgG antibodies post-acute COVID-19 infection does not necessarily translate to a loss of immunity. The boost response seen among previously infected individuals suggests B-cell-mediated memory immunity is preserved regardless of IgG status. This study confirms recently published evidence suggesting that immune memory persists at least 6 months post infection. One single case in the present cohort who showed a boost-type response almost 10 months after testing positive by PCR suggests that the persistence of immune memory could be even longer. In situations of scarce vaccine availability, it may therefore be possible to assume that most individuals with prior evidence of infection are not prioritized for vaccination, regardless of pre-vaccination IgG levels. Nevertheless, infection does not protect 100% against re-infection and offering vaccination to these individuals may confer additional protection, as major public health agencies recommend. A single dose of vaccine in these individuals seems to boost the response although the optimal timing between infection and vaccination as well as the ensuing duration of protection remain to be determined.
This study only contains a small number of previously infected individuals as the Israeli Ministry of Health guidelines recommended that these individuals are not prioritized for vaccination, and findings should be replicated on a larger scale in order to make policy decisions. As the immunisation programme continues to expand in Israel, previously infected healthcare workers will be offered the vaccine and antibody levels in these individuals will continue to be assessed.
| Level 4 |
Angyal A et al. (March 2021) [Prospective Cohort Study – Preprint] T-Cell and Antibody Responses to First BNT162b2 Vaccine Dose in Previously SARS-CoV-2-Infected and Infection-Naive UK Healthcare Workers: A Multicentre, Prospective, Observational Cohort Study[12]
Background: Following a single dose of BNT162b2 mRNA vaccine, higher antibody titres are observed following prior SARS-CoV-2 infection than in infection-naive individuals, but T-cell responses are less well defined.
Methods: The authors sampled healthcare workers (HCWs) enrolled in the PITCH study before and after BNT162b2 mRNA vaccination and measured sSpike-specific antibody and quantified T-cell responses by IFNγ ELISpot assay and intracellular staining of peripheral blood mononuclear cells (PBMC), comparing SARS-CoV-2 naive individuals to those with prior infection.
Findings: HCWs aged 22 to 71 years received one (n=216) or two (n=21) vaccine doses. After a single dose, the sSpike-specific T-cell response was 6-fold higher in previously infected versus naive individuals (median 340 versus 58 SFU/106 PBMC, p<0.0001; fresh PBMC, n=99). The T-cell response in previously infected individuals after one vaccine dose was equivalent to naive individuals receiving two vaccine doses (median 158 versus 165 SFU/106 PBMCs, p=0.65; cryopreserved PBMC, n=117). Anti-sSpike IgG levels following a single dose in those previously infected (median 512.9 antibody units/ml (AU/ml)) were 6.8-fold higher versus naive individuals following one dose (median 75.0 AU/ml, p<0.0001) and 2.9-fold higher than naive individuals given two doses 3 weeks apart (179.9 AU/ml, p=0.03). Following vaccination, plasma from individuals with prior infection demonstrated higher in vitro neutralization of the B.1.351 variant of concern compared to naive individuals.
Interpretation: Following a single BNT162b2 dose, HCWs with a prior history of SARS-CoV-2 infection have significantly higher T-cell and antibody responses than naive individuals.
| Level 4 |
Bradley T et al. (Feb 2021) [Prospective Cohort Study – Preprint] Antibody responses boosted in seropositive healthcare workers after single dose of SARS-CoV-2 mRNA vaccine[13]
Current guidelines recommend that individuals who have had COVID-19 should receive the identical vaccine regimen as those who have not had the infection. This includes two doses of the mRNA platform vaccines (Pfizer-BioNTech BNT162b2; Moderna mRNA-1273) that are approved for use in the United States. In this brief report, the authors show that after a single dose of the Pfizer-BioNTech SARS-CoV-2 vaccine, individuals that had prior SARS-CoV-2 infection had significantly higher antibody levels than individuals that had no history of infection. This provides the rationale for changing vaccination policy to deliver only a single dose to individuals with recent SARS-CoV-2 infection that may free up additional doses for individuals that have no preexisting immunity to the virus. Future studies of other immune parameters such as T cell response and durability of immune response should be rapidly carried out in individuals infected with SARS-CoV-2 prior to vaccination.
| Level 4 |
Callegaro A et al. (March 2021) [Prospective Cohort Study] Antibody response to SARS-CoV-2 vaccination is extremely vivacious in subjects with previous SARS-CoV-2 infection[14]
Background: In this study the authors verified if in individuals with a previous SARS-CoV-2 infection a single dose of mRNA vaccine would be immunologically equivalent to a full vaccine schedule in naive individuals.
Methods: Healthcare workers (n=184) with a previous SARS-CoV-2 infection were sampled soon before the second dose of vaccine and between 7 and 10 days after the second dose. The last sampling time was also applied to SARS-CoV-2 naive individuals. Antibodies against SARS-CoV-2 were measured using Elecsys® Anti-SARS-CoV-2 S immunoassay. The study was powered for non-inferiority. Non parametric tests and the Pearson correlation coefficient were used to perform inferential analysis.
Results: After a single vaccine injection, the median titer of specific antibodies in individuals with previous COVID-19 was 30,527 U/ml (IQR 19,992-39,288) and in subjects with previous SARS-CoV-2 asymptomatic infection 19,367.5 U/ml (IQR 14,688-31,353) (p=0.032). Both results were far above the median titer in naive individuals after a full vaccination schedule: 1,974.5 U/ml (IQR 895-3,455) (p<0.0001). Adverse events after vaccine injection were more frequent after the second dose of vaccine (mean 0.95, 95%CI from 0.75 to 1.14 versus mean 1.91, 95%CI from 1.63 to 2.19)(p<0.0001) and in exposed compared to naive (mean 1.63; 95%CI from 1.28 to 1.98 versus mean 2.35; 95%CI from 1.87 to 2.82)(p=0.015).
