
What is the burden of disease from COVID-19 in 5-11-year-old children?
Download Full Summary of Evidence (PDF)
Main Points
Epidemiology
- The incidence of SARS-CoV-2 infection is similar in children and adults.
- The number of laboratory-confirmed cases of SARS-CoV-2 infection in children reported is likely underestimated given the high proportion of mild and asymptomatic cases in which testing may not be performed.
Severity of Illness
- COVID-19 can cause severe illness in children and adolescents, and may require hospitalisation and ICU support.
- Hospitalisation rates are similar to pre-pandemic influenza-associated hospitalisation rates. Severity is comparable among children hospitalised with influenza and COVID-19.
- Hospitalisation rates increased across all age-groups with the Delta variant.
- Risk factors for severe disease in children include comorbidities such as diabetes mellitus and obesity.
Transmission
- Children of all ages can transmit SARS-CoV-2 to others, but the relative transmissibility of SARS-CoV-2 by children in various age groups is uncertain. Infected children shed SARS-CoV-2 virus with nasopharyngeal viral loads comparable to or higher than those in adults.
- Older children and adolescents transmit SARS-CoV-2 effectively in household and community settings.
- Limited evidence suggests that transmission by preadolescent children occurs but may be uncommon in educational or child care settings. Transmission by presymptomatic children and adolescents also may be uncommon in educational settings when effective case-contact testing and epidemic control strategies are implemented.
- Data from the National Centre for Immunisation Research and Surveillance in Australia19 suggest that the rate of transmission of the SARS-CoV-2 Delta variant in both schools and early childhood education services as well as in households was around 5 times higher than seen with the original strain of the COVID-19 virus.
Multisystem Inflammatory Syndrome in Children (MIS-C)
- Pediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2 (PIMS-TS) or multisystem inflammatory syndrome in children (MIS-C) is a relatively rare complication of COVID-19 in children, occurring in <1% of children with confirmed SARS-CoV-2 infection.
- PIMS-TS/MIS-C is characterized by fever, gastrointestinal and cardiocirculatory manifestations, and increased inflammatory biomarkers. Nevertheless, Hoste et al22 report that 50.3% also present with respiratory symptoms, and that 56.3% present with shock. The majority of the patients need ICU support, including extracorporal membrane oxygenation.
- Despite severe disease, mortality is low (1.9%).
- A predominance of males and non-White ethnicity among the cases is present.
‘Long’ COVID-19
- Miller et al32 estimate the prevalence of persistent symptoms lasting ≥4 weeks as 1.0% in the 2-11-year-old age group. The median duration of symptoms for children aged ≤17 years is 46 days (IQR 32-188).
- Persistent symptom prevalence is higher in girls, teenagers and children with long-term conditions.
- Persistent symptoms include fatigue, muscle and joint pain, headache, insomnia, respiratory problems and palpitations.
- Children with asymptomatic or paucisymptomatic COVID‐19 are among those who have developed chronic, persisting symptoms.
Comorbidities
- Number of comorbid conditions is associated with increased odds of admission to critical care and death from COVID-19.
- Children with obesity and asthma in particular are at increased risk for critical care admission and/or need for respiratory support.
Collateral Health Impacts
- Pooled estimates obtained in the first year of the COVID-19 pandemic suggest that 1 in 4 young people age ≤18 years globally are experiencing clinically elevated depression symptoms, while 1 in 5 young people age ≤18 years are experiencing clinically elevated anxiety symptoms. These pooled estimates have increased over time and are double pre-pandemic estimates.
- Several studies have reported increased levels of pediatric obesity due to the pandemic.
Summary of Evidence
EPIDEMIOLOGY AND SEVERITY OF ILLNESS
The incidence of SARS-CoV-2 infection in children is similar to that in adults4. In surveillance data from various countries children typically account for up to 22% of laboratory-confirmed cases4. Dawood et al12 report site-adjusted incidence rates per 1000 person-weeks of 6.3 (95% CI, 3.6-11.0) for children 0 to 4 years, 4.4 (95% CI, 2.5-7.5) for children 5 to 11 years, 6.0 (95% CI, 3.0-11.7) for children 12 to 17 years, and 5.1 (95% CI, 3.3-7.8) for adults (≥18 years).
In the United States, the Centers for Disease Control and Prevention (CDC) report that incidence rates among persons aged 0–4, 5–11, and 12–17 years in June 2021 were 1.7, 1.9 and 2.9 cases per 100,000 persons, respectively, and increased to 16.2, 28.5, and 32.7 per 100,000 persons in August 2021, after Delta had become the predominant circulating variant2. Among persons aged 0-17 years during the period August 14-27, 2021, COVID-19-related ED visits and hospital admissions in the quartile of states with the lowest vaccination coverage were 3.4 and 3.7 times that of the quartile of states with the highest vaccination coverage, respectively2.
CDC caution that COVID-19 can cause severe illness in children and adolescents, and may require hospitalisation and Intensive Care Unit (ICU) support1-2; and that between March 2020 and August 2021, cumulative COVID-19 associated hospitalisation for all children aged 0-17 was 49.7/100,000 (69.2 in 0-4 years, 24 in 5-11 years, 63.7 in 12-17 years). Hospitalisation rates increased across all age-groups with the Delta variant: the weekly hospitalisation rate per 100,000 children and adolescents during the week ending 14 August 2021 was almost 5 times that of the week ending 26 June 2021. Among all hospitalised children, the proportions with severe disease after Delta became predominant were similar to those earlier in the pandemic.
Children aged 5–11 years are at risk of severe illness from COVID-19, and the CDC5 reports that, as of November 2021, there have been more than 8,300 hospitalisations of children in this age group in the United States. Hospitalisation rates are 3 times higher for non-Hispanic Black, non-Hispanic American Indian or Native Alaskan, and Hispanic children compared with non-Hispanic White children. Hospitalisation rates are similar to pre-pandemic influenza-associated hospitalisation rates. Disease severity was comparable among children hospitalised with influenza and COVID-19. Approximately 1/3 of hospitalised children aged 5–11 years require ICU admission5. At least 94 COVID-19-associated deaths occurred in children aged 5–11 years in the United States in the period January 2020 to October 20215.
Graff et al13 report that comorbidities (including immunocompromise (aOR 3.5, 1.5–8.1), gastrointestinal conditions (aOR 2.7, 1.3–5.7), diabetes (aOR 6.6, 1.1–39.8), and asthma (aOR 2.2, 1.1–4.5), were predictors for hospital admission; and that asthma and gastrointestinal conditions were also predictors for respiratory support.
Woodruff et al7 report that approximately 30% of 3106 hospitalised children in 14 US states between March 2020 and May 2021 had severe COVID-19; and that 0.5% died during hospitalisation. Among hospitalised children aged 2 to 17 years, feeding tube dependence (adjusted risk ratio (aRR): 2.0; 95% CI: 1.5‒2.5), diabetes mellitus (aRR: 1.9; 95% CI: 1.6‒2.3) and obesity (aRR: 1.2; 95% CI: 1.0‒1.4) were associated with severe COVID-19. Severe COVID-19 occurred among 12.0 per 100,000 children overall and was highest among infants, Hispanic children, and non-Hispanic Black children.
Molteni et al9 report that among 694 (276 younger [5-11 years], 418 older [12-17 years]) symptomatic children who tested positive for SARS-CoV-2 with Alpha infection and 706 (227 younger and 479 older) children with Delta infection in Britain, median illness duration was short with either variant. Illness duration in 5-11 year olds was four (IQR 2–8) days with Alpha and four (IQR 2–7.5) days with Delta infection. The most prevalent symptoms were common to both variants: rhinorrhoea, headache and fatigue. The median number of symptoms in 5-11 year olds over the first 28 days was slightly greater with Delta (4, IQR: 2–7) compared with Alpha infection (3, IQR: 2–5). The odds of several symptoms were higher with Delta than Alpha infection, including headache and fever. Few children presented to hospital, and long illness duration was uncommon with either variant. Illness had resolved by 28 days in 274 [99.3%] of 276 younger children with Alpha infection and in 224 [98.7%] of 227 younger children with Delta infection.
Preston et al11 observed an increased association of severe COVID-19 in patients with one or more chronic conditions vs. those with none in children aged 6-11 years vs. those aged 12-18 years (AORs1.53; 95% CI, 1.04-2.23).
TRANSMISSION
Children of all ages can transmit SARS-CoV-2 to others, but the relative transmissibility of SARS-CoV-2 by children in various age groups is uncertain, given the varying contributions of biologic, host, and environmental factors. Older children and adolescents transmit SARS-CoV-2 effectively in household and community settings. Infected children shed SARS-CoV-2 virus with nasopharyngeal viral loads comparable to or higher than those in adults18. Transmission from children to household contacts occurs, although the relative frequency of transmission from young children compared with other age groups is uncertain18. Limited evidence suggests that transmission by preadolescent children occurs but is uncommon in educational or child care settings, particularly if the class size is small, other public health measures are strictly followed, and community transmission is low, although findings are inconsistent. Transmission by presymptomatic children and adolescents also appears to be uncommon in educational settings when effective case-contact testing and epidemic control strategies (eg, universal use of well-fitted masks, physical distancing, improved ventilation) are implemented18. Although there is little information about transmission of SARS-CoV-2 by truly asymptomatic (as opposed to presymptomatic) children, transmission from children with confirmed asymptomatic SARS-CoV-2 to household contacts has been reported18.
Irfan et al16 report that compared to adults, children aged 0-19 years showed comparable national (RR = 0.87, 95% CI = 0.71-1.060) and subnational (RR = 0.81, 95% CI = 0.66-1.01) prevalence in population-screening studies, and lower odds of infection in community/household contact-tracing studies (OR = 0.62, 95% CI = 0.46-0.84). In educational-settings, children attending daycare/preschools (OR = 0.53, 95% CI = 0.38-0.72) were observed to be at lower-risk when compared to adults, with odds of infection among primary (OR = 0.85, 95% CI = 0.55-1.31) and high-schoolers (OR = 1.30, 95% CI = 0.71-2.38) comparable to adults. Overall, children and adolescents had lower odds of infection in educational-settings compared to community and household clusters.
