
What is the impact of COVID-19 on people with disabilities in terms of mortality and development of severe illness?
DOWNLOAD FULL SUMMARY OF EVIDENCE (PDF)
The following information resources have been selected by the National Health Library and Knowledge Service Evidence Virtual Team in response to your question. The resources are listed in our estimated order of relevance to practicing healthcare professionals confronted with this scenario in an Irish context. In respect of the evolving global situation and rapidly changing evidence base, it is advised to use hyperlinked sources in this document to ensure that the information you are disseminating to the public or applying in clinical practice is the most current, valid and accurate. For further information on the methodology used in the compilation of this document – including a complete list of sources consulted – please see our National Health Library and Knowledge Service Summary of Evidence Protocol.
Main Points
- Data from international COVID-19 outbreaks has identified significant levels of mortality and morbidity in high-risk groups.
- Most people with disabilities are not inherently at higher risk of becoming infected with or having severe illness from COVID-19. They are at greater risk because of the pre-existing health condition(s) underlying the disability, and barriers to accessing healthcare.
- People with developmental or behavioural disorders who have serious underlying medical conditions may be at risk of serious illness.
- People with intellectual disabilities are vulnerable due to disparity in healthcare provision and physical and mental health multimorbidity.
- COVID-19 appears to present a greater risk to people with intellectual and developmental disabilities, especially those living in residential care settings.
Summary of Evidence
The Health Protection Surveillance Centre states that data from international COVID-19 outbreaks has identified significant levels of mortality and morbidity in high-risk groups. Particular attention is required when considering how the needs of vulnerable people are managed to support prevention, identification and clinical management scenarios arising within them1.
Disability alone may not be related to higher risk for getting COVID-19 or having severe illness. Most people with disabilities are not inherently at higher risk of becoming infected with or having severe illness from COVID-19. However, some people with disabilities might be at a higher risk of infection or severe illness because of their underlying medical conditions2, 3. People with developmental or behavioural disorders who have serious underlying medical conditions may be at risk of serious illness4.
BMJ Best Practice reports that in the UK, the death rate from COVID-19 is higher in people with learning disabilities than in the general population. People with learning disabilities were over-represented threefold amongst people who died from COVID-19, with a larger disparity in younger age groups5.
Robust evidence associating specific underlying conditions with severe illness in children is limited6. Conditions which may be associated with increased risk of severe disease in children include medical complexity, severe genetic disorders, and severe neurological disorders. Down Syndrome has also been proposed to predispose to severe disease6. Individuals with Down Syndrome deceased with COVID-19 are younger than individuals without Down Syndrome. The burden of co-occurring medical conditions and increased risk of complications can influence COVID-19 prognosis in individuals with Down Syndrome. Specific strategies to prevent and mitigate the effects of COVID-19 in the population with Down Syndrome are needed19. Risk factors and co-occurring medical conditions can contribute to more severe clinical presentations of COVID-19 in this population23. Leading signs/symptoms of COVID-19 and risk factors for severe disease course are similar to the general population. However, individuals with Down Syndrome present significantly higher rates of mortality, especially from age 4010.
Cuyper’s findings suggest that a pandemic may disproportionally affect people with intellectual disabilities while population data may not immediately raise warnings. Early detection of diverging patterns and faster implementation of tailored strategies therefore require collection of good quality data8.
People with intellectual and developmental disabilities living in residential group homes may be at greater risk of severe COVID-19 outcomes. However, a full understanding of the severity of this risk will not be possible until all relevant data on COVID-19 outcomes among this population is publicly shared12.
Multiple sclerosis (MS) patients have been considered a higher-risk population for COVID-19 due to the high prevalence of disability and disease-modifying therapy use; however, there is little data identifying clinical characteristics of MS associated with worse COVID-19 outcomes9. In their multicentre prospective cohort study, Chaudhry et al found that MS patients with more severe COVID-19 courses tended to be older, were more likely to suffer from progressive phenotype, and had a higher degree of disability7.
The data from a descriptive study looking at COVID-19 deaths in people with intellectual disability in the UK and Ireland provides insight into possible factors for deaths in people with intellectual disabilities. Some of the factors varied between the mild and moderate-to-profound intellectual disability groups. This highlights an urgent need for further systemic inquiry and study of the possible cumulative impact of these factors and co-occurring medical conditions given the possibility of COVID-19 resurgence18.
Irish and/or International Guidance
Data from international COVID-19 outbreaks has identified significant levels of mortality and morbidity in high-risk groups. Therefore, particular attention is required when considering how the needs of vulnerable people are managed to support prevention, identification and clinical management scenarios arising within them. Structured approaches to supportive care and anticipatory planning may also affect the course and disease outcomes although evidence at this stage of the outbreak is limited in this regard. This document gives general advice on the management of those with disabilities in community settings. It also gives specific advice for named scenarios and includes supporting information in appendices.
World Health Organization (2020) Disability considerations during the COVID-19 outbreak[ii]
People with disability may be at greater risk of developing severe disease if they become infected because of the preexisting health condition underlying the disability and barriers to accessing healthcare. People with disability may also be disproportionately impacted by the outbreak because of serious disruptions to the services they rely on. The barriers experienced by people with disability can be reduced if key stakeholders take appropriate action.
Centers for Disease Control and Prevention (United States) (2021) People with disabilities[iii]
Disability alone may not be related to higher risk for getting COVID-19 or having severe illness. Most people with disabilities are not inherently at higher risk for becoming infected with or having severe illness from COVID-19. However, some people with disabilities might be at a higher risk of infection or severe illness because of their underlying medical conditions. All people seem to be at higher risk of severe illness from COVID-19 if they have serious underlying chronic medical conditions such as chronic lung disease, a serious heart condition or a weakened immune system. Adults with disabilities are three times more likely than adults without disabilities to have heart disease, stroke, diabetes or cancer than adults without disabilities.
Centers for Disease Control and Prevention (United States) (2021) People with developmental and behavioral disorders[iv]
Most people with developmental or behavioural disorders are not naturally at higher risk of becoming infected with or having severe illness from novel coronavirus (COVID-19). However, people with developmental or behavioural disorders who have serious underlying medical conditions may be at risk of serious illness.
Point-of-Care Tools
BMJ Best Practice (2021) Management of coexisting conditions in the context of COVID-19[v]
In the UK, the death rate from COVID-19 is higher in people with learning disabilities (LDs) than in the general population. People with LDs were over-represented threefold amongst people who died from COVID-19, with a larger disparity in younger age groups. Guidance recommends ensuring that patients with LDs have a handheld summary of their medical information, activities and preferences to support staff in caring for them if admitted to hospital. Community LD teams are encouraged to work with people in their care and their families to develop COVID-19 care plans, which should include any issues associated with diagnostic overshadowing, views of parents, carers and family members, any reasonable adjustments required, communication needs, specialist mental health support, anticipatory care plans, and any end-of-life or do not attempt cardiopulmonary resuscitation discussions. Stringent social distancing should be followed, and community services should use tele- and video conferencing to contact patients and carers where appropriate.
Although children with underlying medical conditions are at greater risk for severe disease ¾ eg hospitalisation, need for intensive care or mechanical ventilation, death ¾ than children without underlying conditions, robust evidence associating specific underlying conditions with severe illness in children is limited. Conditions which may be associated with increased risk of severe disease in children include medical complexity, severe genetic disorders, and severe neurological disorders. Down Syndrome has also been proposed to predispose to severe disease. Age <1 year also has been associated with increased risk for severe disease, but this finding is inconsistent.