Conclusion: In SARS-CoV-2 naturally infected individuals a single mRNA vaccine dose seems sufficient to reach immunity. Modifying current dosing schedules would speed-up vaccination campaigns.
| Level 4 |
Ciccone EJ et al. (Feb 2021) [Prospective Cohort Study – Preprint] SARS-CoV-2 seropositivity after infection and antibody response to mRNA-based vaccination[15]
The effect of SARS-CoV-2 infection on response to mRNA-based SARS-CoV-2 vaccines is not well-described. The authors assessed longitudinal SARS-CoV-2-specific antibody responses pre- and post-vaccination among individuals with and without prior infection. The antibody response to the first vaccine dose was almost 2-fold higher in individuals who were seropositive before vaccination compared to those who were seronegative, suggesting that prior infection primes the immune response to the first dose of mRNA-based vaccine.
| Level 4 |
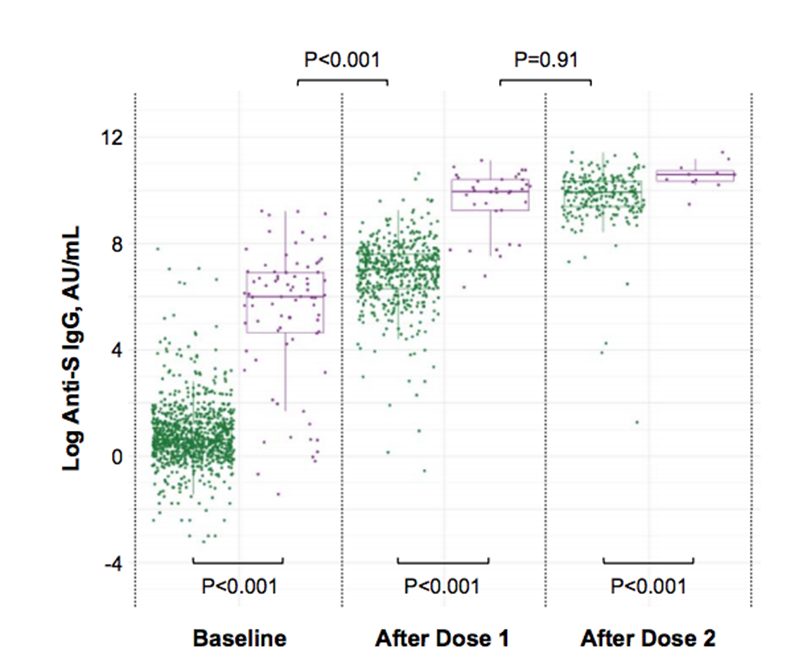
Ebinger JE et al. (Feb 2021) [Prospective Cohort Study] Prior COVID-19 Infection and Antibody Response to Single Versus Double Dose mRNA SARS-CoV-2 Vaccination[16]
With supply chain logistics impacting the rollout of population-scale vaccination programs, increasing attention has turned to the potential efficacy of single versus double dose vaccine administration for select individuals. The authors examined response to Pfizer-BioNTech mRNA vaccine in a large cohort of healthcare workers including those with and without prior COVID-19 infection. For all participants, circulating levels of SARS-CoV-2 anti-sSpike (S) protein IgG at baseline prior to vaccine, after the first vaccine dose and after the second vaccine dose were quantified. The anti-S IgG antibody response following a single vaccine dose in persons who had recovered from confirmed prior COVID-19 infection was similar to the antibody response following two doses of vaccine in persons without prior infection (P≥0.58). Patterns were similar for the post-vaccine symptoms experienced by infection recovered persons following their first dose compared to the symptoms experienced by infection naive persons following their second dose (p=0.66). These results support the premise that a single dose of mRNA vaccine could provoke in COVID-19 recovered individuals a level of immunity that is comparable to that seen in infection naive persons following a double dose regimen. Additional studies are needed to validate our findings, which could allow for public health programs to expand the reach of population-wide vaccination efforts.
Figure: Anti-Spike IgG antibody response to mRNA SARS-CoV-2 vaccination i persons with and without prior COVID-19 infection

| Level 4 |
Ebinger JE et al. (Apr 2021) [Prospective Cohort Study] Antibody responses to the BNT162b2 mRNA vaccine in individuals previously infected with SARS-CoV-2[17]
In a cohort of Pfizer-BioNTech mRNA vaccine recipients (n = 1,090), the authors observed that sSpike-specific IgG antibody levels and ACE2 antibody binding inhibition responses elicited by a single vaccine dose in individuals with prior SARS-CoV-2 infection (n = 35) were similar to those seen after two doses of vaccine in individuals without prior infection (n = 228). Post-vaccine symptoms were more prominent for those with prior infection after the first dose, but symptomology was similar between groups after the second dose.
| Level 4 |
Gobbi F et al. (March 2021) [Prospective Cohort Study] Antibody Response to the BNT162b2 mRNA COVID-19 Vaccine in Subjects with Prior SARS-CoV-2 Infection[18]
Although antibody levels progressively decrease following SARS-CoV-2 infection, immune memory persists for months. Thus, individuals who naturally contracted SARS-CoV-2 are expected to develop a more rapid and sustained response to COVID-19 vaccines than naive individuals. In this study, the authors analyzed the dynamics of the antibody response to the Pfizer-BioNTech BNT162b2 mRNA COVID-19 vaccine in 6 healthcare workers who contracted SARS-CoV-2 in March 2020, in comparison to 9 control subjects without a previous infection. The vaccine was well tolerated by both groups, with no significant difference in the frequency of vaccine-associated side effects, with the exception of local pain, which was more common in previously infected subjects. Overall, the titers of neutralizing antibodies were markedly higher in response to the vaccine than after natural infection. In all subjects with pre-existing immunity, a rapid increase in anti-Spike receptor-binding domain (RBD) IgG antibodies and neutralizing antibody titers was observed one week after the first dose, which seemed to act as a booster. Notably, in previously infected individuals, neutralizing antibody titers 7 days after the first vaccine dose were not significantly different from those observed in naive subjects 7 days after the second vaccine dose. These results suggest that, in previously infected people, a single dose of the vaccine might be sufficient to induce an effective response.
| Level 4 |
Goel RR et al. (March 2021) [Prospective Cohort Study] Longitudinal Analysis Reveals Distinct Antibody and Memory B Cell Responses in SARS-CoV-2 naive and Recovered Individuals Following mRNA Vaccination[19]
Novel mRNA vaccines for SARS-CoV-2 have been authorized for emergency use and are currently being administered to millions of individuals worldwide. Despite their efficacy in clinical trials, there is limited data on vaccine-induced immune responses in individuals with a prior SARS-CoV-2 infection compared to SARS-CoV-2 naive subjects. Moreover, how mRNA vaccines impact the development of antibodies as well as memory B cells in COVID-19 experienced versus COVID-19 naive subjects remains poorly understood. The authors evaluated antibody responses and antigen-specific memory B cell responses over time in 33 SARS-CoV-2 naive and 11 SARS-CoV-2 recovered subjects. mRNA vaccination induced significant antibody and memory B cell responses against full-length SARS-CoV-2 Spike protein and the sSpike receptor binding domain (RBD). SARS-CoV-2 naive individuals benefitted from both doses of mRNA vaccine with additional increases in antibodies and memory B cells following booster immunization. In contrast, SARS-CoV-2 recovered individuals had a significant immune response after the first dose with no increase in circulating antibodies or antigen-specific memory B cells after the second dose. Moreover, the magnitude of the memory B cell response induced by vaccination was lower in older individuals, revealing an age-dependence to mRNA vaccine-induced B cell memory. Side effects also tended to associate with post-boost antibody levels, but not with post-boost memory B cells, suggesting that side effect severity may be a surrogate of short-term antibody responses. The frequency of pre-vaccine antigen-specific memory B cells in SARS-CoV-2 recovered individuals strongly correlated with post-vaccine antibody levels, supporting a key role for memory B cells in humoral recall responses to SARS-CoV-2. This observation may have relevance for future booster vaccines and for responses to viral variants that partially escape pre-existing antibodies and require new humoral responses to be generated from memory B cells. Finally, post-boost antibody levels were not correlated with post-boost memory responses in SARS-CoV-2 naive individuals, indicating that short-term antibody levels and memory B cells are complementary immunological endpoints that should be examined in tandem when evaluating vaccine response. Together, these data provide evidence of both serological response and immunological memory following mRNA vaccination that is distinct based on prior SARS-CoV-2 exposure. These findings may inform vaccine distribution in a resource-limited setting.