There is weak evidence that children and adolescents play a lesser role than adults in transmission of SARS-CoV-2 at a population level. Paul et al20 suggest that younger children may be more likely to transmit SARS-CoV-2 infection compared with older children, and the highest odds of transmission was observed for children aged 0 to 3 years.
In Australia, the National Centre for Immunisation Research and Surveillance19 found that the rate of transmission of the SARS-CoV-2 Delta variant in both schools and early childhood education services as well as in households was around 5 times higher than seen in educational settings and households in this study in 2020 with the original strain of the COVID-19 virus.
MULTISYSTEM INFLAMMATORY SYNDROME IN CHILDREN (MIS-C)
While the incidence of MIS-C is uncertain, it appears to be a relatively rare complication of COVID-19 in children, occurring in <1% of children with confirmed SARS-CoV-2 infection23.
Hoste et al22 report that pediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2 (PIMS-TS) or multisystem inflammatory syndrome in children (MIS-C) presents at a median age of 8 years. A predominance of males (58.9%) and ethnic minorities (37.0% Black) among the cases is present. Apart from obesity (25.3%), comorbidities are rare. PIMS-TS/MIS(-C) is characterized by fever (99.4%), gastrointestinal (85.6%) and cardiocirculatory manifestations (79.3%), and increased inflammatory biomarkers. Nevertheless, 50.3% present respiratory symptoms as well. Over half of patients (56.3%) present with shock. The majority of the patients (73.3%) need intensive care treatment, including extracorporal membrane oxygenation (ECMO) in 3.8%. Despite severe disease, mortality is low (1.9%).
Flood et al24 found that across all age groups included in their surveillance report, males were over-represented (60%), 19% had co-morbidities, 13.4% were overweight and 5-9-year-olds accounted for 30% (n=80) of cases. Dawood et al25 also report that across all age groups, having one or more underlying medical conditions was associated with increased risk of death from MIS-C (aOR, 2.8; 95% CI, 1.4–5.9). The 6-11-year-old age group had a non-statistically significant lower risk of death from MIS-C compared with all other child age groups.
Estimates for MIS-C population-based incidence and incidence among persons with SARS-CoV-2 infection put forward by Payne et al26 suggest that incidence was highest among children aged 5 years or younger (4.9 [95% CI, 3.7-6.6] children per 1 000 000 person-months) and children aged 6 to 10 years (6.3 [95% CI, 4.8-8.3] children per 1 000 000 person-months).
Feldstein et al29 identified patterns of clinical presentation and organ system involvement among children and adolescents with MIS-C compared with those with severe COVID-19. Compared with patients with severe COVID-19, patients with MIS-C were more likely to be 6 to 12 years old (aRR, 1.51 [95% CI, 1.33-1.72] vs 0-5 years), have cardiorespiratory involvement (aRR, 2.99 [95% CI, 2.55-3.50] vs. respiratory involvement), cardiovascular without respiratory involvement (aRR, 2.49 [95% CI, 2.05-3.02] vs. respiratory involvement), and mucocutaneous without cardiorespiratory involvement (aRR, 2.29 [95% CI, 1.84-2.85] vs. respiratory involvement). A total of 398 patients (73.8%) with MIS-C and 253 (43.8%) with COVID-19 were admitted to the Intensive Care Unit, and 10 (1.9%) with MIS-C and 8 (1.4%) with COVID-19 died during hospitalisation. Among patients with MIS-C with reduced left ventricular systolic function (172/503, 34.2%) and coronary artery aneurysm (57/424, 13.4%), an estimated 91.0% (95% CI, 86.0%-94.7%) and 79.1% (95% CI, 67.1%-89.1%), respectively, normalized within 30 days.
‘Long COVID’
Osmanov et al34 report that compared with the <2 years age group older age 6–11 years (OR 2.74, 95% CI 1.37–5.75)was associated with a higher risk of persistent symptoms.
Borch et al31 report that symptoms include fatigue, loss of smell, loss of taste, respiratory problems, dizziness, muscle weakness and chest pain; and that in most children long COVID symptoms resolved within 1–5 months. Miller et al32 estimated the prevalence of persistent symptoms lasting ≥4 weeks as 1.0% in the 2-11-year-old age group. Children aged 12-17 were more likely to report persistent symptoms than children aged 2-11 (aOR 2.67, 1.56, 4.57). Persistent symptom prevalence was higher in girls, teenagers and children with long-term conditions. Say et al33 contrast the relatively rapid resolution of symptoms in children with studies of COVID-19 in adults, which have identified multisystem complications and a higher prevalence and severity of persistent symptoms. Bottino et al36 state that children with an asymptomatic or mildly symptomatic SARS-CoV-2 infection might be less prone to developing pulmonary complications than adults.
COMORBIDITIES
Harwood et al38 report that for children and young people aged <21 years the number of comorbid conditions was associated with increased odds of admission to critical care and death for COVID-19. Tsankov et al39 also report a higher risk of severe COVID-19 among children aged <21 years with comorbidities than for healthy children; relative risk ratio 1.79 (95% CI 1.27 – 2.51; I2 = 94%). Children <21 years with underlying conditions also had a higher risk of COVID-19-associated mortality; relative risk ratio 2.81 (95% CI 1.31 – 6.02; I2 = 82%). Children <21 years with obesity had a relative risk ratio of 2.87 (95% CI 1.16 – 7.07; I2 = 36%).
Verma et al41 report that children aged 0-21 years with obesity and asthma in particular were at increased risk for critical care admission and/or need for respiratory support.
In surveillance of SARS-CoV-2-associated deaths among children aged <21 years in the United States, Bixler et al40 found that 25% (n=30) of those who died had no medical comorbidities, 75% (n=91) had at least one underlying condition, and 45%(n=54) had two or more conditions. Asthma 28% (n=34), obesity 27%(n=33), neurological developmental 22% (n=26), and cardiovascular 18%(n=22) were the underlying conditions reported.
COLLATERAL HEALTH IMPACTS
Racine et al43 report that pooled estimates obtained in the first year of the COVID-19 pandemic suggest that 1 in 4 young people age ≤18 years globally are experiencing clinically elevated depression symptoms, while 1 in 5 young people age ≤18 years are experiencing clinically elevated anxiety symptoms. These pooled estimates, which increased over time, are double the pre-pandemic estimates.
Woolford et al45 report increased levels of paediatric obesity due to the pandemic. The greatest change in the distance from the median BMI for age occurred among 5- through 11-year-olds with an increased BMI of 1.57. Lange et al46 report that between the pre-pandemic and pandemic periods, the rate of BMI increase approximately doubled, from 0.052 (95% CI = 0.051-0.052 to 0.100 (95% CI = 0.098-0.101) kg/m2/month (ratio = 1.93 [95% CI = 1.90-1.96]). Persons aged 2-19 years with overweight or obesity during the pre-pandemic period experienced significantly higher rates of BMI increase during the pandemic period than did those with healthy weight.
Epidemiology and Severity of Illness in Children
| Level 1 |
The Centers for Disease Control and Prevention (CDC) (United States) caution that COVID-19 can cause severe illness in children and adolescents; and that between March 2020 and August 2021, cumulative COVID-19 associated hospitalization for all children aged 0-17 was 49.7/100,000 (69.2 in 0-4 years, 24 in 5-11 years, 63.7 in 12-17 years). Hospitalization rates increased across all age-groups with the Delta variant: the weekly hospitalization rate during the week ending 14 August 2021 was almost 5 times that of the week ending 26 June 2021. Among all hospitalized children, the proportions with severe disease after Delta became predominant were similar to those earlier in the pandemic. Hospitalization rates were 10.1 times higher in unvaccinated vs. fully-vaccinated adolescents in July 2021.
This CDC report may potentially over-estimate hospitalization rates as COVID-19 may have been an incidental diagnosis. In addition, there was a relatively small number of COVID-19 cases during the Delta in comparison with the Omicron period. Deaths following discharge from hospital were not included in the CDC analysis.
| Level 1 |
CDC caution that although COVID-19 generally results in milder disease in children and adolescents than in adults, severe illness from COVID-19 can occur in children and adolescents and may require hospitalization and Intensive Care Unit (ICU) support. CDC analysed new COVID-19 cases, Emergency Department (ED) visits with a COVID-19 diagnosis code, and hospital admissions of patients with confirmed COVID-19 among persons aged 0-17 years during the period August 1, 2020 to August 27, 2021. Since July 2021, after Delta had become the predominant circulating variant, the rate of new COVID-19 cases and COVID-19-related ED visits increased for persons aged 0-4, 5-11, and 12-17 years; and hospital admissions of patients with confirmed COVID-19 increased for persons aged 0-17 years. Incidence rates among persons aged 0–4, 5–11, and 12–17 years in June 2021 were 1.7, 1.9 and 2.9 cases per 100,000 persons, respectively, and increased to 6.2, 28.5, and 32.7 per 100,000 persons in August 2021. Among persons aged 0-17 years during the period August 14-27, 2021, COVID-19-related ED visits and hospital admissions in states with the lowest vaccination coverage were 3.4 and 3.7 times that of states with the highest vaccination coverage, respectively. At selected hospitals, the proportion of COVID-19 patients aged 0-17 years who were admitted to an ICU ranged from 10% to 25% from August 2020 to June 2021, and was 20% and 18% during July and August 2021, respectively. CDC reaffirms that broad, community-wide vaccination of all eligible persons is a critical component of mitigation strategies to protect paediatric populations from SARS-CoV-2 infection and severe COVID-19 illness.
| Level 2 |
BMJ Best Practice (2021) Coronavirus disease 2019 (COVID-19)[3]
See Section: EPIDEMIOLOGY: CHILDREN
Evidence suggests that children have a lower susceptibility to infection compared with adults. However, evidence is conflicting and the detailed relationship between age and susceptibility to infection requires further investigation. Emerging data suggests variants may spread more effectively and rapidly among young children, although hospitalization rates decreased.
Most cases in children are from familial clusters, or children who have a history of close contact with an infected patient. It is rare for children to be the index case in household transmission clusters. Children do not seem to be at higher risk for severe illness based on age or sex.