Irish and/or International Literature
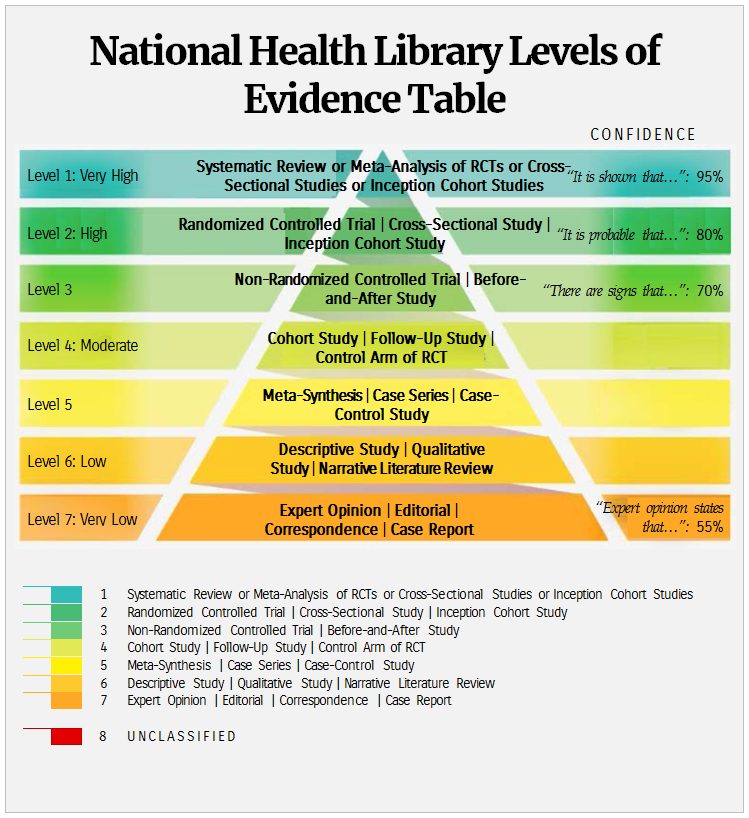
Please refer to the National Health Library Levels of Evidence Table used to grade the levels of evidence included in this section.
Inclusion criteria: all studies, levels 1-8. Exclusion criteria: none.
| Level 4 |
There is little data identifying clinical characteristics of multiple sclerosis (MS) associated with worse COVID-19 outcomes. Therefore, we conducted a multicentre prospective cohort study looking at the outcomes of 40 MS patients with confirmed COVID-19. Severity of COVID-19 infection was based on hospital course, where a mild course was defined as the patient not requiring hospital admission, moderate severity was defined as the patient requiring hospital admission to the general floor, and most severe was defined as requiring intensive care unit admission and/or death. 19/40(47.5%) had mild courses, 15/40(37.5%) had moderate courses, and 6/40(15%) had severe courses. Patients with moderate and severe courses were significantly older than those with a mild course (57[50-63] years old and 66[58.8-69.5] years old vs 48[40-51.5] years old, P = 0.0121, P = 0.0373). There was differing prevalence of progressive MS phenotype in those with more severe courses (severe:2/6[33.3%] primary-progressing and 0/6[0%]secondary-progressing, moderate:1/14[7.14%] and 5/14[35.7%] vs mild:0/19[0%] and 1/19[5.26%], P = 0.0075, 1 unknown). Significant disability was found in 1/19(5.26%) mild course-patients, but was in 9/15(60%, P = 0.00435) of moderate course-patients and 2/6(33.3%, P = 0.200) of severe course-patients. Disease-modifying therapy prevalence did not differ among courses (mild:17/19[89.5%], moderate:12/15[80%] and severe:3/6[50%], P = 0.123). MS patients with more severe COVID-19 courses tended to be older, were more likely to suffer from progressive phenotype, and had a higher degree of disability. However, disease-modifying therapy use was not different among courses.
| Level 4 |
Background: Data on the development of COVID‐19 among people with intellectual disabilities (IDs) are scarce and it is uncertain to what extent general population data applies to people with ID. To give an indication of possible implications, this study investigated excess mortality patterns during a previous influenza epidemic.
Methods: Using Dutch population and mortality registers, a historical cohort study was designed to compare mortality during the 2017–2018 influenza epidemic with mortality in the same period in the three previous years. People with ID were identified by entitlements to residential ID care services as retrieved from a national database.
Results: Data covered the entire adult Dutch population (12.6 million; GenPop), of which 91 064 individuals were identified with an ID. During the influenza epidemic, mortality among people with ID increased almost three times as much than in the GenPop (15.2% vs. 5.4%), and more among male individuals with ID (+19.5%) than among female individuals with ID (+10.6%), as compared with baseline. In both cohorts, comparable increases in mortality within older age groups and due to respiratory causes were seen. Particularly in the ID cohort, excess deaths also occurred in younger age groups, due to endocrine diseases and ID specific causes.
Conclusions: During the 2017–2018 influenza epidemic, excess mortality among people with ID was three times higher than in the general Dutch population, appeared more often at young age and with a broader range of underlying causes. These findings suggest that a pandemic may disproportionally affect people with ID while population data may not immediately raise warnings. Early detection of diverging patterns and faster implementation of tailored strategies therefore require collection of good quality data.
| Level 4 |
Background: The impact of the coronavirus disease 2019 (COVID-19) pandemic on people with multiple sclerosis (MS) is a major current concern, in particular the risk of death. Here we describe the impact of the first wave of COVID-19 infections (Mar 2020-July 2020) on the Scottish MS Register (SMSR) population, a cohort of 4702 individuals with MS, all newly diagnosed in the past decade.
Methods: We established a clinician alert system, linking the SMSR with the Electronic Communication of Surveillance in Scotland (ECOSS). This allows identification of patients within this cohort who had a positive SARS-CoV-2 PCR test. The SMSR was also linked to death records from National Records Scotland.
Results: Of 4702 people with MS, 246 severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) PCR tests were performed, of which 17 were positive. The proportion of positive tests were similar to the general Scotland population (Observed PCR confirmed cases = 17, expected = 17.5, O/E = 0.97, 95% CI: 0.60 – 1.56, p =.90). Between 1 st March – 31 st July 2020 12 individuals on the SMSR died, 5 of which were linked to COVID-19 (1 PCR confirmed, 4 clinical diagnoses without PCR confirmation). This number of COVID-19-related deaths was higher than expected (observed deaths = 5, expected deaths = 1.2, O/E = 4.03, 95% CI = 1.48 – 8.94, p =.01). All COVID-19-related deaths in the SMSR occurred in individuals with advanced disability (Expanded Disability Status Scale ≥7), and no deaths occurred in patients receiving disease modifying therapy (DMT) therapies.
Conclusion: In this nationally comprehensive cohort of MS patients diagnosed in Scotland within the past 10 years, we observed similar rates of PCR-confirmed SARS-CoV-2 infection compared to the general Scottish population, but a small number of excess COVID-19 related deaths. These deaths occurred in individuals with advanced disability who were not receiving DMTs.
| Level 4 |
Background: Health conditions and immune dysfunction associated with trisomy 21 Down syndrome (DS) may impact the clinical course of COVID-19 once infected by SARS-CoV-2.