| Level 4 |
Levi R et al. (Feb 2021) [Prospective Cohort Study – Preprint]A cautionary note on recall vaccination in ex-COVID-19 subjects[20]
Currently approved mRNA or adenovirus vector COVID-19 vaccines require a first injection followed by recall immunization. There is no indication as to whether individuals who have recovered from COVID-19 should be vaccinated; and, if vaccinated, whether they should receive one or two vaccine doses. The authors tested antibody response developed after the first dose of the Pfizer-BioNTech mRNA-based vaccine in 124 healthcare workers of which 57 had a previous history of COVID-19 (‘ex-COVID’). Post-vaccine antibodies in ex-COVID individuals increase exponentially within 7-15 days after the first dose compared to naive subjects (p<0.0001). The authors developed a multivariate linear regression (LR) model to predict the IgG response for SARS-COV-2 vaccine and found that the antibody response of ex-COVID patients depends on the IgG pre-vaccine titer and on the symptoms developed during the disease, with anosmia/dysgeusia and gastrointestinal disorders being the most significantly positively correlated in the LR. Thus, one vaccine dose is sufficient to induce a good antibody response in ex-COVID subjects.
| Level 4 |
Prendecki M et al. (March 2021) [Prospective Cohort Study] Effect of previous SARS-CoV-2 infection on humoral and T-cell responses to single-dose BNT162b2 vaccine[21]
The authors show that individuals with previous SARS-CoV-2 infection generate strong humoral and cellular responses to one dose of the Pfizer-BioNTech BNT162b2 vaccine, with evidence of high titres of in-vitro live virus neutralization. In contrast, most individuals who are infection-naive generate both weak T-cell responses and low titres of neutralizing antibodies. Existing studies predicting risk of re-infection based on neutralizing antibody titres or longevity of immunological responses are highly heterogeneous. Evidence for the longevity and protective effect of T-cell responses is particularly limited. In particular, peptide pool selection might affect T-cell responses, meaning results cannot be compared between studies. The authors use S1 and S2 peptide pools, rather than peptides spanning the whole sSpike glycoprotein, which might underestimate the true magnitude of T-cell responses. Despite the difficulty of extrapolating immunological data to clinical protection, the study’s findings raise important issues that warrant consideration when determining optimal use of vaccine supplies. Firstly, those with serological evidence of previous disease at baseline mount robust antibody and T-cell responses after a single dose of vaccine. Conversely, some infection-naive individuals mount very little demonstrable response to single-dose vaccination, which might not provide sufficient immunity to protect from clinical disease or viral shedding, and might not persist for a 12-week delay until the second vaccine is administered. One infection-naive individual included in the study developed symptomatic, PCR-proven infection 5 weeks after one dose of vaccine; notably, their anti-S titre post-vaccination was 61·8 AU/mL.
In line with published reports of other vaccines, serological response to BNT162b2 inversely correlates with age. The authors found median anti-S titres post-vaccination in the infection cohort to be lower than those seen 2–8 weeks after natural infection alone, and this difference was particularly striking in those older than 50 years. 2 participants did not seroconvert, and 8 participants generated antibody titres less than 250 AU/mL, which might not be sufficient for any virus neutralization based on correlation of virus neutralization and anti-S titre in the study. All 10 of these individuals were older than 50 years. In a setting where prioritization of groups of healthcare workers for second vaccination might be necessary, consideration must be given to protocolised vaccination of infection-naive individuals or those over the age of 50 who are at increased risk of both severe COVID-19 and minimal vaccine response. These results also highlight the need for continuing rigorous use of personal protective equipment after vaccination to prevent both infection and asymptomatic spread of disease.
| Level 4 |
Saadat S et al. (Feb 2021) [Prospective Cohort Study – Preprint] Single Dose Vaccination in Healthcare Workers Previously Infected with SARS-CoV-2[22]
Coronavirus disease 2019 (COVID-19) vaccine shortages have led some experts and countries to consider untested dosing regimens. The authors studied antibody responses to a single dose of the Pfizer-BioNTech or Moderna vaccines in healthcare workers (HCWs) with laboratory-confirmed COVID-19 infection and compared to them to antibody responses of HCWs who were IgG negative to SARS-CoV-2. HCWs with prior COVID-19 showed clear secondary antibody responses to vaccination with IgG sSpike binding titers rapidly increasing by 7 days and peaking by days 10 and 14 post-vaccination. At all time-points tested, HCWs with prior COVID-19 infection showed statistically significant higher antibody titers of binding and functional antibody compared to HCWs without prior COVID-19 infection (p<.0001 for each of the time-points tested). In times of vaccine shortage, and until correlates of protection are identified, our preliminary findings point toward the following strategy as more evidence-based: (a) a single dose of vaccine for patients already having had laboratory-confirmed COVID-19; and (b) patients who have had laboratory-confirmed COVID-19 may be placed lower on the vaccination priority list.
| Level 4 |
Samanovic MI et al. (Feb 2021) [Prospective Cohort Study – Preprint] Poor antigen-specific responses to the second BNT162b2 mRNA vaccine dose in SARS-CoV-2-experienced individuals[23]
Vaccine candidates have demonstrated robust humoral responses and protective efficacy against infection. However, efficacy trials were focused on individuals with no prior exposure to SARS-CoV-2; and, as a result, little is known about immune responses induced by these mRNA vaccines in individuals who have recovered from COVID-19. The authors evaluated immune responses in 32 subjects who received two-dose Pfizer-BioNTech BNT162b2 mRNA vaccination. In individuals naive to SARS-CoV-2, robust increases in humoral and antigen-specific antibody-secreting cell (ASC) responses following each dose of vaccine were observed; however, individuals with prior exposure to SARS-CoV-2 demonstrated strong humoral and antigen-specific ASC responses to the first dose, but muted responses to the second dose of the vaccine for the time-points studied. These data highlight an important gap in our knowledge and may have major implications for how these vaccines should be used to prevent COVID-19.
| Level 4 |
Tré-Hardy M et al. (April 2021) [Prospective Cohort Study] Reactogenicity, safety and antibody response, after one and two doses of mRNA-1273 in seronegative and seropositive healthcare workers[24]
With the start of worldwide vaccination campaigns, evidence is emerging from the medical literature to dispute the second injection of mRNA vaccines in individuals previously infected with SARS-CoV-2. Knowing that a significant proportion of the population would be seropositive at the time of the first injection, the authors investigated the utility of a second dose under both supply and time constraints in a cohort of healthcare workers (HCWs) who were administered mRNA-1273 at the inception of the national vaccination campaign. Manisty et al. first questioned the administration of the second dose of BNT162b2 — another mRNA vaccine — in order to reserve it only for individuals not previously infected, and showed that the antibody response after a first dose in HCWs previously infected (n=24) reached levels 140 times higher than their peak value before vaccination. Krammer et al. observed in previously infected individuals antibody titers 10 to 45 times higher than in their uninfected counterparts after a first-dose of either BNT162b2 (n=88) or mRNA-1273 (n=22) vaccines.