In the UK, a prospective observational cohort study found that children and young adults represented 0.9% of all hospitalized patients at the time. The median age of children admitted to hospital was 4.6 years, 56% were male, 35% were under 12 months of age, and 42% had at least one comorbidity. In terms of ethnicity, 57% were White, 12% were South Asian, and 10% were Black. Age under 1 month, age 10 to 14 years, and Black race were risk factors for admission to critical care.
In the US, a retrospective cohort study of over 135,000 children found that the mean age of infected children was 8.8 years, and 53% were male. In terms of ethnicity, 59% were White, 15% were Black, 11% were Hispanic, and 3% were Asian. Only 4% of children tested positive for SARS-CoV-2 in this population, and clinical manifestations were typically mild.
Globally, the case fatality rate in children appears to be higher in low- and middle-income countries compared with high-income countries.
| Level 2 |
UpToDate (2021) COVID-19: Clinical manifestations and diagnosis in children[4]
See Section: EPIDEMIOLOGY
Can children get COVID-19?
Children of all ages can get COVID-19. Although children typically have a lower risk of exposure and are tested less frequently than adults, the incidence in children is similar to that in adults. In studies where children and adolescents were tested for acute or past SARS-CoV-2 infection without respect to symptoms, the rates of infection in children ≥5 years were similar to or greater than those in adults. In surveillance from various countries children typically account for up to 18% of laboratory-confirmed cases.
In the United States, children under 18 years of age account for approximately 16% to 17% of cumulative laboratory-confirmed cases reported to the Centers for Disease Control and Prevention (CDC). The weekly number of cases reported to the CDC among persons <21 years of age has increased over time, possibly because increased numbers of children were tested as testing availability increased. Children account for approximately 15% of newly identified cases each week. The number of laboratory-confirmed cases of SARS-CoV-2 infection in children reported to the CDC is likely underestimated given the high proportion of mild and asymptomatic cases in which testing may not be performed.
Age Distribution
Children of all ages can get COVID-19. Among children and adolescents in the United States, there were more than 1.2 million positive tests for SARS-CoV-2 between March and December 2020, distributed as follows according to school age group:
- High school (age 14 through 17 years): 38.3%
- Middle school (age 11 through 13 years): 18.6%
- Elementary school (age 5 through 10 years): 25.7%
- Preschool (age 0 through 4 years): 17.4%
Race/Ethnicity
Among adult patients with COVID-19, underrepresented racial and ethnic groups are disproportionately affected, perhaps related to underlying health conditions and economic and social conditions. Children from underrepresented racial and ethnic groups also appear to be disproportionately affected by SARS-CoV-2, SARS-CoV-2 hospitalization, and SARS-CoV-2 deaths. The CDC’s COVID-NET provides race/ethnicity information for COVID-19-associated hospitalizations in children. Among children hospitalized with COVID-19 from 14 states, the cumulative hospitalization rate by late July 2020 was 16.9 per 100,000 population in Hispanic or Latin American children, 10.5 per 100,000 in non-Hispanic Black children, and 2.1 per 100,000 among White children. Among 121 SARS-CoV-2-associated deaths reported to the CDC among persons <21 years of age, nearly 80% occurred among Hispanic, non-Hispanic Black, and non-Hispanic American Indian/Alaskan Native persons, who account for approximately 40% of the population <21 years of age.
How do children get COVID-19?
In case series early in the pandemic, most cases in children resulted from household exposure, usually with an adult as the index patient. These findings must be interpreted with caution because the cases were identified after implementation of strict physical distancing measures, limiting the exposure of children to close contacts outside their household.
In observational studies of household transmission, the secondary attack rate among pediatric contacts (<18 years of age) ranged from 4% to 57% before the development of variants. In a meta-analysis of 87 studies of household transmission including 1,249,163 household contacts from multiple countries, the secondary attack rate was 18% among pediatric contacts (age <18 years) and 30% among adult contacts. Household transmission rates are increased with more transmissible variants. In a study of familial clusters during predominant circulation of the Alpha (B.1.1.7 lineage) variant, the secondary attack rate was 90% in adults and 72% to 75% in children <18 years of age.
How often are children with COVID-19 hospitalized?
CDC population-based surveillance and hospital admission data from the United States Department of Health and Human Services indicate that the number of monthly COVID-19 hospitalizations and weekly rates of COVID-19 hospitalizations among children <18 years of age peaked in January 2021, declined through June, and began to increase in July, when the Delta (B.1.617.2) variant become predominant. Weekly hospitalization rates for children <18 years peaked again in September (1.8 per 100,000 population), began to decline in October, but rose again thereafter when the Omicron (B.1.1.529) variant began circulating.
In population based surveillance, higher rates of SARS-CoV-2 vaccination coverage in the state and full vaccination among eligible adolescents were associated with lower rates of hospitalization. Despite the trend of increasing hospitalization with the predominance of the Delta variant, similar proportions of children required intensive care and invasive mechanical ventilation before and after predominance of the Delta variant.
With universal testing for SARS-CoV-2 upon admission at most hospitals, the rates of hospitalization for SARS-CoV-2 in children may be overestimated if hospitalizations for SARS-CoV-2-related illness are not differentiated from hospitalizations for other reasons (eg, elective surgery, trauma) with incidental detection of SARS-CoV-2. In CDC surveillance of COVID-19 in the United States, underlying conditions are associated with higher rates of hospitalization (15 to 22 versus 2 to 4%) and intensive care unit (ICU) admission (4 to 5 versus <1%). Whether underlying conditions are associated with increased severity or a lower threshold for admission is unclear. Age <1 year has also been associated with increased rates of hospitalization, although hospitalization of infants may not reflect severity of illness.
| Level 2 |
CDC report that children aged 5–11 years are at least as likely to be infected with SARS-CoV-2 as adults. There have been more than 1.9 million reported cases among children aged 5-11 years, and seroprevalence was estimated to be ~38% in September 2021. Seroprevalence data suggest that infections in children are less likely to be reported than infections in adults. Children aged 5–11 years are at risk of severe illness from COVID-19, and there have been more than 8,300 hospitalizations to date. Hospitalization rates are 3 times higher for non-Hispanic Black, non-Hispanic American Indian or Native Alaskan, and Hispanic children compared with non-Hispanic White children. Hospitalization rates are similar to pre-pandemic influenza-associated hospitalization rates. Severity was comparable among children hospitalized with influenza and COVID-19. Approximately 1/3 of hospitalized children aged 5–11 years require ICU admission. At least 94 COVID-19-associated deaths occurred in children aged 5–11 years in the period January 2020 to October 2021. MIS-C was most frequent among children aged 5–11 Children aged 5–11 years are at risk of severe illness from COVID-19, and there have been more than 8,300 hospitalizations to date. Hospitalization rates are 3 times higher for non-Hispanic Black, non-Hispanic American Indian or Native Alaskan, and Hispanic children compared with non-Hispanic White children. Hospitalization rates are similar to pre-pandemic influenza-associated hospitalization rates. Severity was comparable among children hospitalized with influenza and COVID-19. Post-COVID conditions have been reported in children. All might have been more numerous had pandemic mitigation measures not been implemented. Secondary transmission from young school-aged children occurs in household and school settings.
| Level 2 |
SARS-CoV-2 infection is rarely fatal in children and young people (CYP, <18 years old), but quantifying the risk of death is challenging because CYP are often infected with SARS-CoV-2 exhibiting no or minimal symptoms. To distinguish between CYP who died as a result of SARS-CoV-2 infection and those who died of another cause but were coincidentally infected with the virus, the authors carried out a clinical review of all CYP deaths with a positive SARS-CoV-2 test from March 2020 to February 2021. The predominant SARS-CoV-2 variants were wild-type and Alpha. The authors show that, of 12,023,568 CYP living in England, 3,105 died, including 61 who were positive for SARS-CoV-2. Of these deaths, 25 were due to SARS-CoV-2 infection (mortality rate, two per million), including 22 due to COVID-19, and 3 to pediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2 (PIMS-TS). In total, 99.995% of CYP with a positive SARS-CoV-2 test survived. CYP older than 10 years, Asian or Black ethnic background and comorbidities were over-represented in SARS-CoV-2-related deaths compared with other CYP deaths. New variants might have different mortality risks and should be evaluated in a similar way.
| Level 2 |
METHODS: During March 2020 to May 2021, the COVID-19–Associated Hospitalization Surveillance Network identified 3106 children hospitalized with laboratory-confirmed SARS-CoV- 2 infection in 14 states. Among 2293 children primarily admitted for COVID-19, multivariable generalized estimating equations generated adjusted risk ratios (aRRs) and 95% confidence intervals (CIs) of the associations between demographic and medical characteristics abstracted from patient electronic medical records and severe COVID-19. The authors calculated age-adjusted cumulative population-based rates of severe COVID-19 among all children.
RESULTS: Approximately 30% of hospitalized children had severe COVID-19; 0.5% died during hospitalization. Among hospitalized children aged <2 years, chronic lung disease (aRR: 2.2; 95% CI: 1.1–4.3), neurologic disorders (aRR: 2.0; 95% CI: 1.5‒2.6), cardiovascular disease (aRR: 1.7; 95% CI: 1.2‒2.3), prematurity (aRR: 1.6; 95% CI: 1.1‒2.2), and airway abnormality (aRR: 1.6; 95% CI: 1.1‒2.2) were associated with severe COVID-19. Among hospitalized children aged 2 to 17 years, feeding tube dependence (aRR: 2.0; 95% CI: 1.5‒2.5), diabetes mellitus (aRR: 1.9; 95% CI: 1.6‒2.3) and obesity (aRR: 1.2; 95% CI: 1.0‒1.4) were associated with severe COVID-19. Severe COVID-19 occurred among 12.0 per 100 000 children overall and was highest among infants, Hispanic children, and non-Hispanic Black children.