Methods: The Trisomy 21 Research Society (T21RS) COVID-19 Initiative launched an international survey for clinicians or caregivers/family members on patients with COVID-19 and DS (N=1046). De-identified survey data collected between April and October 2020 were analysed and compared with the UK ISARIC4C survey of hospitalized COVID-19 patients with and without DS. COVID-19 patients with DS from the ISARIC4C survey (ISARIC4C DS cases=100) were matched to a random set of patients without DS (ISARIC4C controls=400) and hospitalized DS cases in the T21RS survey (T21RS DS cases=100) based on age, gender, and ethnicity.
Finding: The mean age in the T21RS survey was 29 years (SD=18), 73% lived with their family. Similar to the general population, the most frequent signs and symptoms of COVID-19 were fever, cough, and shortness of breath. Pain and nausea were reported less frequently (p<0.01), whereas altered consciousness/confusion were reported more frequently (p<0.01). Risk factors for hospitalization and mortality were similar to the general population (age, male gender, diabetes, obesity, dementia) with the addition of congenital heart defects as a risk factor for hospitalization. Mortality rates showed a rapid increase from age 40 and were higher than for controls (T21RS DS versus controls: risk ratio (RR)=3.5 (95%-CI=2.6;4.4), ISARIC4C DS versus controls: RR=2.9 (95%-CI=2.1;3.8)) even after adjusting for known risk factors for COVID-19 mortality.
Interpretation: Leading signs/symptoms of COVID-19 and risk factors for severe disease course are similar to the general population. However, individuals with DS present significantly higher rates of mortality, especially from age 40.
| Level 4 |
Background: People with intellectual and developmental disabilities (IDD) appear to be at greater risk for severe outcomes from COVID-19. The roles of congregate living and skilled nursing care needs in this disparity are unclear.
Objective: To determine the impact of residential setting and level of skilled nursing care on COVID-19 outcomes for people receiving IDD services, compared to those not receiving IDD services.
Methods: Utilizing publicly available California data on COVID-19 outcomes for people receiving IDD services (early May through October 2, 2020), we report outcomes based on seven types of residence, differentiated by number of residents and level of skilled nursing care provided. We compared these results to the larger California published outcomes.
Results: Compared to Californians not receiving IDD services, in general, those receiving IDD services had a 60% lower case rate, but 2.8 times higher case-fatality rate. COVID-19 outcomes varied significantly among Californians receiving IDD services by type of residence and skilled nursing care needs: higher rates of diagnosis in settings with larger number of residents, higher case-fatality and mortality rates in settings that provided 24-h skilled nursing care.
Conclusions: Diagnosis with COVID-19 among Californians receiving IDD services appears to be related to the number of individuals within the residence, while adverse COVID-19 outcomes were associated with level of skilled nursing care. When data is available, future research should examine whether these relationships persist even when controlling for age and pre-existing conditions.
| Level 4 |
Background: People with intellectual and developmental disabilities (IDD) may be at higher risk of severe outcomes from COVID-19.
Objective: To describe COVID-19 outcomes among people with IDD living in residential groups homes in the state of New York and the general population of New York State.
Methods: Data for people with IDD are from a coalition of organizations providing over half of the residential services for the state of New York, and from the New York State Department of Health. Analysis describes COVID-19 case rates, case-fatality, and mortality among people with IDD living in residential group homes and New York State through May 28, 2020.
Results: People with IDD living in residential group homes were at greater risk of severe COVID-19 outcomes: case rates – 7,841 per 100,000 for people with IDD compared to 1,910 for New York State; case-fatality – 15.0% for people with IDD compared to 7.9% for New York State; and mortality rate – 1,175 per 100,000 for people with IDD compared to 151 per 100,000 for New York State. Differences in cases and mortality rate were confirmed across regions of the state, but case-fatality rate was only higher for people with IDD in and around the New York City region.
Conclusions: COVID-19 appears to present a greater risk to people with IDD, especially those living in congregate settings. A full understanding of the severity of this risk will not be possible until US states begin publicly sharing all relevant data they have on COVID-19 outcomes among this population.
| Level 4 |
Importance: Risk factors associated with the severity of coronavirus disease 2019 (COVID-19) in patients with multiple sclerosis (MS) are unknown. Disease-modifying therapies (DMTs) may modify the risk of developing a severe COVID-19 infection, beside identified risk factors such as age and co-occurring medical conditions.
Objective: To describe the clinical characteristics and outcomes in patients with MS and COVID-19 and identify factors associated with COVID-19 severity.
Design, Setting, and Participants: The Covisep registry is a multicentre, retrospective, observational cohort study conducted in MS expert centres and general hospitals and with neurologists collaborating with MS expert centres and members of the Société Francophone de la Sclérose en Plaques. The study included patients with MS presenting with a confirmed or highly suspected diagnosis of COVID-19 between March 1, 2020, and May 21, 2020.
Exposures: COVID-19 diagnosed with a polymerase chain reaction test on a nasopharyngeal swab, thoracic computed tomography, or typical symptoms.
Main Outcomes and Measures: The main outcome was COVID-19 severity assessed on a 7-point ordinal scale (ranging from 1 [not hospitalized with no limitations on activities] to 7 [death]) with a cutoff at 3 (hospitalized and not requiring supplemental oxygen). We collected demographics, neurological history, Expanded Disability Severity Scale score (EDSS; ranging from 0 to 10, with cutoffs at 3 and 6), co-occurring medical conditions, COVID-19 characteristics, and outcomes. Univariate and multivariate logistic regression models were used to estimate the association of collected variables with COVID-19 outcomes.
Results: A total of 347 patients (mean [SD] age, 44.6 [12.8] years, 249 women; mean [SD] disease duration, 13.5 [10.0] years) were analysed. Seventy-three patients (21.0%) had a COVID-19 severity score of 3 or more, and 12 patients (3.5%) died of COVID-19. The median EDSS was 2.0 (range, 0-9.5), and 284 patients (81.8%) were receiving DMT. There was a higher proportion of patients with a COVID-19 severity score of 3 or more among patients with no DMT relative to patients receiving DMTs (46.0% vs 15.5%; P < .001). Multivariate logistic regression models determined that age (odds ratio per 10 years: 1.9 [95% CI, 1.4-2.5]), EDSS (OR for EDSS ≥6, 6.3 [95% CI. 2.8-14.4]), and obesity (OR, 3.0 [95% CI, 1.0-8.7]) were independent risk factors for a COVID-19 severity score of 3 or more (indicating hospitalization or higher severity). The EDSS was associated with the highest variability of COVID-19 severe outcome (R2, 0.2), followed by age (R2, 0.06) and obesity (R2, 0.01).
Conclusions and Relevance: In this registry-based cohort study of patients with MS, age, EDSS, and obesity were independent risk factors for severe COVID-19; there was no association found between DMTs exposure and COVID-19 severity. The identification of these risk factors should provide the rationale for an individual strategy regarding clinical management of patients with MS during the COVID-19 pandemic.
| Level 4 |
Background: It is unknown how the novel Coronavirus SARS-CoV-2, the cause of the current acute respiratory illness COVID-19 pandemic that has infected millions of people, affects people with intellectual and developmental disability (IDD). The aim of this study is to describe how individuals with IDD have been affected in the first 100 days of the COVID-19 pandemic.