In the present study, the authors compared not only the antibody response but also the local and systemic side effects in terms of duration and intensity after the first and second dose of mRNA-1273. Quantitative analysis of the anti-SARS-CoV-2 IgG antibodies directed against the subunits (S1 and S2) of the virus sSpike protein was carried out using the LIAISON®SARS-CoV-2 IgG kit (DiaSorin®, Saluggia, Italy) on a LIAISON®XL analyzer previously laboratory validated. In order to assess the serological status of the participants (n=160), a first dosage was carried out with a median time (± 95% confidence interval [CI]) of 2 (± 0.29) days before the first injection (T0). Among those, 36 participants were found to be seropositive. Two other samples were taken from all participants 2 weeks after the first injection (T1) (median time [± 95% CI]: 16 [± 0.25] days), and 2 weeks after the second injection (T2) (median time [± 95% CI]: 14 [± 0.21] days). Except for 2 individuals, all participants who were seropositive at T0 saw their antibody levels boosted by the first dose, but no additional boosting effect was observed after the second injection; in these two individuals (1.6%), the second injection made it possible to raise their antibody levels from 59.7 and 105 AU/mL to above the maximum detection limit (> 400 AU/mL) at T2. In seronegative participants, the anti-S antibody titers obtained after a single dose were comparable to those obtained in unvaccinated seropositive participants, while the second injection was necessary to achieve higher antibody levels approaching those obtained for seropositive individuals (T1). The authors also explored the frequency of side effects after the first dose in a slightly larger cohort (n=206, mean age, 48.6 (± 11.6) years) including 151 seronegative (71% female) and 55 seropositive participants (69% female), as well as after the second dose in 113 participants (mean age, 49.2 (± 11.3) years) including 89 seronegative participants (69% female) and 24 seropositive participants (58% female). The intensity of local and systemic side effects reported by participants was graded into 4 levels of severity: very mild; mild; moderate; severe. Common side effects such as articular pain, muscular pain, headache, fatigue, fever, adenopathy and oedema from the first dose appear to be more frequent and severe in previously infected individuals (p<0.05). Nevertheless, it seems that the second injection generates a greater overall systemic reaction than that observed after the first injection, regardless of initial serological status of the participants. 7 days after the first or second dose, all observed side effects disappeared in all participants, and none were hospitalized. 2 weeks after the last injection, a clinical follow-up questionnaire was sent to the 113 participants. Only 41 were returned at the time of redaction. None of the respondents reported infection. 10 respondents had to undergo a RT-qPCR and all were negative.
| Level 4 |
Shields A et al. (Feb 2021) [Longitudinal Study – Preprint] Longitudinal protection following natural SARS-CoV-2 infection and early vaccine responses: insights from a cohort of community based dental health care professionals[25]
Natural infection leads to a serological response that remains detectable in over 70% of individuals 6 months after initial sampling and 9 months from the peak of the first wave of the pandemic. Post-vaccination, antibody responses were more rapid and of higher magnitude in individuals with who were seropositive at baseline. Following a single dose of vaccine in naive recipients, SARS-CoV-2 antibodies were detectable in over 95% of individuals 12 days after vaccination and persisted >25 days post vaccination.
| Level 4 |
Chodick G et al. (Jan 2021) [Retrospective Cohort Study – Preprint] The effectiveness of the first dose of BNT162b2 vaccine in reducing SARS-CoV-2 infection 13-24 days after immunization: real-world evidence[26]
Background: BNT162b2 vaccines showed high efficacy against COVID-19 in a randomized controlled phase 3 trial. A vaccine effectiveness evaluation in real life settings is urgently needed, especially given the global disease surge. The authors assessed the short-term effectiveness of the first dose of BNT162b2 vaccine against SARS-CoV-2 infection. Given the BNT162b2 phase 3 results, the authors hypothesized that the cumulative incidence of SARS-CoV-2 infection among vaccinees will decline after 12 days following immunization compared to the incidence during the preceding days.
Methods: The study population consisted of all members aged ≥16 years who were vaccinated with BNT162b2-vaccine between December 19, 2020 and January 15, 2021 in Israel. The authors collected information regarding medical history and positive SARS-CoV-2 PCR tests from days after first dose to January 17, 2021. Daily and cumulative infection rates in days 13-24 were compared to days 1-12 after first dose using Kaplan-Meier survival analysis and generalized linear models.
Findings: Data of 503,875 individuals (mean age 59·7 years SD=14·7, 47·8% males) were analyzed, of whom 351,897 had 13-24 days of follow-up. The cumulative incidence of SARS-CoV-2 infection was 0·57% (n=2484) during days 1-12 and 0·27% (n=614) in days 13-24. A 51·4% relative risk reduction (RRR) was calculated in weighted-average daily incidence of SARS-CoV-2 infection from 43·41 per 100,000 (SE=12·07) in days 1-12 to 21·08 per 100,000 (SE=6·16) in days 13-24 following immunization. The decrement in incidence was evident from day 18 after first dose. Similar RRRs were calculated in individuals aged 60 or above (44.5%), younger individuals (50.2%), females (50.0%) and males (52.1%). Findings were similar in sub-populations and patients with various comorbidities.
Conclusions: The findings showed that the first dose of the vaccine is associated with an approximately 51% reduction in the incidence of PCR-confirmed SARS-CoV-2 infections at 13 to 24 days after immunization compared to the rate during the first 12 days. Similar levels of effectiveness were found across age groups, sex, as well as among individuals residing in Arab or ultra-orthodox Jewish communities that display an increased COVID-19 risk.