CONCLUSIONS: Results identify children at potentially higher risk of severe COVID-19 who may benefit from prevention efforts, including vaccination. Rates establish a baseline for monitoring changes in pediatric illness severity after increased availability of COVID-19 vaccines and the emergence of new variants.
| Level 2 |
While early evidence and experience with COVID-19 suggest that children are less susceptible to infection and have a lower risk for symptomatic and severe disease, pediatric patients are not immune from the virus. The authors examined pediatric COVID-19 hospitalization trends in 22 states for indications of both severity among this population and spread of the virus.
Methods: Using data extracted from the University of Minnesota COVID-19 Hospitalization Tracking Project, the authors identified the 22 states that reported cumulative COVID-19 hospitalizations overall and for patients 19 years and younger (in some states younger than 17 or 14 years) between May 15, 2020, and November 15, 2020. State-level hospitalization data with population estimates from the US Census were combined. Cumulative pediatric COVID-19 hospitalizations per 100 000 children were calculated at regular time intervals, and growth rates were calculated on the changes in per capita hospitalizations. Cross-sectional analyses done include tabulations by state over time.
Results: There were a total of 301,102 COVID-19 hospitalizations and 5,364 pediatric COVID-19 hospitalizations in 22 states during the study period. At the beginning of the study, the average cumulative hospitalization rate for children was 2.0 per 100 000 children, increasing to 17.2 per 100,000 children by the end of the study.
| Level 4 |
The Delta (B.1.617.2) SARS-CoV-2 variant became the predominant UK circulating strain in May 2021. Whether COVID-19 from Delta infection differs to infection with other variants in children is unknown.
Methods: Through the prospective COVID Symptom Study, 109,626 UK school-aged children were proxy-reported between December 28, 2020 and July 8, 2021. The authors selected all symptomatic children who tested positive for SARS-CoV-2 and were proxy-reported at least weekly, within two timeframes: December 28, 2020 to May 6, 2021 (Alpha (B.1.1.7) the main UK circulating variant); and May 26 to July 8, 2021 (Delta the main UK circulating variant). Illness profiles (symptom prevalence, duration, and burden), hospital presentation, and presence of long (≥28 day) illness were assessed; and calculated odds ratios for symptoms presenting within the first 28 days of illness.
Findings: 694 (276 younger [5-11 years], 418 older [12-17 years]) symptomatic children tested positive for SARS-CoV-2 with Alpha infection and 706 (227 younger and 479 older) children with Delta infection. Median illness duration was short with either variant (overall cohort: 5 days (IQR 2–9.75) with Alpha, 5 days (IQR 2-9) with Delta). The most prevalent symptoms were common to both variants: rhinorrhoea, headache and fatigue. Symptom burden over the first 28 days was slightly greater with Delta compared with Alpha infection (in younger children, 3 (IQR 2–5) with Alpha, 4 (IQR 2–7) with Delta; in older children 5 (IQR 3–8) with Alpha and 6 (IQR 3–9) with Delta infection in older children). The odds of several symptoms were higher with Delta than Alpha infection, including headache and fever. Few children presented to hospital, and long illness duration was uncommon with either variant. Illness had resolved by 28 days in 274 [99.3%] of 276 children with Alpha infection and in 224 [98.7%] of 227 children with Delta infection.
Interpretation: COVID-19 in UK school-aged children due to SARS-CoV-2 Delta strain B.1.617.2 resembles illness due to the Alpha variant B.1.1.7., with short duration and similar symptom burden.
| Level 4 |
Identifying which children and young people (CYP) are vulnerable to severe disease following SARS-CoV-2 is important to guide shielding and vaccination policy.
Methods: The authors used data for all inpatient hospital admissions in England in CYP aged 0-17 between March 1, 2020 and February 28, 2021, examining associations between PICU admission and death by sociodemographic factors and comorbidities within COVID-19 and PIMS-TS admissions. Odds ratios and predicted probability of PICU admission were calculated using generalized estimation equations, and compared between COVID-19, PIMS-TS, other admissions in 2020/21, all admissions in 2019/20, and admissions due to influenza in 20219/20. Analyses of deaths were descriptive due to low numbers.
Findings: Of the 12.02 million 0-17 year olds in England during 2020, 1 in 2062 (n=5830) were admitted to hospital due to COVID-19, and 1 in 47,903 (n=251) were admitted to PICU. This represents only 1.3% of all secondary care admissions in the pandemic year and <5% of non-traumatic emergency PICU admissions. 8 of these 0-17-year-olds died. Within COVID-19, there were 6,338 hospital admissions, 259 PICU admissions and 8 deaths. Within PIMS-TS there were 712 hospital admissions, 312 PICU admissions and <5 deaths. Males were 52.8% of COVID-19 admissions, but were 63.5% of PIMS-TS admissions. CYP aged 10-17 were 35.6% and 29% of COVID-19 and PIMS-TS admissions respectively, higher than in all admission and influenza admissions in 2019/20. In multivariable models, odds of PICU admission were: increased among neonates, and decreased among 15-17 compared with 1-4 year olds with COVID-19; increased in older CYP and females with PIMS-TS; and increased for Black compared with White ethnicity in COVID-19 and PIMS-TS. Odds of PICU admission with COVID-19 were increased for CYP with any comorbidity and were highest for CYP with multiple medical problems. Increases in risk of PICU admission associated with comorbidities showed similar patterns for COVID-19 and all admissions in 2019/20 and influenza admissions in 2019/20, but were greater for COVID-19. Interpreting associations with comorbidities within PIMS-TS was complex due to the multisystem nature of the disease.
Interpretation: CYP were at very low risk of severe disease and death from COVID-19 or PIMS-TS. PICU admission due to PIMS-TS was associated with older non-White CYP. Patterns of vulnerability for severe COVID-19 appear to magnify background risk factors for serious illness in CYP.
| Level 4 |
This cohort study uses data from the Premier Healthcare Database Special COVID-19 Release to assess the association of demographic and clinical characteristics with severe COVID-19 illness among hospitalized US pediatric patients with COVID-19.
Findings: Among 20,714 pediatric patients with COVID-19, 3,497 (16.9%) were aged 6-11. 274 (7.8%) of those infected and aged 6-11 years were hospitalized with COVID-19, 119 (3.4%) had severe disease and 119 (3.4%) were admitted to ICU. An increased association of severe COVID-19 was observed among patients with one or more chronic conditions vs. those with none (AOR, 3.27; 95% CI, 2.44-4.37); and in children aged 2-5 years or 6-11 years vs. those aged 12-18 years (AORs, 1.53; 95% CI, 1.11-2.13 and 1.53; 95% CI, 1.04-2.23, respectively).
| Level 4 |
Data about the risk of SARS-CoV-2 infection among children compared with adults are needed to inform COVID-19 risk communication and prevention strategies, including COVID-19 vaccination policies for children.
Objective: To compare incidence rates and clinical characteristics of SARS-CoV-2 infection among adults and children and estimated household infection risks within a prospective household cohort.
Design, setting, and participants: Households with at least 1 child aged 0 to 17 years in selected counties in Utah and New York City, New York, were eligible for enrolment. From September 2020 through April 2021, participants self-collected mid-turbinate nasal swabs for RT-PCR testing for SARS-CoV-2 and responded to symptom questionnaires each week. Participants also self-collected additional respiratory specimens with onset of suspected COVID-19 symptoms. For children unable to self-collect respiratory specimens, an adult caregiver collected the specimens.
Main outcomes and measures: The primary outcome was incident cases of any SARS-CoV-2 infection, including asymptomatic and symptomatic infections. Additional measures were the asymptomatic fraction of infection calculated by dividing incidence rates of asymptomatic infection by rates of any infection, clinical characteristics of infection, and household infection risks. Primary outcomes were compared by participant age group.
Results: A total of 1236 participants in 310 households participated in surveillance, including 176 participants (14%) who were aged 0 to 4 years, 313 (25%) aged 5 to 11 years, 163 (13%) aged 12 to 17 years, and 584 (47%) 18 years or older. Overall incidence rates of SARS-CoV-2 infection were 3.8 (95% CI, 2.4-5.9) and 7.7 (95% CI, 4.1-14.5) per 1000 person-weeks among the Utah and New York City cohorts, respectively. Site-adjusted incidence rates per 1000 person-weeks were similar by age group: 6.3 (95% CI, 3.6-11.0) for children 0 to 4 years, 4.4 (95% CI, 2.5-7.5) for children 5 to 11 years, 6.0 (95% CI, 3.0-11.7) for children 12 to 17 years, and 5.1 (95% CI, 3.3-7.8) for adults (≥18 years). The asymptomatic fractions of infection by age group were 52%, 50%, 45%, and 12% among individuals aged 0 to 4 years, 5 to 11 years, 12 to 17 years, and 18 years or older, respectively. Among 40 households with 1 or more SARS-CoV-2 infections, the mean risk of SARS-CoV-2 infection among all enrolled household members was 52% (range, 11%-100%), with higher risks in New York City compared with Utah (80% [95% CI, 64%-91%] vs 44% [95% CI, 36%-53%]; P < .001).
Conclusions and relevance: In this study, children had similar incidence rates of SARS-CoV-2 infection compared with adults, but a larger proportion of infections among children were asymptomatic.
| Level 4 |
Graff et al (2021) [Retrospective Cohort Study] Risk Factors for Severe COVID-19 in Children[13]
This study aims to describe the epidemiology and identify risk factors for severe COVID-19 disease in children.
Methods: A retrospective cohort study among children with positive SARS-CoV-2 PCR from March to July 2020 at Children’s Hospital Colorado. Risk factors for severe disease were analyzed as defined by hospital admission, respiratory support, or critical care. Univariable and multivariable analyses were conducted.