Methods: Shortly after the first COVID-19 case was reported in the USA, our organisation, which provides continuous support for over 11 000 individuals with IDD, assembled an outbreak committee composed of senior leaders from across the health care organisation. The committee led the development and deployment of a comprehensive COVID-19 prevention and suppression strategy, utilising current evidence-based practice, while surveilling the global and local situation daily. We implemented enhanced infection control procedures across 2400 homes, which were communicated to our employees using multi-faceted channels including an electronic resource library, mobile and web applications, paper postings in locations, live webinars and direct mail. Using custom-built software applications enabling us to track patient, client and employee cases and exposures, we leveraged current public health recommendations to identify cases and to suppress transmission, which included the use of personal protective equipment. A COVID-19 case was defined as a positive nucleic acid test for SARS-CoV-2 RNA.
Results: In the 100-day period between 20 January 2020 and 30 April 2020, we provided continuous support for 11 540 individuals with IDD. Sixty-four per cent of the individuals were in residential, community settings, and 36% were in intermediate care facilities. The average age of the cohort was 46 ± 12 years, and 60% were male. One hundred twenty-two individuals with IDD were placed in quarantine for exhibiting symptoms and signs of acute infection such as fever or cough. Sixty-six individuals tested positive for SARS-CoV-2, and their average age was 50. The positive individuals were located in 30 different homes (1.3% of total) across 14 states. Fifteen homes have had single cases, and 15 have had more than one case. Fifteen COVID-19-positive individuals were hospitalised. As of 30 April, seven of the individuals hospitalised have been discharged back to home and are recovering. Five remain hospitalised, with three improving and two remaining in intensive care and on mechanical ventilation. There have been three deaths. We found that among COVID-19-positive individuals with IDD, a higher number of chronic medical conditions and male sex were characteristics associated with a greater likelihood of hospitalisation.
Conclusions: In the first 100 days of the COVID-19 outbreak in the USA, we observed that people with IDD living in congregate care settings can benefit from a coordinated approach to infection control, case identification and cohorting, as evidenced by the low relative case rate reported. Male individuals with higher numbers of chronic medical conditions were more likely to be hospitalised, while most younger, less chronically ill individuals recovered spontaneously at home.
| Level 5 |
Background: In view of the emerging coronavirus pandemic, the demand for knowledge about the impact of SARS-CoV-2 on people with Multiple Sclerosis (MS) continues to grow. Patients receiving disease modifying therapy (DMT) for MS have a higher background risk of infection-related health care utilization when compared to the general population. Therefore, there is a need of evidence-based recommendations to reduce the risk of infection and also managing MS patients with SARS-CoV-2.
Case Description: We present three patients with history of Multiple Sclerosis (MS) on DMTs presenting with worsening MS symptoms likely pseudo exacerbation who were diagnosed with COVID-19.
Discussion(s): An extensive review of 7 articles was performed, in addition to a brief review on DMTs use in MS patients with COVID-19. In our cases, all patients were on DMT and severe course of disease was noted in 2 cases. No fatality was observed.
Conclusion(s): This review provides a base on the clinical characteristics, outcomes and the roles of DMTs in MS patients suffering from n-cov-2. Physicians need to be vigilant about considering COVID-19 infection related relapse in the MS patients, especially in this COVID-19 pandemic era and look for pseudo-exacerbation. As most cases are found to have mild course and full recovery on DMTs, further research is needed to formulate evidence-based guidelines. This review will particularly be helpful for the researchers and registries to collect future data on MS and COVID-19.
| Level 5 |
With increasing information available about the epidemiology, pathophysiology, and management of patients affected with severe acute respiratory syndrome corona virus-2 infection, patients with Down syndrome, congenital heart disease, airway obstruction, and pulmonary hypertension present a unique challenge. This case series describes 3 patients with Down syndrome and respiratory failure secondary to coronavirus infection.
| Level 5 |
Nollace et al (2020) Autism and COVID-19: a case series in a neurodevelopmental unit[xvii]
Background: COVID-19 has become pandemic and can impact individuals with autism as well. Here, we report a case series admitted to a neurobehavioral unit dedicated to challenging behaviours in patients with autism.
Method(s): We describe 16 patients (mean age 20.8 years; range 12-43 years; 76% male) with autism hospitalized between March 2020 and mid-April 2020 for challenging behaviours, for which COVID-19 disease has been suspected and who needed both psychiatric and medical care. A close cooperation with the Infectious and Tropical Diseases Department was organized to limit viral spread and training sessions ¾ eg hygiene, clinical COVID-19 monitoring, virus testing ¾ were given to staff members.
Result(s): Most patients had severe autism and severe/moderate intellectual disability. Eleven patients were already in the unit when it was hit by the pandemic, and five were admitted from the community. Based on a virus search via reverse transcriptase polymerase chain reaction (RT-PCR) or serology at the 2-month follow-up, we had 11 confirmed COVID-19 cases. The main COVID-19 symptoms included benign upper respiratory infection signs (N = 9, 81.8%), diarrhoea (N = 7, 63.6%), fatigue (N = 7, 63.6%), and respiratory signs (N = 5, 45.5%), including one patient who needed oxygen therapy. Three patients remained asymptomatic and COVID-19-free (including two under immunosuppressive treatments). Among the symptomatic patients, five showed atypical behaviours that we understood as idiosyncratic manifestations (eg irrepressible licking behaviour). On day 14, only one patient with respiratory dysfunction still had a positive RT-PCR SARS-CoV-2 test.
Conclusion(s): Organizing a COVID+ unit for patients with autism is realistic and requires close collaboration with infectologists. We believe that this initiative should be promoted to limit both the spread of the virus and the ostracism of patients with autism and challenging behaviours.
| Level 5 |
Background: Rapid spread of COVID-19 has affected people with intellectual disability disproportionately. Existing data does not provide enough information to understand factors associated with increased deaths in those with intellectual disability. Establishing who is at high risk is important in developing prevention strategies, given that risk factors or co-occurring medical conditions in people with intellectual disability may be different to those in the general population.
Aims: To identify co-occurring medical conditions, demographic and clinical factors of those individuals with intellectual disability who have died from COVID-19.
Method: An observational descriptive case series looking at deaths because of COVID-19 in people with intellectual disability was conducted. Along with established risk factors observed in the general population, possible specific risk factors and co-occurring medical conditions in people with intellectual disability for deaths related to COVID-19 were examined. Comparisons between mild and moderate-to-profound intellectual disability subcohorts were undertaken.
Results: Data on 66 deaths in individuals with intellectual disability were analysed. This group was younger (mean age 64 years) compared with the age of death in the general population because of COVID-19. High rates of moderate-to-profound intellectual disability (n = 43), epilepsy (n = 29), mental illness (n = 29), dysphagia (n = 23), Down syndrome (n = 20) and dementia (n = 15) were observed.
Conclusions: This is the first study exploring associations between possible risk factors and co-occurring medical conditions found in COVID-19 deaths in people with intellectual disability. Our data provides insight into possible factors for deaths in people with intellectual disability. Some of the factors varied between the mild and moderate-to-profound intellectual disability groups. This highlights an urgent need for further systemic inquiry and study of the possible cumulative impact of these factors and co-occurring medical conditions given the possibility of COVID-19 resurgence.
| Level 5 |
Background: Persons with Down syndrome (DS) are presumed to be at high risk of severe COVID-19, due to immune dysregulation and often compromised cardiopulmonary function. Aim of the present study is to assess epidemiological and clinical characteristics of individuals with DS deceased in Italian hospitals with COVID-19.