Implications of all the available evidence: Together our findings and the 95% efficacy shown in the phase 3 trial suggest that the BNT162b2 vaccine should be administered in 2 doses to achieve maximum protection and impact in terms of disease burden reduction and possibly reducing SARS-CoV-2 transmission. COVID-19 vaccines should be urgently deployed globally.
| Level 4 |
Vasileiou E et al. (May 2021) [Prospective Cohort Study] Interim findings from first-dose mass COVID-19 vaccination roll-out and COVID-19 hospital admissions in Scotland: a national prospective cohort study[27]
Background: The BNT162b2 mRNA Pfizer-BioNTech and ChAdOx1 Oxford-AstraZeneca COVID-19 vaccines have demonstrated high efficacy against infection in phase 3 clinical trials and are now being used in national vaccination programmes in Britain and several other countries. There is an urgent need to study the real-world effects of these vaccines. The aim of the present study was to estimate the effectiveness of the first dose of these COVID-19 vaccines in preventing hospital admissions.
Methods: A prospective cohort study using the Early Pandemic Evaluation and Enhanced Surveillance of COVID-19 (EAVE II) database comprising of linked vaccination, primary care, reverse-transcription polymerase chain reaction (RT-PCR) testing, hospitalization and mortality records for 5.4 million people in Scotland, covering ~99% of the population. A time-dependent Cox model and Poisson regression models were fitted to estimate effectiveness against COVID-19 related hospitalization following the first dose of vaccine.
Findings: Between December 8, 2020 and February 22, 2021, a total of 1,331,993 people were vaccinated over the study period. The mean age of those vaccinated was 65·0 years (SD 16·2). The first dose of the BNT162b2 mRNA vaccine was associated with a vaccine effect of 91% (95% CI 85-94) for reduced COVID-19 hospital admission at 28-34 days post-vaccination. Vaccine effect at the same time interval for the ChAdOx1 vaccine was 88% (95% CI 75-94). Results of combined vaccine effects against hospital admission due to COVID-19 were similar when restricting the analysis to those aged 80 years and older (83%, 95% CI 72-89 at 28-34 days post-vaccination).
Interpretation: Mass roll-out of the first doses of the BNT162b2 mRNA and ChAdOx1 vaccines was associated with substantial reductions in the risk of hospital admission due to COVID-19 in Scotland. There remains the possibility that some of the observed effects might have been due to residual confounding.
[1] Vasileiou E, Simpson CR, Shi T, Kerr S, Agrawal U, Akbari A, Bedston S, Beggs J, Bradley D, Chuter A, de Lusignan S, Docherty AB, Ford D, Hobbs FR, Joy M, Katikireddi SV, Marple J, McCowan C, McGagh D, McMenamin J, Moore E, Murray JL, Pan J, Ritchie L, Shah SA, Stock S, Torabi F, Tsang RS, Wood R, Woolhouse M, Robertson C, Sheikh A. Interim findings from first-dose mass COVID-19 vaccination roll-out and COVID-19 hospital admissions in Scotland: a national prospective cohort study. Lancet. 2021 May 1;397(10285):1646-1657. doi: 10.1016/S0140-6736(21)00677-2. Epub 2021 Apr 23. PMID: 33901420; PMCID: PMC8064669.
| Level 5 |
Manisty C et al. (Feb 2021) [Nested Case Control Analysis] Antibody response to first BNT162b2 dose in previously SARS-CoV-2-infected individuals[28]
Rapid vaccine-induced population immunity is a key global strategy to control COVID-19. Vaccination programmes must maximize early impact, particularly with accelerated spread of new variants. Most vaccine platforms use a two-dose prime-boost approach to generate an immune response against the virus S1 sSpike protein, the titres of which correlate with functional virus neutralization and increase with boosting.
To enable larger numbers of people to receive the first dose, delayed administration of the second dose has been advocated and implemented by some jurisdictions. The impact of previous SARS-CoV-2 infection on the need for boosting is not known. The authors assumed that previous infection could be analogous to immune priming. As such, a first prime vaccine dose would effectively act as a boost, so a second dose might not be needed. To test their assumption, the authors undertook a nested case-control analysis of 51 participants of COVIDsortium, an ongoing longitudinal observational study of healthcare workers (HCWs) in London who underwent weekly PCR and quantitative serology testing from the day of the first lockdown in Britain on 23 March 2020, and for 16 weeks onwards. 24 of 51 HCWs had a previous laboratory-confirmed mild or asymptomatic SARS-CoV-2 infection, as confirmed by positive detection of antibodies against the SARS-CoV-2 nucleocapsid or the receptor binding domain of the SARS-CoV-2 S1 subunit of the sSpike protein, whereas 27 HCWs remained seronegative. A median of 12.5 sampling time-points per participant permitted the identification of peak antibody titres in seropositive individuals while avoiding false negatives.
| Level 5 |
Hyams C et al. (March 2021) [Case Control Study – Preprint] Assessing the Effectiveness of BNT162b2 and ChAdOx1nCoV-19 COVID-19 Vaccination in Prevention of Hospitalizations in Elderly and Frail Adults: A Single Centre Test Negative Case-Control Study[29]
Background: On 8 December 2020, deployment of the first vaccine against SARS-CoV-2 authorised for use in Britain, the mRNA-based vaccine BNT162b2, began, followed by the adenoviral vector vaccine ChAdOx1nCoV-19 on 4 January 2021. Initially care home residents and staff, frontline healthcare workers and adults from age 80 were targeted. In phase 3 trials, BNT162b2 and ChAdOx1nCoV-19 demonstrated 95% and 70% efficacy, respectively, after two doses against symptomatic SARS-CoV-2 infection. However, few data exist regarding the effectiveness of these vaccines in elderly frail people. Evaluation following implementation to determine the effectiveness of one dose in reducing hospitalizations due to SARS-CoV-2 infection in elderly adults is urgent.
Methods: A prospective single-centre test-negative design case-control study of adults aged ≥80 years hospitalized with COVID-19 disease or other acute respiratory disease. The authors conducted logistic regression controlling for time (week), gender, index of multiple deprivations (IMD) and care residency status (CRS), and sensitivity analyses matched for time and gender using a conditional logistic model adjusting for IMD and CRS.
Findings: First dose vaccine effectiveness of BNT162b2 was 71.4% (95% confidence interval [CI] 46.5-90.6). ChAdOx1nCoV-19 first dose vaccine effectiveness was 80.4% (95% CI 36.4-94.5). When effectiveness analysis for BNT162b2 was restricted to the period covered by ChAdOx1nCoV-19, the estimate was 79.3% (95% CI 47.0-92.5).