Results: Among 454 patients identified with SARS-CoV-2, 191 (42.1%) were females, median age 11 years. 55% of all patients identified as Hispanic compared with 29% among all hospital visits in 2019 (P < 0.0001). In multivariable analyses, age 0-3 months or >20 years (adjusted odds ratio (aOR), 7.85; p < 0.0001 and aOR, 5.1; p = 0.03, respectively), preterm birth history (aOR, 3.7; p = 0.03), comorbidities (including immunocompromise (aOR, 3.5; p = 0.004), gastrointestinal condition (aOR, 2.7; p = 0.009), diabetes (aOR, 6.6; p = 0.04), asthma (aOR, 2.2; p = 0.04)), and specific symptoms at presentation were predictors for admission. Age 0-3 months or >20 years, asthma, gastrointestinal condition, and similar symptoms at presentation were also predictors for respiratory support. Elevated C-reactive protein was associated with the need for critical care with median of 17.7 mg/dL (IQR, 5.3-22.9) vs. 1.95 mg/dL (IQR, 0.7-5.5) among patients requiring critical vs. no critical care (OR, 1.2; p = 0.02).
Conclusions: Extremes of age, comorbid conditions, and elevated CRP are predictors of severe disease in children.
| Level 4 |
Children and adolescents account for ~ 13% of total COVID-19 cases in the United States. This study sought to assess the clinical characteristics and outcomes in pediatric COVID-19 patients. The authors conducted a retrospective cross-sectional analysis of pediatric patients diagnosed with COVID-19 from healthcare organizations in the United States. Study outcomes —hospitalization, mechanical ventilation, and critical care — were assessed using logistic regression. The subgroups of sex and race were compared after propensity score matching. Among 12,306 children with lab-confirmed COVID-19, 16.5% presented with respiratory symptoms (cough, dyspnea), 13.9% had gastrointestinal symptoms (nausea, vomiting, diarrhea, abdominal pain), 8.1% had dermatological symptoms (rash), 4.8% had neurological symptoms (headache), and 18.8% had other non-specific symptoms (fever, malaise, myalgia, arthralgia and disturbances of smell or taste). In the study cohort, the hospitalization frequency was 5.3%, with 17.6% needing critical care services and 4.1% requiring mechanical ventilation. There were ≤ 10 deaths in the study population. Among those without any comorbidities (N = 8,297), the frequency of hospitalization was 3.5%, 0.4% required critical care, and 0.3% required mechanical ventilation. Following propensity score matching, the risk of all outcomes was similar between males and females. Following propensity score matching, the risk of hospitalization was greater in non-Hispanic Black (RR 1.97 [95% CI 1.49–2.61]) and Hispanic children (RR 1.31 [95% CI 1.03–1.78]) compared with non-Hispanic White children. In the pediatric population infected with COVID-19, a substantial proportion were hospitalized due to the illness and developed adverse clinical outcomes.
Transmission
| Level 1 |
A previous systematic review and meta-analysis of household transmission of SARS-CoV-2 that summarized 54 published studies through October 19, 2020, found an overall secondary attack rate (SAR) of 16.6% (95% CI, 14.0%-19.3%). However, the understanding of household secondary attack rates for SARS-CoV-2 is still evolving, and updated analysis is needed.
Overall household SAR for SARS-CoV-2, SAR by covariates (contact age, sex, ethnicity, comorbidities, and relationship; index case age, sex, symptom status, presence of fever, and presence of cough; number of contacts; study location; and variant), and SAR by index case identification period were calculated.
Results: A total of 2722 records (2710 records from database searches and 12 records from the reference lists of eligible articles) published between October 20, 2020, and June 17, 2021, were identified. Of those, 93 full-text articles reporting household transmission of SARS-CoV-2 were assessed for eligibility, and 37 studies were included. These 37 new studies were combined with 50 of the 54 studies (published through October 19, 2020) from our previous review (4 studies from Wuhan, China, were excluded because their study populations overlapped with another recent study), resulting in a total of 87 studies representing 1 249 163 household contacts from 30 countries. The estimated household SAR for all 87 studies was 18.9% (95% CI, 16.2%-22.0%). Compared with studies from January to February 2020, the SAR for studies from July 2020 to March 2021 was higher (13.4% [95% CI, 10.7%-16.7%] vs. 31.1% [95% CI, 22.6%-41.1%], respectively). Results from subgroup analyses were similar to those reported in a previous systematic review and meta-analysis; however, the SAR was higher to contacts with comorbidities (3 studies; 50.0% [95% CI, 41.4%-58.6%]) compared with previous findings, and the estimated household SAR for the B.1.1.7 (α) variant was 24.5% (3 studies; 95% CI, 10.9%-46.2%).
Conclusions and relevance: The findings of this study suggest that the household remains an important site of SARS-CoV-2 transmission, and recent studies have higher household SAR estimates compared with the earliest reports. More transmissible variants and vaccines may be associated with further changes.
| Level 1 |
There is uncertainty with respect to SARS-CoV-2 transmission in children (0-19 years) with controversy on effectiveness of school-closures in controlling the pandemic. It is of equal importance to evaluate the risk of transmission in children who are often asymptomatic or mildly symptomatic carriers that may incidentally transmit SARS-CoV-2 in different settings. The authors conducted a systematic review to assess transmission and risks for SARS-CoV-2 in children (by age-groups or grades) in community and educational-settings compared to adults.
Results: 90 studies were included. Compared to adults, children showed comparable national (RR = 0.87, 95% CI = 0.71-1.060) and subnational (RR = 0.81, 95% CI = 0.66-1.01) prevalence in population-screening studies, and lower odds of infection in community/household contact-tracing studies (OR = 0.62, 95% CI = 0.46-0.84). On disaggregation, adolescents observed comparable risk (OR = 1.22, 95% CI = 0.74-2.04) with adults. In educational-settings, children attending daycare/preschools (OR = 0.53, 95% CI = 0.38-0.72) were observed to be at lower-risk when compared to adults, with odds of infection among primary (OR = 0.85, 95% CI = 0.55-1.31) and high-schoolers (OR = 1.30, 95% CI = 0.71-2.38) comparable to adults. Overall, children and adolescents had lower odds of infection in educational-settings compared to community and household clusters.
Conclusions: Children (<10 years) showed lower susceptibility to COVID-19 compared to adults, whereas adolescents in communities and high-schoolers had comparable risk. Risks of infection among children in educational-settings was lower than in communities. Evidence from school-based studies demonstrate it is largely safe for children (<10 years) to be at schools, however older children (10-19 years) might facilitate transmission.
| Level 1 |
Objective: To systematically review the susceptibility to and transmission of SARS-CoV-2 among children and adolescents compared with adults.
Data sources: PubMed and medRxiv were searched from database inception to July 28, 2020, and a total of 13 926 studies were identified, with additional studies identified through hand searching of cited references and professional contacts.
Study selection: Studies that provided data on the prevalence of SARS-CoV-2 in children and adolescents younger than 20 years compared with adults derived from contact tracing or population screening were included. Single-household studies were excluded.
Results: A total of 32 studies comprising 41 640 children and adolescents and 268 945 adults met inclusion criteria, including 18 contact-tracing studies and 14 population screening studies. The pooled odds ratio of being an infected contact in children compared with adults was 0.56 (95% CI, 0.37-0.85), with substantial heterogeneity (I2 = 94.6%). Three school-based contact-tracing studies found minimal transmission from child or teacher index cases. Findings from population screening studies were heterogenous and were not suitable for meta-analysis. Most studies were consistent with lower seroprevalence in children compared with adults, although seroprevalence in adolescents appeared similar to adults.
Conclusions and relevance: In this meta-analysis, there is preliminary evidence that children and adolescents have lower susceptibility to SARS-CoV-2, with an odds ratio of 0.56 for being an infected contact compared with adults. There is weak evidence that children and adolescents play a lesser role than adults in transmission of SARS-CoV-2 at a population level. This study provides no information on the infectivity of children.
| Level 2 |
UpToDate (2021) COVID-19: Clinical manifestations and diagnosis in children[18]
Do children transmit SARS-CoV-2 to others?
Children of all ages can transmit SARS-CoV-2 to others, but the relative transmissibility of SARS-CoV-2 by children in various age groups is uncertain, given the varying contributions of biologic, host, and environmental factors. Older children and adolescents transmit SARS-CoV-2 effectively in household and community settings. Infected children shed SARS-CoV-2 virus with nasopharyngeal viral loads comparable to or higher than those in adults.
Household Transmission: Transmission from children to household contacts occurs, although the relative frequency of transmission from young children compared with other age groups is uncertain.
Household contact studies have identified variable rates of transmission from pediatric index cases. In some studies, transmission from children to household contacts is infrequent; in other studies, rates of transmission from children to household contacts are similar to or higher than those in adults. The variable rates may be related to different community prevalence and mitigation measures, methods of diagnosing secondary cases, timing of sample collection, and levels of adherence to infection control measures in the home, which is particularly challenging when the index patient is a young child.
Transmission in Educational or Child Care Settings: Limited evidence suggests that transmission by preadolescent children occurs but is uncommon in educational or child care settings, particularly if the class size is small, other public health measures are strictly followed, and community transmission is low, although findings are inconsistent.
Transmission by presymptomatic children and adolescents also appears to be uncommon in educational settings when effective case-contact testing and epidemic control strategies (eg, universal use of well-fitted masks, physical distancing, improved ventilation) are implemented.
In the United States and other countries, resumption of in-person primary and secondary education before the emergence of more transmissible variants was associated with relatively few reports of school outbreaks when mitigation strategies (eg, mask-wearing, cohorting classrooms) were in place.
Transmission by Asymptomatic Children: Although there is little information about transmission of SARS-CoV-2 by truly asymptomatic (as opposed to presymptomatic) children, transmission from children with confirmed asymptomatic SARS-CoV-2 to household contacts has been reported. In addition, there are reports of familial clusters that included asymptomatic children and possible transmission from asymptomatic children to adults outside their family. These reports suggest that asymptomatic children may play a role in transmission. Asymptomatic transmission by adults is well documented.
| Level 2 |
Key findings of the report from 16 June to 31 July 2021 include:
- In 51 educational settings (19 schools and 32 ECEC services), there were 59 individuals (34 students and 25 staff members) with COVID-19 who attended the educational setting while infectious. For these 59 primary (first) cases, 2,347 close contacts from schools and ECEC services (1,830 students and 517 staff members) were identified. Testing for SARS-CoV-2 infection occurred for 96% of close contacts.
- Most children in this study had no or only mild symptoms from COVID-19, while 2% across the state required hospitalisation.