Methods: We used a nationwide database of 3,438 patients deceased with RT-PCR-confirmed SARS-CoV-2 infection in Italy (10.4% of all deaths with COVID-19 in the country at the time of analysis). Data on demographics, pre-existing medical conditions and in-hospital complications leading to death were extracted from medical charts obtained from hospitals. Data on individuals with DS deceased with COVID-19 were obtained from this sample.
Results: Sixteen cases of death in individuals with DS (0.5% of all charts analysed) were identified. Acute respiratory distress syndrome occurred in all 16 cases. Compared with individuals without DS, those with DS deceased with COVID-19 were younger (52.3 ± 7.3 vs. 78.1 ± 10.6 years, p < .001) and presented a higher incidence of superinfections (31.2 vs. 13.0%, p = .029). Autoimmune diseases (43.8 vs. 4%, p < .001), obesity (37.5 vs. 11%, p = .009), and dementia (37.5 vs. 16.3%, p = .012) were more prevalent in individuals with DS. ICU admissions was similar in both groups (25 vs. 18.8%, p = .129).; Conclusions: Individuals with DS deceased with COVID-19 are younger than individuals without DS. The burden of co-occurring medical conditions and increased risk of complications (i.e., bacterial superinfections) can influence COVID-19 prognosis in individuals with DS. Specific strategies to prevent and mitigate the effects of COVID-19 in the population with DS are needed.
| Level 6 |
Objectives: To develop a protocol for a scoping review mapping as well as thematically analysing the literature on the effect of, and responses to, the coronavirus disease 2019 (COVID-19) pandemic, focused on people with disabilities with other layers of individual vulnerability or social disadvantage.
Methods: We will search scientific databases (Medline/PubMed, Web of Science, Scopus, AgeLine, PsycINFO, CINAHL, ERIC) and preprint servers (MedRxiv, SocArXiv, PsyArXiv). Google searches, snowballing, and key-informant strategies were also used, including a focus on the grey literature. Peer-reviewed and preprint publications will be covered in 6 languages, and the grey literature in English. Publications will be included if they address individuals with disabilities; the COVID-19 pandemic or subsequent socioeconomic or occupational effects; and individual or social vulnerabilities, including any form of discrimination, marginalization, or social disadvantage. Two independent reviewers will perform eligibility decisions and key data extractions. Beyond mapping the literature, the results will thematically analyse any disproportionate risks people with disabilities and other forms of vulnerability experience in terms of being infected by COVID-19, having severe health consequences, and facing negative socioeconomic effects. Actions taken or recommended to reduce identified inequalities will also be synthesized. Our entire research team, with diverse backgrounds, will be involved in the synthesis.
Conclusions: This review, which we plan to expedite, aims to inform policy makers, health authorities, disability advocates, and other stakeholders regarding the needs and ways to promote equity and disability-inclusive responses to the COVID-19 pandemic and the resultant socioeconomic shockwaves.
| Level 6 |
The severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) pandemic is a challenge for all participants in the healthcare system. At the beginning of the pandemic, many physicians asked themselves what risk their patients, especially those with chronic diseases, were exposed to. We present an overview of all patients with multiple sclerosis (MS) and SARS-CoV-2 infection published in the literature so far. In total, there are publications on 873 SARS-CoV-2 positive MS patients and information on the outcome can be given for 700 patients. With regard to the different disease modifying therapies (DMTs), by far the most cases were described under anti-CD20 treatment (n = 317). The mortality rate of all MS patients was 4% and a further 3% required invasive or non-invasive ventilation. When looking at the severe and fatal cases, it is particularly noticeable that patients without DMTs, with previous cardiovascular diseases, or with a severe degree of dis-ability are at risk. Immunosuppressive therapy itself does not appear to be a substantial risk factor. Rather, it is reasonable to assume that the therapies could be protective, either directly, by mitigating the cytokine storm, or indirectly, by reducing the disease activity of MS.
| Level 6 |
Recently, the COVID19 Open Research Dataset (CORD–19) was published. For researchers on ID such as ourselves, it is of key interest to learn whether this open research dataset may be used to investigate the virus and its consequences for people with an ID.
Methods: From CORD–19, we identified full‐text articles containing terms related to the ID care and applied a text mining technique, specifically the term frequency ¾ inverse document frequency analysis in combination with K ¾means clustering.
Results: Two hundred fifty–nine articles contained one or more of our specified terms related to ID. We were able to cluster these articles related to ID into five clusters on different topics, namely: mental health, viral diseases, diagnoses and treatments, maternal care and paediatrics, and genetics.
Conclusion: The CORD–19 open research dataset consists of valuable information about not only COVID–19 disease but also ID and the relationship between them. We suggest researchers investigate literature‐based discovery approaches on the CORD–19 and develop a new dataset that addresses the intersection of these two fields for further research.
| Level 7 |
We report two cases of Corona Virus Disease-19 (COVID-19) in patients with Down Syndrome (DS) and describe the identification, diagnosis, clinical course and management of the infection. Down Syndrome, which is caused by trisomy 21, is characterized by immune dysregulation, anatomical differences in the upper respiratory tract and higher rate of co-occurring medical conditions. All these risk factors can contribute to more severe clinical presentations of COVID-19 in this population. It is essential to raise awareness of the clinical relevance of SARS-COV-2 infection in DS patients, as well as in other most vulnerable patients, in order to improve their management and treatment and to encourage vaccinating these individuals early, once a vaccination is available.
| Level 7 |
The current COVID–19 pandemic is a pressing world crisis and people with intellectual disabilities (IDs) are vulnerable due to disparity in healthcare provision and physical and mental health multimorbidity. The aim of this study is to present guidelines for the care and treatment of people with IDs during the COVID–19 pandemic for both community teams providing care to people with IDs and inpatient psychiatric settings. The guidelines cover specific issues associated with hospital passports, individual COVID–19 care plans, the important role of families and carers, capacity to make decisions, issues associated with social distancing, ceiling of care/treatment escalation plans, mental health and challenging behaviour, and caring for someone suspected of contracting or who has contracted SARS–CoV–2 within community or inpatient psychiatric settings. We have proposed that the included conditions recommended by Public Health England to categorize someone as high risk of severe illness due to COVID‐19 should also include mental health and challenging behaviour. There are specific issues associated with providing care to people with IDs and appropriate action must be taken by care providers to ensure that disparity of healthcare is addressed during the COVID–19 pandemic. We recognize that our guidance is focused on healthcare delivery in England and invite others to augment our guidance for use in other jurisdictions.
| Level 7 |
Down Syndrome is characterised by the coexistence of obesity and cardiovascular and respiratory anomalies, which are risk factors for COVID-19. A total of 55 children were admitted to the paediatric ward in Bergamo, between February and May 2020 for COVID-19. The authors describe the cases of two children with Down Syndrome and a confirmed COVID-19 diagnosis who had a severe course. In addition, both cases involved one or more co-occurring medical conditions, including cardiovascular anomalies, obesity, and/or obstructive sleep apnoea. These observations indicate that children with Down Syndrome are at risk for severe COVID-19 disease course.