Interpretation: A single dose of either BNT162b2 or ChAdOx1nCoV-19 vaccine resulted in substantial reductions in the risk of COVID-19-related hospitalization in elderly, frail patients with extensive co-morbid disease.
| Level 6 |
Aran D (Feb 2021)Estimating real-world COVID-19 vaccine effectiveness in Israel using aggregated counts[30]
The vaccination roll-out of the COVID-19 vaccines in Israel has been highly successful. By 22 February 2021, approximately 47% of the population had already been administered at least one dose of the Pfizer-BioNTech vaccine. Efforts to estimate the real-world effectiveness of the vaccine have been hampered by disease dynamics and socio-economic discrepancies. Here, using counts of positive and hospitalized cases of vaccinated individuals, the authors conducted a sensitivity analysis of vaccine effectiveness. Under an assumption of no effectiveness during the first two weeks after the first dose, the authors observed very low effectiveness on the third week. After the second dose, on weeks 1 and 2 the authors found 73%-85% effectiveness in reducing positive cases, hospitalizations and severe cases, which increased to 89%-97% effectiveness 14 days after the second dose. As more granular data become available, it will be possible to extract more exact estimates; however, the emerging evidence suggests that the vaccine is highly effective.
| Level 6 |
Rossman H et al. (April 2021) Patterns of COVID-19 pandemic dynamics following deployment of a broad national immunization program[31]
The authors conducted a retrospective analysis of data from the Israeli Ministry of Health collected between 28 August 2020 and 24 February 2021. The temporal dynamics of the number of new COVID-19 cases and hospitalizations after the vaccination campaign, which was initiated on 20 December 2020, were observed. To distinguish the possible effects of the vaccination on cases and hospitalizations from other factors, including a third lockdown implemented on 8 January 2021, several comparisons were performed: 1) individuals aged 60 years and older prioritized to receive the vaccine first versus younger age groups; 2) the January lockdown versus the September lockdown; and 3) early-vaccinated cities and geographical statistical areas (GSAs) versus late-vaccinated cities and GSAs. A larger and earlier decrease in COVID-19 cases and hospitalizations was observed in individuals older than 60 years, followed by younger age groups, by the order of vaccination prioritization. This pattern was not observed in the previous lockdown and was more pronounced in early-vaccinated cities. This analysis demonstrates the real-life effect of a national vaccination campaign on the dynamics of the pandemic.
| Level 7 |
Lustig Y et al. (April 2021) [Correspondence] Neutralizing Response against Variants after SARS-CoV-2 Infection and One Dose of BNT162b2[32]
In their small study of six health care workers previously infected with SARS-CoV-2, the authors reported that one Pfizer-BioNTech mRNA vaccine dose substantially increased neutralizing activity against all variants tested (the original virus of B.1 sublineage, B.1.1.7, B.1.351, and P.1 variants), with similar titers detected across patients for each variant. This highlights the importance of vaccination even in previously infected patients, given the added benefit of an increased antibody response to the variants tested.
| Level 7 |
Amit, S et al. (March 2021) [Correspondence] Early rate reductions of SARS-CoV-2 infection and COVID-19 in BNT162b2 vaccine recipients[33]
To assess vaccine-associated rate reductions, the authors analyzed a retrospective cohort of 9,109 vaccine-eligible health care workers (HCWs), comparing vaccinated versus unvaccinated. Active daily symptom reporting and immediate same-day testing allowed for prompt (<24h) detection and investigation of exposed or symptomatic HCWs.
Data show substantial early reductions in SARS-CoV-2 infection and symptomatic COVID-19 rates following first vaccine dose administration. Early reductions of COVID-19 rates provide support for delaying the second dose in countries facing vaccine shortages and scarce resources to allow higher population coverage with a single dose. Longer follow-up to assess long-term effectiveness of a single dose is needed to inform a second dose delay policy.
| Level 7 |
Moore JP (April 2021) [Editorial] Approaches for Optimal Use of Different COVID-19 Vaccines: Issues of Viral Variants and Vaccine Efficacy[34]
“Small-scale studies have shown that a single mRNA vaccine dose [administered to individuals who have previously been infected with SARS-CoV-2] rapidly boosts neutralizing antibody titers to very high levels, perhaps rendering the second dose redundant in this special circumstance. Considering the number of people in the US who have had COVID-19, there is a potential to save tens of millions of vaccine doses. Although logistically this would be a major challenge, the French government has already adopted this policy. A related issue is that the mRNA vaccines appear to trigger strong (although short-lived) adverse effects (such as headaches and mild fever) in people who have previously been infected with COVID-19. One potential solution to the adverse effect problem might be to use the Novavax protein vaccine (if it is approved) to boost antibody levels in patients who have recovered from COVID-19, particularly for younger individuals. This vaccine seems to elicit fewer adverse effects than the mRNA vaccines but had comparable efficacy in a UK phase 3 trial. However, data from carefully designed clinical trials are needed to address these issues and inform the best decisions.”
References
[1] World Health Organization (21 April 2021). Interim recommendations for use of the ChAdOx1-S [recombinant] vaccine against COVID-19 (AstraZeneca COVID-19 vaccine AZD1222, SII Covishield, SK Bioscience). https://www.who.int/publications/i/item/WHO-2019-nCoV-vaccines-SAGE_recommendation-AZD1222-2021.1. Accessed 26/05/2021.
[2] World Health Organization (17 March 2021) Interim recommendations for the use of the Janssen Ad26.COV2.S (COVID-19) vaccine.
https://www.who.int/publications/i/item/WHO-2019-nCoV-vaccines-SAGE-recommendation-Ad26.COV2.S-2021.1. Accessed 26/05/2021.
[3] World Health Organization (25 January 2021) Interim recommendations for use of the Moderna mRNA-1273 vaccine against COVID-19.
https://www.who.int/publications/i/item/interim-recommendations-for-use-of-the-moderna-mrna-1273-vaccine-against-covid-19. Accessed 26/05/2021.
[4] World Health Organization (8 January 2021) Interim recommendations for use of the Pfizer–BioNTech COVID-19 vaccine, BNT162b2, under Emergency Use Listing.
https://www.who.int/publications/i/item/WHO-2019-nCoV-vaccines-SAGE_recommendation-BNT162b2-2021.1. Accessed 26/05/2021.
[5] Centers for Disease Control and Prevention. Interim Clinical Considerations for Use of COVID-19 Vaccines Currently Authorized in the United States (last reviewed March 2021) https://www.cdc.gov/vaccines/COVID-19/info-by-product/clinical-considerations.html#Administration Accessed 19/04/2021.
[6] European Centre for Disease Control and Prevention (2021) Overview of the implementation of COVID-19 vaccination strategies and vaccine deployment plans in the EU/EEA 29 March 2021https://www.ecdc.europa.eu/en/publications-data/overview-implementation-covid-19-vaccination-strategies-and-vaccine-deployment. Accessed 07/04/2021.
[7] Haute Autorité de Santé (12 February 2021) SARS-CoV-2 vaccination strategy – vaccination of people with a history of Covid-19. https://www.has-sante.fr/jcms/p_3237271/en/strategie-de-vaccination-contre-le-sars-cov-2-vaccination-des-personnes-ayant-un-antecedent-de-covid-19. Accessed 27/05/2021.
[8] Federal Office of Public Health (Switzerland) Coronavirus: Frequently Asked Questions (FAQs). https://www.faq.bag.admin.ch/en. Accessed 27/05/2021.