- The overall transmission rate from primary cases to close contacts was 4.7% (106 secondary cases, comprising 69 students and 37 staff members, in 2,253 tested close contacts). Virus transmission occurred in 19 of the 51 educational settings (38%; 3 primary schools and 16 ECEC services).
- The highest transmission rates occurred in ECEC services between staff members (16.9%) and from a staff member to children (8.1%). ECEC services were fully open with high attendance rates during this period and many staff were not yet age-eligible for vaccination. The majority of affected ECEC services (28/32) were in the Local Government Areas (LGAs) with the highest community incidence rates of COVID-19 in Sydney.
- Transmission was low in schools (1.2%; 9 secondary cases in 728 close contacts). This was likely due to the school holiday period and subsequent limited onsite attendance in Term 3, when the majority of Greater Sydney was under stay-at-home orders and students engaged in remote learning.
- Staff and children who contracted COVID-19 at a school or ECEC service often passed it on to their household members. There were 181 household tertiary cases following exposure to the 106 secondary cases from the school or ECEC service. The overall transmission rate among household contacts was 70.7%.
- The rate of transmission of the SARS-CoV-2 Delta variant in both schools and ECEC services as well as in households was around 5 times higher than seen in educational settings and households in this study in 2020 with the original strain of the COVID-19 virus.
| Level 4 |
Objective: To determine whether there are differences in the odds of household transmission by younger children compared with older children.
Design, setting, and participants: This population-based cohort study took place between June 1 and December 31, 2020, in Ontario, Canada. Private households in which the index case individual of laboratory-confirmed SARS-CoV-2 infection was younger than 18 years were included. Individuals were excluded if they resided in apartments missing suite information, in households with multiple index cases, or in households where the age of the index case individual was missing.
Exposures: Age group of pediatric index cases categorized as 0 to 3, 4 to 8, 9 to 13, and 14 to 17 years.
Main outcomes and measures: Household transmission, defined as households where at least 1 secondary case occurred 1 to 14 days after the pediatric index case.
Results: A total of 6280 households had pediatric index cases, and 1717 households (27.3%) experienced secondary transmission. The mean (SD) age of pediatric index case individuals was 10.7 (5.1) years and 2863 (45.6%) were female individuals. Children aged 0 to 3 years had the highest odds of transmitting SARS-CoV-2 to household contacts compared with children aged 14 to 17 years (OR 1.43; 95% CI, 1.17-1.75). This association was similarly observed in sensitivity analyses defining secondary cases as 2 to 14 days or 4 to 14 days after the index case and stratified analyses by presence of symptoms, association with a school/childcare outbreak, or school/childcare reopening. Children aged 4 to 8 years and 9 to 13 years also had increased odds of transmission (aged 4-8 years: OR 1.40; 95% CI, 1.18-1.67; aged 9-13 years: OR 1.13; 95% CI, 0.97-1.32).
Conclusions and relevance: This study suggests that younger children may be more likely to transmit SARS-CoV-2 infection compared with older children, and the highest odds of transmission was observed for children aged 0 to 3 years. Differential infectivity of pediatric age groups has implications for infection prevention within households, as well as schools/childcare, to minimize risk of household secondary transmission.
| UNCLASSIFIED |
Chun et al (2021) Age-Varying Susceptibility to the Delta Variant (B.1.617.2) of SARS-CoV-2[21]
Methods: Combining age-specific contact matrices and observed periods between each stage of infection, the authors constructed a compartmental model (SEIQ) of COVID-19 transmission, comparing age-specific susceptibility to the Delta variant with susceptibility to the original virus, using the 3rd (pre-Delta) and 4th (driven by the Delta variant) waves in South Korea.
Findings: A significant difference between age-specific susceptibility to Delta and that to the pre-Delta variant was found in the younger age group. The fold rise in susceptibility to the Delta/pre-Delta variant was highest in the 10–15 years age group (1.92-fold rise), whereas in those aged 50 years or more, the susceptibility to the Delta/pre-Delta remained stable at approximately one-fold.
Interpretation: Even after adjusting for both contact pattern and vaccination status, the Delta variant of SARS-CoV-2 tends to propagate more easily among children than the pre-Delta strains.
Multisystem Inflammatory Syndrome in Children (MIS-C)
| Level 1 |
An association between a novel pediatric hyperinflammatory condition and SARS-CoV-2 was recently published and termed pediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2 (PIMS-TS) or multisystem inflammatory syndrome in children (MIS-C). The authors performed a systematic review and describe the epidemiological, clinical and prognostic characteristics of 953 PIMS-TS/MIS-C cases in 68 records. Additionally, the authors studied the sensitivity of different case definitions that are currently applied. PIMS-TS/MIS-C presents at a median age of 8 years. Epidemiological enrichment for males (58.9%) and ethnic minorities (37.0% Black) is present. Apart from obesity (25.3%), comorbidities are rare. PIMS-TS/MIS(-C) is characterized by fever (99.4%), gastrointestinal (85.6%) and cardiocirculatory manifestations (79.3%), and increased inflammatory biomarkers. Nevertheless, 50.3% present respiratory symptoms as well. Over half of patients (56.3%) present with shock. The majority of the patients (73.3%) need intensive care treatment, including extracorporal membrane oxygenation (ECMO) in 3.8%. Despite severe disease, mortality is low (1.9%). Of the currently used case definitions, the WHO definition is preferred, as it is more precise, while encompassing most cases.
Conclusion: PIMS-TS/MIS-C is a severe, heterogeneous disease with epidemiological enrichment for males, adolescents, and racial and ethnic minorities. However, mortality rate is low and short-term outcome favorable. Long-term follow-up of chronic complications and additional clinical research to elucidate the underlying pathogenesis is crucial.
This systematic review illustrates the heterogeneous spectrum of PIMS-TS/MIS-C and its epidemiological enrichment for males, adolescents, and racial and ethnic minorities. Despite its severe presentation, overall short-term outcome is good.
| Level 2 |
See Section: EPIDEMIOLOGY
While the incidence of MIS-C is uncertain, it appears to be a relatively rare complication of COVID-19 in children, occurring in <1% of children with confirmed SARS-CoV-2 infection. In one report from New York State, the estimated incidence of laboratory-confirmed SARS-CoV-2 infection in individuals <21 years old was 322 per 100,000 and the incidence of MIS-C was 2 per 100,000.
While some children with MIS-C meet criteria for complete or incomplete Kawasaki disease (KD), the epidemiology differs from that of classic KD. Most MIS-C cases have occurred in older children and adolescents who were previously healthy. Black and Hispanic children appear to be disproportionally affected. By contrast, classic KD typically affects infants and young children and has a higher incidence in East Asia and in children of Asian descent.
The epidemiology of MIS-C also differs from that of severe acute COVID-19 illness in children, which more often occurs in children with underlying health problems.
The first report of MIS-C was a series of eight children seen at a tertiary center in South East England. In subsequent larger case series from the United Kingdom and the United States, >70% of affected children were previously healthy. The most common comorbidities were obesity and asthma. The median age was 8 to 11 years (range 1 to 20 years).
Rates of MIS-C appear to vary by race and ethnicity, with Black and Hispanic children accounting for a disproportionally high number of cases and Asian children accounting for a small number of cases.
In most studies, there was a lag of several weeks between the peak of COVID-19 cases within communities and the rise of MIS-C cases. For example, in London, the peak of COVID-19 cases occurred in the first to second weeks of April, while the spike of MIS-C cases occurred in the first to second week of May. This three- to four-week lag coincides with the timing of acquired immunity and suggests that MIS-C may represent a post-infectious complication of the virus rather than acute infection, at least in some children.
| Level 2 |
Paediatric Multisystem Inflammatory Syndrome temporally associated with SARS-CoV-2 (PIMS-TS), first identified in April 2020, shares features of both Kawasaki disease (KD) and toxic shock syndrome (TSS). This surveillance study describes the epidemiology and clinical characteristics of PIMS-TS in the United Kingdom and Ireland.
Methods: Public Health England initiated prospective national surveillance of PIMS-TS through the British Paediatric Surveillance Unit. Paediatricians were contacted monthly to report PIMS-TS, KD and TSS cases electronically and complete a detailed clinical questionnaire. Cases with symptom onset between 01 March and 15 June 2020 were included.
Findings: There were 216 cases with features of PIMS-TS alone, 13 with features of both PIMS-TS and KD, 28 with features of PIMS-TS and TSS and 11 with features of PIMS-TS, KD and TSS, with differences in age, ethnicity, clinical presentation and disease severity between the phenotypic groups. 5-9-year-olds accounted for 30% (n=80) of cases. Across all age groups, males were over-represented (60%), 19% had co-morbidities, and 13.4% were overweight. For MIS-C only cases, 48.6% were White, 20.4% Asian and 19.4% Black.
44% (n=118) of MIS-C cases were admitted to PICU and 1.1% (n=3) died. There was a strong geographical and temporal association between SARS-CoV-2 infection rates and PIMS-TS cases. Of those tested, 14.8% (39/264) children had a positive SARS-CoV-2 RT-PCR, and 63.6% (75/118) were positive for SARS-CoV-2 antibodies. In total 44·0% (118/268) required intensive care, which was more common in cases with a TSS phenotype. Three of five children with cardiac arrest had TSS phenotype. Three children (1·1%) died.
Interpretation: The strong association between SARS-CoV-2 infection and PIMS-TS emphasises the importance of maintaining low community infection rates to reduce the risk of this rare but severe complication in children and adolescents. Close follow-up will be important to monitor long-term complications in children with PIMS-TS.
| Level 4 |
Results: There were 35 deaths from MIS-C among the 2,818 cases of MIS-C reported from February 2020 to March 2021. 7 deaths occurred in the 6-11-year-old age group. The 6-11-year-old age group had a [non-statistically significant] lower risk of death from MIS-C compared with all other child age groups. 16-20 year olds had a significantly higher odds of death.
Across all age groups, having one or more underlying medical conditions was associated with increased risk of death from MIS-C (aOR, 2.8; 95% CI, 1.4–5.9).
| Level 4 |
Multisystem inflammatory syndrome in children (MIS-C) is associated with recent or current SARS-CoV-2 infection. Information on MIS-C incidence is limited.