| Level 7 |
Kleiman et al (2020) COVID-19 infection in a patient with Fragile-X Syndrome[xxvi]
In this report, the authors explore the case of a patient with Fragile-X Syndrome (FXS) who developed pneumonia due to COVID-19. FXS is an inherited cause of intellectual disability with potential neurologic and physiologic sequelae. In this narrative, we aim to describe how FXS may potentially play a role in the clinical course of patients with COVID-19.
| Level 7 |
The article offers information on the harmful impact of COVID-19 on deaf older adults and older adults with hearing loss in the U.S. It mentions that US Centers for Disease Control and Prevention (CDC) has identified older adults as particularly vulnerable to COVID-19 pandemic. It discusses the developing innovative and effective interventions to reduce adverse COVID-19 outcomes.
| Level 7 |
Peate (2020) [Editorial] Inequality: it’s life and death[xxviii]
This editorial discusses findings from a review undertaken by Public Health England (PHE). COVID-19 deaths among those with learning disabilities were more widely spread across age groups and there were far greater mortality rates among younger adults. People aged 18-34 years, when compared with the general population, were 30 times more likely to die with the virus.
| Level 7 |
Infection with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), leading to Coronavirus disease 2019 (COVID-19), is not always confined to the respiratory tract, while patients with can develop neurological manifestations. The patients with multiple sclerosis (MS) pose challenges in this pandemic situation, because of the immunosuppressive medications they get and the fact that viral infections may contribute to MS exacerbation and relapses as an environmental factor in genetically predisposed individuals. Herein, possible consequences of COVID-19 which may carry for the MS patients and the underlying mechanisms of its impact are discussed.
| Level 8: UNCLASSIFIED |
Callea et al (2020) COVID-19 and Down Syndrome[xxx]
Surprisingly, to date no single PubMed study has dealt with the potential impact of the COVID‐19 on Down Syndrome. As COVID‐19 presents as an acute severe respiratory syndrome and Down Syndrome is by far the most frequent chromosomal disease with the highest susceptibility to develop respiratory infections and complications, it seems timely to focus on this syndrome during the ongoing pandemic.
| Level 8: UNCLASSIFIED |
Steinman (2020) COVID-19 and autism[xxxi]
The current pandemic of COVID-19 has created a paradigm for possibly gaining greater insight in two conditions: Studies since the beginning of this century have supported the view that IGF-1 deficiency in the neonate defines the basis of autism. As a result, it appears that interleukin-6 in corona virus-based infections causes reduced defences because of suppressed IGF-1, especially in older patients. This may also portend an increase of autism in the offspring of gravidas currently affected severely by COVID-19.
Other Sources of Evidence
ASHA Leader (2021) [News] High COVID-19 mortality rate seen in special needs population[xxxii]
The news piece reports on the findings of an analysis which revealed a high COVID-19 mortality rate among people with intellectual disabilities and developmental disorders.
European Disability Forum (2020) Impact of COVID-19 on persons with disabilities: European leaders must act now: extract from the Human Rights Report 2020[xxxiii]
This extract from the Human Rights Report 2020 gives an overview of the impact of the COVID-19 pandemic on persons with disabilities in Europe and draws specific recommendations for the EU and European countries. Factors increasing the risk of persons with disabilities to COVID-19 infection include medical conditions and unmet needs for healthcare, barriers in access to healthcare, older age, and institutionalization.
IDS – TILDA (2020) Understanding the impact of COVID-19 on the health and well-being of older adults with an intellectual disability in Ireland: Findings from wave 4 of The Intellectual Disability Supplement to The Irish Longitudinal Study on Ageing (IDS-TILDA)[xxxiv]
A telephone survey was conducted to investigate the impact of COVID-19 and the associated lockdown on older adults with intellectual disability.
- 710 people over 40 years of age with intellectual disabilities (ID) completed the COVID-19 survey.
- Two-thirds (62.4%) of the older adults with ID surveyed were tested for COVID-19, with only 11 people testing positive, and no reported deaths. This gives an overall infection rate of 2.5%.
- There was a high rate of reported pre-existing conditions which are associated with poorer outcomes for COVID-19. 371 (52%) participants having a history of cardiovascular disease and 365 (66%) participants having a history of overweight/obesity.
- There was also a high prevalence of certain psychiatric/neurological conditions: 209 (29.5%) participants had a history of epilepsy, and 29 (4.1%) participants had a history of dementia. A further 61 (8.6%) participants had a history of lung disease/asthma, 68 (9.6%) had a history of diabetes, and 380 (53.5%) had a history of emotional, nervous or psychiatric disorder.
Irish Human Rights and Equality Commission (2020) The impact of COVID-19 on people with disabilities: submission by the Irish Human Rights and Equality Commission to the Oireachtas Special Committee on COVID-19 Response: June 2020[xxxv]
Data published by the Central Statistics Office on 5 June 2020 showed that the rate of COVID-19 infection per 100,000 persons was somewhat higher for people with disabilities (530) that for those without disabilities (499). However, the COVID-19 mortality rate was 41 per 100,000 for people with disabilities compared to 23 per 100,000 without a disability. The CSO does not provide any analysis of these comparative figures. However, it is clear that these significantly higher death rates for people with disabilities are related to the higher rates identified for vulnerable people living in long-term care settings including nursing homes and more generally to the higher risk faced by older people who have a greater likelihood of being disabled.
As of 4 June 2020, some 650 people in disability services had been identified as having COVID-19symptoms, and 430 of these had their diagnosis confirmed in a lab. Among the cases, 57% were staff and 43% were residents, while a total of 14 people in disability services have died from the virus.
The Department of Health and Social Care, with the support of the Chief Medical Officer for England, commissioned Public Health England (PHE) to review the available data on the deaths of people with learning disabilities in England from the start of the COVID-19 Pandemic to 5 June 2020. The review examined:
- deaths from COVID-19 of people with learning disabilities;
- factors impacting the risk of death from COVID-19 of people with learning disabilities; and
- deaths in care settings of people with learning disabilities.
Based on the deaths reported to the Learning Disabilities Mortality Review, the COVID-19 death rate for people with learning disabilities was 240 deaths per 100,000 adults with learning disabilities. This is 2.3 times the rate in the general population for the same period. However, after adjusting for under-reporting the estimated rate was 369 per 100,000 adults, which is 3.6 times the rate in the general population. Most deaths (82%) of people with learning disabilities from COVID-19 happened in hospital. This was higher than the proportion of all deaths in previous years (60%) and higher than the proportion of COVID-19 deaths in the general population (63%). COVID-19 accounted for 54% of deaths of adults with learning disabilities in residential care in the review period, slightly less than for people with learning disabilities generally, but still much more than in the general population.
UK Office for National Statistics (2021) Updated estimates of coronavirus (COVID-19) related deaths by disability status, England: 24 January to 20 November 2020[xxxvii]
Between 24 January and 20 November 2020 in England, the risk of death involving COVID-19 was 3.1 times greater for more-disabled men and 1.9 times greater for less-disabled men, compared with non-disabled men; among women, the risk of death was 3.5 times greater for more-disabled women and 2.0 times greater for less-disabled women, compared with non-disabled women.
After using statistical models to adjust for personal and household characteristics, including residence type, geography, demographic and socio-economic factors, and pre-existing health conditions, a smaller but statistically significantly raised risk of death remained unexplained for more-disabled and less-disabled women (1.4 and 1.2 times respectively) and more-disabled men (1.1 times) but not for less-disabled men.