[9] UptoDate COVID-19: Vaccines to prevent SARS-CoV-2 infection, April 2021. https://www.uptodate.com/contents/covid-19-vaccines-to-prevent-sars-cov-2-infection . Accessed 27/5/2021.
[10] Krammer F, Srivastava K, The PARIS team, Simon V. Robust Spike antibody responses and increased reactogenicity in seropositive individuals after a single dose of SARS-CoV-2 mRNA vaccinemedRxiv 2021.01.29.21250653; doi: https://doi.org/10.1101/2021.01.29.21250653. Accessed 6/4/2021.
[11] Abu Jabal K, Ben-Amram H, Beiruti K, Batheesh Y, Sussan C, Zarka S, Edelstein M. Impact of age, ethnicity, sex and prior infection status on immunogenicity following a single dose of the BNT162b2 mRNA COVID-19 vaccine: real-world evidence from healthcare workers, Israel, December 2020 to January 2021. Euro Surveill. 2021 Feb;26(6):2100096. doi: 10.2807/1560-7917.ES.2021.26.6.2100096. PMID: 33573712; PMCID: PMC7879501. https://www.eurosurveillance.org/content/10.2807/1560-7917.ES.2021.26.6.2100096. Accessed 27/05/2021.
[12] Angyal, Adrienn and Longet, Stephanie and Moore, Shona and Payne, Rebecca P. and Harding, Adam and Tipton, Tom and Rongkard, Patpong and Ali, Mohammad and Hering, Luisa M. and Meardon, Naomi and Austin, James and Brown, Rebecca and Skelly, Donal and Gillson, Natalie and Dobson, Sue L. and Cross, Andrew and Sandhar, Gurjinder and Kilby, Jonathan A. and Tyerman, Jessica K. and Nicols, Alexander R. and Spegarova, Jarmila S. and Mehta, Hema and Hornsby, Hailey and Whitham, Rachel and Conlon, Christopher P. and Jeffery, Katie and Goulder, Philip and Frater, John and Dold, Christina and Pace, Matthew and Ogbe, Ane and Brown, Helen and Ansari, Azim M. and Adland, Emily and Brown, Anthony and Chand, Meera A. and Shields, Adrian and Matthews, Philippa and Hopkins, Susan and Hall, Victoria Jane and James, William and Rowland-Jones, Sarah L. and Klenerman, Paul and Dunachie, Susanna and Richter, Alex G. and Duncan, Christopher J. A. and Barnes, Eleanor and Carroll, Miles W. and Turtle, Lance and de Silva, Thushan I. and Consortium, PITCH, T-Cell and Antibody Responses to First BNT162b2 Vaccine Dose in Previously SARS-CoV-2-Infected and Infection-Naive UK Healthcare Workers: A Multicentre, Prospective, Observational Cohort Study. Available at SSRN: https://ssrn.com/abstract=3812375 or http://dx.doi.org/10.2139/ssrn.3812375 . Accessed 27/5/202.
[13] Bradley T, Grundberg E, Selvarangan R. Antibody responses boosted in seropositive healthcare workers after single dose of SARS-CoV-2 mRNA vaccine. medRxiv [Preprint]. 2021 Feb 5:2021.02.03.21251078. doi: 10.1101/2021.02.03.21251078. PMID: 33564797; PMCID: PMC7872392.
[14] Callegaro A, Borleri D, Farina C, Napolitano G, Valenti D, Rizzi M, Maggiolo F. Antibody response to SARS-CoV-2 vaccination is extremely vivacious in subjects with previous SARS-CoV-2 infection. J Med Virol. 2021 Mar 31. doi: 10.1002/jmv.26982. Epub ahead of print. PMID: 33788281.
[15] Ciccone EJ, Zhu DR, Ajeen R, Lodge EK, Shook-Sa BE, Boyce RM, Aiello AE. SARS-CoV-2 seropositivity after infection and antibody response to mRNA-based vaccination. medRxiv [Preprint]. 2021 Feb 22:2021.02.09.21251319. doi: 10.1101/2021.02.09.21251319. PMID: 33619498; PMCID: PMC789946
[16] Ebinger JE, Fert-Bober J, Printsev I, Wu M, Sun N, Figueiredo JC, Eyk JEV, Braun JG, Cheng S, Sobhani K. Prior COVID-19 Infection and Antibody Response to Single Versus Double Dose mRNA SARS-CoV-2 Vaccination. medRxiv [Preprint]. 2021 Feb 26:2021.02.23.21252230. doi: 10.1101/2021.02.23.21252230. PMID: 33655279; PMCID: PMC7924304.
[17] Ebinger JE, Fert-Bober J, Printsev I, Wu M, Sun N, Prostko JC, Frias EC, Stewart JL, Van Eyk JE, Braun JG, Cheng S, Sobhani K. Antibody responses to the BNT162b2 mRNA vaccine in individuals previously infected with SARS-CoV-2. Nat Med. 2021 Apr 1. doi: 10.1038/s41591-021-01325-6. Epub ahead of print. PMID: 33795870.
[18] Gobbi F, Buonfrate D, Moro L, Rodari P, Piubelli C, Caldrer S, Riccetti S, Sinigaglia A, Barzon L. Antibody Response to the BNT162b2 mRNA COVID-19 Vaccine in Subjects with Prior SARS-CoV-2 Infection. Viruses. 2021 Mar 5;13(3):422. doi: 10.3390/v13030422. PMID: 33807957.
[19] Goel RR, Apostolidis SA, Painter MM, Mathew D, Pattekar A, Kuthuru O, Gouma S, Kuri-Cervantes L, Meng W, Adamski S, Baxter AE, Giles JR, Weirick ME, McAllister CM, Hicks A, Korte S, Dougherty J, Long S, D’Andrea K, Hamilton JT, Luning Prak ET, Betts MR, Bates P, Hensley SE, Greenplate AR, Wherry EJ. Longitudinal Analysis Reveals Distinct Antibody and Memory B Cell Responses in SARS-CoV-2 Naïve and Recovered Individuals Following mRNA Vaccination. medRxiv [Preprint]. 2021 Mar 6:2021.03.03.21252872. doi: 10.1101/2021.03.03.21252872. PMID: 33688691; PMCID: PMC7941668.
[20] Levi R, Azzolini E, Pozzi C, Ubaldi L, Lagioia, M, Mantovani A, Rescigno M. A cautionary note on recall vaccination in ex-COVID-19 subjects. medRxiv 2021.02.01.21250923; doi: https://doi.org/10.1101/2021.02.01.21250923. Accessed 26/5/2021.
[21] Prendecki M, Clarke C, Brown J, Cox A, Gleeson S, Guckian M, Randell P, Pria AD, Lightstone L, Xu XN, Barclay W, McAdoo SP, Kelleher P, Willicombe M. Effect of previous SARS-CoV-2 infection on humoral and T-cell responses to single-dose BNT162b2 vaccine. Lancet. 2021 Mar 27;397(10280):1178-1181. doi: 10.1016/S0140-6736(21)00502-X. Epub 2021 Feb 25. PMID: 33640037; PMCID: PMC7993933.