Objective: To estimate population-based MIS-C incidence per 1 000 000 person-months and to estimate MIS-C incidence per 1 000 000 SARS-CoV-2 infections in persons younger than 21 years.
Design, setting, and participants: This cohort study used enhanced surveillance data to identify persons with MIS-C during April to June 2020, in 7 jurisdictions reporting to both the Centers for Disease Control and Prevention national surveillance and to Overcoming COVID-19, a multicenter MIS-C study. Denominators for population-based estimates were derived from census estimates; denominators for incidence per 1 000 000 SARS-CoV-2 infections were estimated by applying published age- and month-specific multipliers accounting for underdetection of reported COVID-19 case counts. Jurisdictions included Connecticut, Georgia, Massachusetts, Michigan, New Jersey, New York (excluding New York City), and Pennsylvania. Data analyses were conducted from August to December 2020.
Exposures: Race/ethnicity, sex, and age group (≤5, 6-10, 11-15, and 16-20 years).
Main outcomes and measures: Overall and stratum-specific adjusted estimated MIS-C incidence per 1 000 000 person-months and per 1 000 000 SARS-CoV-2 infections.
Results: In the 7 jurisdictions examined, 248 persons with MIS-C were reported (median [interquartile range] age, 8 [4-13] years; 133 [53.6%] male; 96 persons [38.7%] were Hispanic or Latino; 75 persons [30.2%] were Black). The incidence of MIS-C per 1 000 000 person-months was 5.1 (95% CI, 4.5-5.8) persons. Compared with White persons, incidence per 1 000 000 person-months was higher among Black persons (adjusted incidence rate ratio [aIRR], 9.26 [95% CI, 6.15-13.93]), Hispanic or Latino persons (aIRR, 8.92 [95% CI, 6.00-13.26]), and Asian or Pacific Islander (aIRR, 2.94 [95% CI, 1.49-5.82]) persons. MIS-C incidence per 1 000 000 SARS-CoV-2 infections was 316 (95% CI, 278-357) persons and was higher among Black (aIRR, 5.62 [95% CI, 3.68-8.60]), Hispanic or Latino (aIRR, 4.26 [95% CI, 2.85-6.38]), and Asian or Pacific Islander persons (aIRR, 2.88 [95% CI, 1.42-5.83]) compared with White persons. For both analyses, incidence was highest among children aged 5 years or younger (4.9 [95% CI, 3.7-6.6] children per 1 000 000 person-months) and children aged 6 to 10 years (6.3 [95% CI, 4.8-8.3] children per 1 000 000 person-months).
Conclusions and relevance: In this cohort study, MIS-C was a rare complication associated with SARS-CoV-2 infection. Estimates for population-based incidence and incidence among persons with infection were higher among Black, Hispanic or Latino, and Asian or Pacific Islander persons. Further study is needed to understand variability by race/ethnicity and age group.
| Level 4 |
This cohort study describes the distribution of race/ethnicity among cases of coronavirus disease 2019 (COVID-19)–associated multisystem inflammatory syndrome in children reported to the New York City Department of Health and Mental Hygiene.
Findings: Overall MIS-C incidence was 11.4 cases per 100,000 population (<20 years). Compared with White children, there was a higher incidence of MIS-C among Black (IRR, 3.2; 95% CI, 2.0-4.9) and Hispanic (IRR, 1.7; 95% CI, 1.1-2.7) children and no difference among Asian or Pacific Islander children (IRR, 0.9; 95% CI, 0.4-1.7). Black (IRR, 1.7; 95% CI, 1.3-2.2) and Hispanic (IRR, 2.1; 95% CI, 1.7-2.7) children had higher COVID-19 hospitalization rates compared with White children.
| Level 4 |
Data from adult studies show that COVID-19 is more severe in men than women. However, no data are available for the pediatric population. This study sought to understand if sex influenced disease severity and outcomes in a large cohort of Latin-American children with COVID-19 and Multisystem Inflammatory Syndrome (MIS-C). The authors found that a higher percentage of male children developed MIS-C (8.9% vs 5% in females) and died (1.2% and 0.4% in females), although on multivariate adjusted analyses the only statistically significant difference was found in need for hospitalization, with females less frequently admitted compared with males (25.6% vs. 35.4%). These data are preliminary and need further independent studies to better assess the role of sex and COVID-19 severity.
| Level 5 |
Refinement of criteria for multisystem inflammatory syndrome in children (MIS-C) may inform efforts to improve health outcomes.
Objective: To compare clinical characteristics and outcomes of children and adolescents with MIS-C vs. those with severe coronavirus disease 2019 (COVID-19).
Setting, design, and participants: Case series of 1116 patients aged younger than 21 years hospitalized between March 15 and October 31, 2020 at 66 US hospitals in 31 states. The final date of follow-up was January 5, 2021. Patients with MIS-C had fever, inflammation, multisystem involvement, and positive SARS-CoV-2 reverse transcriptase-polymerase chain reaction (RT-PCR) or antibody test results or recent exposure with no alternate diagnosis. Patients with COVID-19 had positive RT-PCR test results and severe organ system involvement.
Main outcomes and measures: Presenting symptoms, organ system complications, laboratory biomarkers, interventions, and clinical outcomes. Multivariable regression was used to compute adjusted risk ratios (aRRs) of factors associated with MIS-C vs. COVID-19.
Results: Of 1116 patients (median age, 9.7 years; 45% female), 539 (48%) were diagnosed with MIS-C and 577 (52%) with COVID-19. Compared with patients with COVID-19, patients with MIS-C were more likely to be 6 to 12 years old (40.8% vs. 19.4%; absolute risk difference [RD], 21.4% [95% CI, 16.1%-26.7%]; aRR, 1.51 [95% CI, 1.33-1.72] vs. 0-5 years) and non-Hispanic Black (32.3% vs. 21.5%; RD, 10.8% [95% CI, 5.6%-16.0%]; aRR, 1.43 [95% CI, 1.17-1.76] vs. White). Compared with patients with COVID-19, patients with MIS-C were more likely to have cardiorespiratory involvement (56.0% vs. 8.8%; RD, 47.2% [95% CI, 42.4%-52.0%]; aRR, 2.99 [95% CI, 2.55-3.50] vs. respiratory involvement), cardiovascular without respiratory involvement (10.6% vs. 2.9%; RD, 7.7% [95% CI, 4.7%-10.6%]; aRR, 2.49 [95% CI, 2.05-3.02] vs. respiratory involvement), and mucocutaneous without cardiorespiratory involvement (7.1% vs. 2.3%; RD, 4.8% [95% CI, 2.3%-7.3%]; aRR, 2.29 [95% CI, 1.84-2.85] vs. respiratory involvement). Patients with MIS-C had higher neutrophil to lymphocyte ratio (median, 6.4 vs. 2.7, P < .001), higher C-reactive protein level (median, 152 mg/L vs. 33 mg/L; P < .001), and lower platelet count (<150 ×103 cells/μL [212/523 [41%] vs. 84/486 [17%], P < .001]). A total of 398 patients (73.8%) with MIS-C and 253 (43.8%) with COVID-19 were admitted to the intensive care unit, and 10 (1.9%) with MIS-C and 8 (1.4%) with COVID-19 died during hospitalization. Among patients with MIS-C with reduced left ventricular systolic function (172/503, 34.2%) and coronary artery aneurysm (57/424, 13.4%), an estimated 91.0% (95% CI, 86.0%-94.7%) and 79.1% (95% CI, 67.1%-89.1%), respectively, normalized within 30 days.
Conclusions and relevance: This case series of patients with MIS-C and with COVID-19 identified patterns of clinical presentation and organ system involvement. These patterns may help differentiate between MIS-C and COVID-19.
Long COVID
| Level 2 |
Buonsenso et al (2021) [Cross-Sectional Study] Preliminary evidence on long COVID in children[30]
20/30 (66.6%) children assessed as part of this cross-sectional study between 60-120 days after initial COVID-19 had at least 1 persisting symptom. 35/68 (27.1%) assessed 120 days or more after diagnosis had at least 1 persisting symptom. Symptoms such as fatigue, muscle and joint pain, headache, insomnia, respiratory problems and palpitations were particularly frequent. The authors assert that an important and unexpected finding is that children with asymptomatic or paucisymptomatic COVID‐19 developed chronic, persisting symptoms, although followed‐up for a relatively short time after the diagnosis.
Limitations of the study include the single‐centre design with a relatively small sample size. All patients were interviewed once, and a control group of children without COVID‐19 was not included.
| Level 4 |
Most children have a mild course of acute COVID-19. Only few mainly non-controlled studies with small sample size have evaluated long-term recovery from SARS-CoV-2 infection in children. The aim of this study was to evaluate symptoms and duration of ‘long COVID’ in children.
METHODS: A nationwide cohort study of 37,522 children aged 0–17 years with RT-PCR verified SARS-CoV-2 infection (response rate 44.9%) and a control group of 78,037 children (response rate 21.3%). An electronic questionnaire was sent to all children from March 24 to May 9, 2021.
RESULTS: Symptoms lasting > 4 weeks were common among both SARS-CoV-2 children and controls. However, SARS-CoV-2 children aged 6–17 years reported symptoms more frequently than the control group (percent difference 0.8%). The most reported symptoms among pre-school children were fatigue (risk difference (RD) 0.05 (CI 0.04–0.06)), loss of smell (RD 0.01 (CI 0.01–0.01)), loss of taste (RD 0.01 (CI 0.01–0.02)) and muscle weakness (RD 0.01 (CI 0.00–0.01)). Among school children the most significant symptoms were loss of smell (RD 0.12 (CI 0.12–0.13)), loss of taste RD (0.10 (CI 0.09–0.10)), fatigue (RD 0.05 (CI 0.05–0.06)), respiratory problems (RD 0.03 (CI 0.03–0.04)), dizziness (RD 0.02 (CI 0.02–0.03)), muscle weakness (RD 0.02 (CI 0.01–0.02)) and chest pain (RD 0.01 (CI 0.01–0.01)). Children in the control group experienced significantly more concentration difficulties, headache, muscle and joint pain, cough, nausea, diarrhea and fever than SARS-CoV-2 infected children. In most children long COVID symptoms resolved within 1–5 months.