Looking at people with a medically diagnosed learning disability, the risk of death involving COVID-19 was 3.7 times greater for both men and women compared with people who did not have a learning disability; after using statistical models to adjust for a range of factors, a raised risk of 1.7 times remained unexplained for both sexes.
All the socio-economic and geographical circumstances and pre-existing health conditions considered made some difference to the risk for people with learning disabilities, but the largest effect was associated with living in a care home or other communal establishment.
Patterns in excess COVID-19 mortality risk experienced by disabled people remained largely unchanged between the first and second waves of the pandemic.
[i] Health Protection Surveillance Centre (2020) Guidance for COVID-19 in Social Care Group Homes and Residential Care Services – Disabilities. https://www.hpsc.ie/a-z/respiratory/coronavirus/novelcoronavirus/guidance/disabilityservicesguidance/. [Accessed 26 February 2021]
[ii] World Health Organization (2020) Disability considerations during the COVID-19 outbreak. https://apps.who.int/iris/handle/10665/332015 [Accessed 1 March 2021].
[iii] CDC (2021) People with disabilities. https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/people-with-disabilities.html. [Accessed 1 March 2021].
[iv] Centers for Disease Control and Prevention (2021) People with developmental and behavioral disorders. https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/people-with-developmental-behavioral-disabilities.html. [Accessed 1 March 2021].
[v] BMJ Best Practice (2021) Management of coexisting conditions in the context of COVID-19. https://bestpractice.bmj.com/topics/en-gb/3000190#referencePop340. [Accessed 26 February 2021]
[vi] UpToDate (2021) Coronavirus Disease 2019 (COVID-19): Clinical manifestations and diagnosis in children. https://www.uptodate.com/contents/coronavirus-disease-2019-COVID-19-clinical-manifestations-and-diagnosis-in-children. [Accessed 26 February 2021]
[vii] Chaudhry, F., Bulka, H., Rathnam, A. S., Said, O. M., Lin, J., Lorigan, H., Bernitsas, E., Rube, J., Korzeniewski, S. J., Memon, A. B., Levy, P. D., Schultz, L., Javed, A., Lisak, R., & Cerghet, M. (2020). COVID-19 in multiple sclerosis patients and risk factors for severe infection. Journal of the neurological sciences, 418, 117147. https://doi.org/10.1016/j.jns.2020.117147
[viii] Cuypers, M., Schalk, B., Koks-Leensen, M., Nägele, M. E., Bakker-van Gijssel, E. J., Naaldenberg, J., & Leusink, G. L. (2020). Mortality of people with intellectual disabilities during the 2017/2018 influenza epidemic in the Netherlands: potential implications for the COVID-19 pandemic. Journal of intellectual disability research : JIDR, 64(7), 482–488. https://doi.org/10.1111/jir.12739
[ix] Fernandes, P. M., O’Neill, M., Kearns, P., Pizzo, S., Watters, C., Baird, S., MacDougall, N., & Hunt, D. (2020). Impact of the first COVID-19 pandemic wave on the Scottish Multiple Sclerosis Register population. Wellcome open research, 5, 276. https://doi.org/10.12688/wellcomeopenres.16349.1
[x] Hüls, A., Costa, A., Dierssen, M., Baksh, R. A., Bargagna, S., Baumer, N. T., Brandão, A. C., Carfi, A., Carmona-Iragui, M., Chicoine, B. A., Ghosh, S., Lakhanpaul, M., Manso, C., Mayer, M. A., Del Carmen Ortega, M., de Asua, D. R., Rebillat, A. S., Russell, L. A., Sgandurra, G., Valentini, D., … Strydom, A. (2020). An international survey on the impact of COVID-19 in individuals with Down syndrome. medRxiv : the preprint server for health sciences, 2020.11.03.20225359. https://doi.org/10.1101/2020.11.03.20225359
[xi] Landes, S. D., Turk, M. A., & Wong, A. (2020). COVID-19 outcomes among people with intellectual and developmental disability in California: The importance of type of residence and skilled nursing care needs. Disability and health journal, 101051. Advance online publication. https://doi.org/10.1016/j.dhjo.2020.101051
[xii] Landes, S. D., Turk, M. A., Formica, M. K., McDonald, K. E., & Stevens, J. D. (2020). COVID-19 outcomes among people with intellectual and developmental disability living in residential group homes in New York State. Disability and health journal, 13(4), 100969. https://doi.org/10.1016/j.dhjo.2020.100969
[xiii] Louapre, C., Collongues, N., Stankoff, B., Giannesini, C., Papeix, C., Bensa, C., Deschamps, R., Créange, A., Wahab, A., Pelletier, J., Heinzlef, O., Labauge, P., Guilloton, L., Ahle, G., Goudot, M., Bigaut, K., Laplaud, D. A., Vukusic, S., Lubetzki, C., De Sèze, J., … Videt, D. (2020). Clinical Characteristics and Outcomes in Patients With Coronavirus Disease 2019 and Multiple Sclerosis. JAMA neurology, 77(9), 1079–1088. https://doi.org/10.1001/jamaneurol.2020.2581
[xiv] Mills, W. R., Sender, S., Lichtefeld, J., Romano, N., Reynolds, K., Price, M., Phipps, J., White, L., Howard, S., Poltavski, D., & Barnes, R. (2020). Supporting individuals with intellectual and developmental disability during the first 100 days of the COVID-19 outbreak in the USA. Journal of intellectual disability research : JIDR, 64(7), 489–496. https://doi.org/10.1111/jir.12740
[xv] Kataria, S., Tandon, M., Melnic, V., & Sriwastava, S. (2020). A case series and literature review of multiple sclerosis and COVID-19: Clinical characteristics, outcomes and a brief review of immunotherapies. eNeurologicalSci, 21, 100287. https://doi.org/10.1016/j.ensci.2020.100287
[xvi] Krishnan, U. S., Krishnan, S. S., Jain, S., Chavolla-Calderon, M. B., Lewis, M., Chung, W. K., & Rosenzweig, E. B. (2020). SARS-CoV-2 Infection in Patients with Down Syndrome, Congenital Heart Disease, and Pulmonary Hypertension: Is Down Syndrome a Risk Factor?. The Journal of pediatrics, 225, 246–248. https://doi.org/10.1016/j.jpeds.2020.06.076
[xvii] Nollace, L., Cravero, C., Abbou, A., Mazda-Walter, B., Bleibtreu, A., Pereirra, N., Sainte-Marie, M., Cohen, D., & Giannitelli, M. (2020). Autism and COVID-19: A Case Series in a Neurodevelopmental Unit. Journal of clinical medicine, 9(9), 2937. https://doi.org/10.3390/jcm9092937
[xviii] Perera, B., Laugharne, R., Henley, W., Zabel, A., Lamb, K., Branford, D., Courtanay, K., Alexander, R., Purandare, K., Wijeratne, A., Radhakrishnan, V., McNamara, E., Daureeawoo, Y., Sawhney, I., Scheepers, M., Taylor, G., & Shankar, R. (2020). COVID-19 deaths in people with intellectual disability in the UK and Ireland: descriptive study. BJPsych open, 6(6), e123. https://doi.org/10.1192/bjo.2020.102
[xix] Villani, E. R., Carfì, A., Di Paola, A., Palmieri, L., Donfrancesco, C., Lo Noce, C., Taruscio, D., Meli, P., Salerno, P., Kodra, Y., Pricci, F., Tamburo de Bella, M., Floridia, M., Onder, G., & Italian National Institute of Health COVID-19 Mortality Group (2020). Clinical characteristics of individuals with Down syndrome deceased with COVID-19 in Italy-A case series. American journal of medical genetics. Part A, 182(12), 2964–2970. https://doi.org/10.1002/ajmg.a.61867