[22] Saman Saadat, Zahra Rikhtegaran Tehrani, James Logue, Michelle Newman, Matthew B. Frieman, Anthony D. Harris, Mohammad M. Sajadi Single Dose Vaccination in Healthcare Workers Previously Infected with SARS-CoV-2 medRxiv 2021.01.30.21250843;
doi: https://doi.org/10.1101/2021.01.30.21250843https://www.medrxiv.org/content/10.1101/2021.01.30.21250843v5. Accessed 27/05/2021.
[23] Samanovic MI, Cornelius AR, Wilson JP, Karmacharya T, Gray-Gaillard SL, Allen JR, Hyman SW, Moritz G, Ali M, Koralov SB, Mulligan MJ, Herati RS. Poor antigen-specific responses to the second BNT162b2 mRNA vaccine dose in SARS-CoV-2-experienced individuals. medRxiv [Preprint]. 2021 Feb 9:2021.02.07.21251311. doi: 10.1101/2021.02.07.21251311. PMID: 33594383; PMCID: PMC7885942. [Accessed 6/4/2021]
[24] Tré-Hardy M, Cupaiolo R, Papleux E, Wilmet A, Horeanga A, Antoine-Moussiaux T, Della Vecchia A, Beukinga I, Vekemans M, Blairon L. Reactogenicity, safety and antibody response, after one and two doses of mRNA-1273 in seronegative and seropositive healthcare workers. J Infect. 2021 Apr 1:S0163-4453(21)00158-4. doi: 10.1016/j.jinf.2021.03.025. Epub ahead of print. PMID: 33811939; PMCID: PMC8012163.
[25] Shields A, Faustini F, Kristunas C, Cook A M, Backhouse C et al. Longitudinal protection following natural SARS-CoV-2 infection and early vaccine responses: insights from a cohort of community based dental health care professionals. medRxiv 2021.02.24.21252368; doi: https://doi.org/10.1101/2021.02.24.21252368. Accessed 27/05/2021. [26] Chodick G, Tene L., Gatiz S., Ben Tov A, Cohen D, Mushen K. The effectiveness of the first dose of BNT162b2 vaccine in reducing SARS-CoV-2 infection 13-24 days after immunization: real-world evidence. https://doi.org/10.1101/2021.01.27.21250612 . Accessed 27/05/2021.[27] Vasileiou E, Simpson CR, Shi T, Kerr S, Agrawal U, Akbari A, Bedston S, Beggs J, Bradley D, Chuter A, de Lusignan S, Docherty AB, Ford D, Hobbs FR, Joy M, Katikireddi SV, Marple J, McCowan C, McGagh D, McMenamin J, Moore E, Murray JL, Pan J, Ritchie L, Shah SA, Stock S, Torabi F, Tsang RS, Wood R, Woolhouse M, Robertson C, Sheikh A. Interim findings from first-dose mass COVID-19 vaccination roll-out and COVID-19 hospital admissions in Scotland: a national prospective cohort study. Lancet. 2021 May 1;397(10285):1646-1657. doi: 10.1016/S0140-6736(21)00677-2. Epub 2021 Apr 23. PMID: 33901420; PMCID: PMC8064669.
[28] Manisty C, Otter AD, Treibel TA, McKnight Á, Altmann DM, Brooks T, Noursadeghi M, Boyton RJ, Semper A, Moon JC. Antibody response to first BNT162b2 dose in previously SARS-CoV-2-infected individuals. Lancet. 2021 Mar 20;397(10279):1057-1058. doi: 10.1016/S0140-6736(21)00501-8. Epub 2021 Feb 25. PMID: 33640038; PMCID: PMC7972310.
[29] Hyams C, Marlow R Maseko Z, King J Ward L, Fox K , Heath R , Turner A et al. Assessing the Effectiveness of BNT162b2 and ChAdOx1nCoV-19 COVID-19 Vaccination in Prevention of Hospitalizations in Elderly and Frail Adults: A Single Centre Test Negative Case-Control Study. Available at SSRN: https://ssrn.com/abstract=3796835 or http://dx.doi.org/10.2139/ssrn.3796835. Accessed 26/5/2021.
[30] Aran, D. Estimating real-world COVID-19 vaccine effectiveness in Israel using aggregated counts. https://www.medrxiv.org/content/10.1101/2021.02.05.21251139v3. Accessed 27/05/2021.
[31] Rossman, H., Shilo, S., Meir, T. et al. COVID-19 dynamics after a national immunization program in Israel. Nat Med (2021). https://doi.org/10.1038/s41591-021-01337-2. Accessed 26/5/2021.
[32] Lustig Y, Nemet I, Kliker L, Zuckerman N, Yishai R, Alroy-Preis S, Mendelson E, Mandelboim M. Neutralizing Response against Variants after SARS-CoV-2 Infection and One Dose of BNT162b2. N Engl J Med. 2021 Apr 7:NEJMc2104036. doi: 10.1056/NEJMc2104036. Epub ahead of print. PMID: 33826815; PMCID: PMC8063887.
[33] Amit S, Regev-Yochay G, Afek A, Kreiss Y, Leshem E. Early rate reductions of SARS-CoV-2 infection and COVID-19 in BNT162b2 vaccine recipients. Lancet. 2021 Mar 6;397(10277):875-877. doi: 10.1016/S0140-6736(21)00448-7. Epub 2021 Feb 18. PMID: 33610193; PMCID: PMC7906709. Accessed 26/5/2021.
[34] Moore JP. Approaches for Optimal Use of Different COVID-19 Vaccines: Issues of Viral Variants and Vaccine Efficacy. JAMA. 2021 Apr 6;325(13):1251-1252. doi: 10.1001/jama.2021.3465. PMID: 33662101.
Produced by the members of the National Health Library and Knowledge Service Evidence Team†. Current as at 24 May 2021. This evidence summary collates the best available evidence at the time of writing and does not replace clinical judgement or guidance. Emerging literature or subsequent developments in respect of COVID-19 may require amendment to the information or sources listed in the document. Although all reasonable care has been taken in the compilation of content, the National Health Library and Knowledge Service Evidence Team makes no representations or warranties expressed or implied as to the accuracy or suitability of the information or sources listed in the document. This evidence summary is the property of the National Health Library and Knowledge Service and subsequent re-use or distribution in whole or in part should include acknowledgement of the service.
Helen Clark, Sligo University Hospital [Author]; Margaret Morgan, Midland Regional Hospital Mullingar [Author]; Brendan Leen, Area Library Manager, HSE South [Editor]; NIAC Subgroup Contributors: Dr. Peter O’Reilly; Dr. Niamh Bambury; Dr. Geraldine Casey; Dr. Kenneth Beatty; Dr. Paul Mullane; Dr. Philippa White.

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.