[xx] Jesus, T. S., Kamalakannan, S., Bhattacharjya, S., Bogdanova, Y., Arango-Lasprilla, J. C., Bentley, J., Gibson, B. E., Papadimitriou, C., & Refugee Empowerment Task Force, International Networking Group of the American Congress of Rehabilitation Medicine (2020). People with Disabilities and Other Forms of Vulnerability to the COVID-19 Pandemic: Study Protocol for a Scoping Review and Thematic Analysis. Archives of rehabilitation research and clinical translation, 2(4), 100079. https://doi.org/10.1016/j.arrct.2020.100079
[xxi] Möhn, N., Konen, F. F., Pul, R., Kleinschnitz, C., Prüss, H., Witte, T., Stangel, M., & Skripuletz, T. (2020). Experience in Multiple Sclerosis Patients with COVID-19 and Disease-Modifying Therapies: A Review of 873 Published Cases. Journal of clinical medicine, 9(12), 4067. https://doi.org/10.3390/jcm9124067
[xxii] Tummers, J., Catal, C., Tobi, H., Tekinerdogan, B., & Leusink, G. (2020). Coronaviruses and people with intellectual disability: an exploratory data analysis. Journal of intellectual disability research : JIDR, 64(7), 475–481. https://doi.org/10.1111/jir.12730
[xxiii] Vita, S., Di Bari, V., Corpolongo, A., Goletti, D., Espinosa, J., Petracca, S., Palmieri, F., Nicastri, E., & INMI COVID-19 study groups (2021). Down Syndrome patients with COVID-19 pneumonia: A high-risk category for unfavourable outcome. International journal of infectious diseases : IJID : official publication of the International Society for Infectious Diseases, 103, 607–610. https://doi.org/10.1016/j.ijid.2020.11.188
[xxiv] Alexander, R., Ravi, A., Barclay, H., Sawhney, I., Chester, V., Malcolm, V., Brolly, K., Mukherji, K., Zia, A., Tharian, R., Howell, A., Lane, T., Cooper, V., & Langdon, P. E. (2020). Guidance for the Treatment and Management of COVID-19 Among People with Intellectual Disabilities. Journal of policy and practice in intellectual disabilities, 10.1111/jppi.12352. Advance online publication. https://doi.org/10.1111/jppi.12352
[xxv] Kantar, A., Mazza, A., Bonanomi, E., Odoni, M., Seminara, M., Verde, I. D., Lovati, C., Bolognini, S., & D’Antiga, L. (2020). COVID-19 and children with Down syndrome: is there any real reason to worry? Two case reports with severe course. BMC pediatrics, 20(1), 561. https://doi.org/10.1186/s12887-020-02471-5
[xxvi] Kleiman, J. D., Veerapaneni, K., Escovar, J., & Orsini, J. (2020). COVID-19 Infection in a Patient With Fragile-X Syndrome. Cureus, 12(10), e11266. https://doi.org/10.7759/cureus.11266
[xxvii] Park J. (2020). Unraveling the Invisible but Harmful Impact of COVID-19 on Deaf Older Adults and Older Adults with Hearing Loss. Journal of gerontological social work, 63(6-7), 598–601. https://doi.org/10.1080/01634372.2020.1799282
[xxviii] Peate I. (2020). Inequality: it’s life and death. British journal of nursing (Mark Allen Publishing), 29(22), 1305. https://doi.org/10.12968/bjon.2020.29.22.1305
[xxix] Sadeghmousavi, S., & Rezaei, N. (2020). COVID-19 and Multiple Sclerosis: Predisposition and Precautions in Treatment. SN comprehensive clinical medicine, 1–6. Advance online publication. https://doi.org/10.1007/s42399-020-00504-9
[xxx] Callea, M., Cammarata-Scalisi, F., Galeotti, A., Villani, A., & Valentini, D. (2020). COVID-19 and Down syndrome. Acta paediatrica (Oslo, Norway : 1992), 109(9), 1901–1902. https://doi.org/10.1111/apa.15409
[xxxi] Steinman G. (2020). COVID-19 and autism. Medical hypotheses, 142, 109797. https://doi.org/10.1016/j.mehy.2020.109797
[xxxii] News (2021). ASHA Leader https://leader.pubs.asha.org/do/10.1044/leader.NIB1.26012021.14/full/. [Accessed 26 February 2021]
[xxxiii] European Disability Forum (2020) Impact of COVID-19 on persons with disabilities: European leaders must act now: extract from the Human Rights Report 2020. https://www.edf-feph.org/content/uploads/2021/01/Final-final-Human-Rights-Published.pdf [Accessed 1 March 2021].
[xxxiv] IDS – TILDA (2020) Understanding the impact of COVID-19 on the health and well-being of older adults with an intellectual disability in Ireland: Findings from wave 4 of The Intellectual Disability Supplement to The Irish Longitudinal Study on Ageing (IDS-TILDA). https://idstilda.tcd.ie/assets/docs/wave4idstildareport.pdf. [Accessed 1 March 2021].
[xxxv] Irish Human Rights and Equality Commission (2020) The Impact of COVID-19 on people with disabilities: submission by the Irish Human Rights and Equality Commission to the Oireachtas Special Committee on COVID-19 Response: June 2020. https://www.ihrec.ie/app/uploads/2020/07/IHREC-Submission-The-Impact-of-COVID-19-on-People-with-Disabilites.pdf. [Accessed 1 March 2021].
[xxxvi] Public Health England (2020) Research and analysis: COVID-19 deaths of people identified as having learning disabilities: summary
https://www.gov.uk/government/publications/COVID-19-deaths-of-people-with-learning-disabilities/COVID-19-deaths-of-people-identified-as-having-learning-disabilities-summary [Accessed 26 February 2021]
[xxxvii] UK Office for National Statistics (2021) Updated estimates of coronavirus (COVID-19) related deaths by disability status, England: 24 January to 20 November 2020. https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/articles/coronavirusCOVID19relateddeathsbydisabilitystatusenglandandwales/24januaryto20november2020#overview-of-COVID-19-related-deaths-by-disability-status. [Accessed 1 March 2021].
Produced by the members of the National Health Library and Knowledge Service Evidence Team†. Current as at 30 October 2020. This evidence summary collates the best available evidence at the time of writing and does not replace clinical judgement or guidance. Emerging literature or subsequent developments in respect of COVID-19 may require amendment to the information or sources listed in the document. Although all reasonable care has been taken in the compilation of content, the National Health Library and Knowledge Service Evidence Team makes no representations or warranties expressed or implied as to the accuracy or suitability of the information or sources listed in the document. This evidence summary is the property of the National Health Library and Knowledge Service and subsequent re-use or distribution in whole or in part should include acknowledgement of the service.
Margaret Morgan, Librarian, Midland Regional Hospital, Mullingar [Author]; Linda Halton, Librarian, Our Lady’s Hospital, Navan [Author/Editor]; Brendan Leen, Area Library Manager, HSE [Editor]

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.