Conclusions: Long COVID in children is rare and mainly of short duration.
| Level 4 |
Using data from 4678 children participating in VirusWatch, a household cohort study, the authors estimated the prevalence of persistent symptoms lasting ≥4 weeks as 1.7%, and 4.6% in children with a history of SARS-CoV-2 infection. The median duration of symptoms was 46 days (IQR 32-188). In the 2-11-year-old age group, 1.0% had persistent symptoms. Children 12-17 were more likely to report persistent symptoms (aOR 2.67, 1.56, 4.57). Persistent symptom prevalence was higher in girls, teenagers and children with long-term conditions.
| Level 4 |
This cohort study aimed to describe medium-term clinical outcomes 3–6 months after diagnosis in children with COVID-19 presenting to a tertiary paediatric hospital.
The authors followed children (aged ≤18 years) at a dedicated COVID-19 follow-up clinic at the Royal Children’s Hospital (RCH) in Melbourne, Australia, between March 21, 2020 and March 17, 2021. Children who tested positive for SARS-CoV-2 at the RCH or externally between March 21 and Oct 28, 2020, were referred to the clinic.
The study cohort comprised of 171 children (median age 3 years [IQR 1–8]): 90 (53%) boys and 81 (47%) girls. Most children had mild disease (100 [58%]) or were asymptomatic (61 [36%]), and 9 (5%) children had moderate disease. The few hospital admissions (14 [8%] children) were generally brief and were for observation or fluid rehydration. One (1%) child with complex congenital heart disease had severe COVID-19 pneumonitis with acute respiratory failure. Two (1%) children had post-acute COVID-19 inflammatory conditions temporally associated with SARS-CoV-2: a 7-year-old child with paediatric multisystem inflammatory syndrome who required intensive care management, and an 11-month-old child with Kawasaki disease.
Follow-up data at 3–6 months were available for 151 (88%) of 171 children, of whom 54 (36%) were asymptomatic and 97 (64%) were symptomatic (ie, with mild, moderate, or severe disease) with acute COVID-19. 12 (8%) children had post-acute COVID-19 symptoms, all of whom were symptomatic with acute COVID-19. The most common post-acute COVID-19 symptoms were mild post-viral cough (6 [4%] of 151 children), fatigue (3 [2%] children) or both post-viral cough and fatigue (one [1%] child). The duration of post-viral cough ranged from 3 weeks to 8 weeks and of post-viral fatigue ranged from 6 weeks to 8 weeks from the time of symptom onset. At the most recent review in March, 2021, all 151 children had returned to their baseline health status and post-acute COVID-19 symptoms had resolved. Follow-up data for 20 children were not available; 7 (35%) of these children had asymptomatic COVID-19.
These findings contrast those of studies of COVID-19 in adults, which have identified multisystem complications and a higher prevalence and severity of persistent symptoms.
| Level 4 |
The long-term sequelae of COVID-19 in children remain poorly characterised. This study aimed to assess long-term outcomes in children previously hospitalised with COVID-19 and associated risk factors.
Methods: A prospective cohort study of children (≤18 years old) admitted with confirmed COVID-19 between April 2, 2020 and August 26, 2020. Telephone interviews using the International Severe Acute Respiratory and emerging Infection Consortium (ISARIC) COVID-19 Health and Wellbeing paediatric follow-up survey were carried out. Persistent symptoms (>5 months) were further categorised by system(s) involved.
Findings: 518 of 853 (61%) of eligible children were available for the follow-up assessment and included in the study. Median age was 10.4 years (IQR, 3-15.2) and 270 (52.1%) were girls; median follow-up since hospital discharge was 256 (223-271) days. At the time of the follow-up interview 126 (24.3%) participants reported persistent symptoms among which fatigue (53, 10.7%), sleep disturbance (36, 6.9%,) and sensory problems (29, 5.6%) were the most common. Multiple symptoms were experienced by 44 (8.4%) participants. Risk factors for persistent symptoms were: older age “6-11 years” (OR 2.74 (95% CI 1.37 to 5.75) and “12-18 years” (OR 2.68, 95% CI 1.41 to 5.4); and a history of allergic diseases (OR 1.67, 95% CI 1.04 to 2.67).
Interpretation: A quarter of children experienced persistent symptoms months after hospitalization with acute COVID-19 infection, with almost one in ten experiencing multi-system involvement. Older age and allergic diseases were associated with higher risk of persistent symptoms at follow-up.
| Level 4 |
This Swedish study assessed the extent and type of persistent symptoms in children aged 0–18 years who were admitted to one of the two paediatric hospitals in the Stockholm Region from 13 March to 31 August 2020 due to COVID‐19.
There were 147 SARS‐CoV‐2‐positive children hospitalised during the study period, and 60 were primarily admitted due to COVID‐19. Of these 60 children, 9 fulfilled the criteria of multisystem inflammatory syndrome in children (MIS‐C) and two of these required intensive care. A total of 55 were interviewed and analysed. The authors found that 12/55 (22%) had persistent symptoms and 8/12 had fatigue, which was the most common symptom. There were 6/12 with mild persistent symptoms with an uncertain relationship with COVID‐19, including vague symptoms such as parental reports of poor appetite despite good growth, an infant with a congested nose and intermittent increases in body temperature. A third (4/12), aged 4, 14, 15 and 16 years, had multiple severe symptoms that were possibly related to COVID‐19. All 4 reported fatigue and headache or myalgia, and 3 reported cognitive difficulties. Their median admission was seven days, compared with 4 days for the overall group: 3 had a C‐reactive protein value of more than 200mg/l during their initial illness, and two were diagnosed with MIS‐C. All the severe cases had symptoms that had a major impact on their daily activities, including reduced school attendance and leisure activities.
The groups were too small to determine statistically significant differences, but persistent symptoms seemed higher among children diagnosed with MIS‐C.
A tenth of the 55 children who were hospitalised due to COVID‐19 reported persistent symptoms that were assessed to have a possible association with the SARS‐CoV‐2 infection more than 4 months after their acute illness.
| Level 4 |
Pulmonary complications in adults who recovered from SARS-CoV-2 have been reported even in minimally symptomatic patients. In this study, lung ultrasound (LUS) findings and pulmonary function of children who recovered from an asymptomatic or mildly symptomatic SARS-CoV-2 infection were evaluated. The authors followed up for at least 30 days patients younger than 18 years who recovered from SARS-CoV-2 infection at the Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico, Milan (Italy). All enrolled patients underwent LUS. Airway resistance measured by the interrupter technique test was assessed in subjects aged 4-6 years, whereas forced spirometry and measurement of diffusing capacity of the lungs for carbon monoxide were performed in subjects older than 6 years. To evaluate a possible correlation between pulmonary alterations and immune response to SARS-CoV-2, two semiquantitative enzyme immune assays were used. 16 out of 23 eligible children were enrolled. The median age of enrolled subjects was 7.5 (0.5-10.5) years, with a male to female ratio of 1.7. No subject presented any abnormality on LUS, airway resistance test, forced spirometry, and diffusing capacity of the lungs for carbon monoxide. On the other hand, all subjects presented Ig G against SARS-CoV-2. In contrast in adults, the authors did not detect any pulmonary complications in our cohort. These preliminary observations suggest that children with an asymptomatic or mildly symptomatic SARS-CoV-2 infection might be less prone to developing pulmonary complications than adults.
| Level 4 |
Children can experience SARS-CoV-2 post-viral syndromes, but it is unclear to what extent these individuals are affected by long COVID. Evidence is predominantly limited to select populations without control groups, which does not allow estimating the overall prevalence and burden in a general pediatric population. The authors compared symptoms compatible with long COVID in children and adolescents reported within 6 months after SARS-CoV-2 serologic testing.
This study found a low prevalence of symptoms compatible with long COVID in a randomly selected cohort of children assessed 6 months after serologic testing. 4/109 (4%) seropositive children vs. 28/1246 (2%) seronegative reported at least one symptom lasting beyond 12 weeks.
This study reports the distribution of symptoms compatible with long COVID on a population level; it did not capture severe SARS-CoV-2 infections because they are rare in children. A strength of this study is the population-based seronegative control group. Limitations include the relatively small number of seropositive children, lack of information on the exact time of SARS-CoV-2 infection, possible misclassification of some children with false seropositive results, potential recall bias, parental report of child’s symptoms, lack of information on symptom severity, and non-completion of the questionnaire.
Comorbidities
| Level 1 |
This study aimed to use individual patient data to describe pre-existing factors associated with severe disease, primarily admission to critical care, and death secondary to SARS-CoV-2 infection in children and young people (CYP) in hospital.
Methods: The authors searched PubMed, Europe PubMed Central, Medline and Embase for case series and cohort studies that included all CYP admitted to hospital with ≥30 CYP with SARS-CoV-2 or ≥5 CYP with PIMS-TS or MIS-C. Eligible studies contained (a) details of age, sex, ethnicity or co-morbidities; and (b) an outcome which included admission to critical care, mechanical invasive ventilation, cardiovascular support, or death.
Findings: 81 studies were included, 57 in the meta-analysis (of which 22 provided IPD) and 26 in the narrative synthesis. Most studies had an element of bias in their design or reporting. Sex was not associated with critical care or death. Compared with CYP aged 1-4 years, infants had increased odds of admission to critical care (OR 1.63 (95% CI 1.40-1.90)) and death (OR 2.08 (1.57-2.86)). Odds of death were increased among CYP over 10 years (10-14 years OR 2.15 (1.54-2.98); >14 years OR 2.15 (1.61-2.88)).
Number of comorbid conditions was associated with increased odds of admission to critical care and death for COVID-19 in a dose-related fashion. For critical care admission odds ratios were: 1 comorbidity 1.49 (1.45-1.53); 2 comorbidities 2.58 (2.41-2.75); ≥3 comorbidities 2.97 (2.04-4.32), and for death: 1 comorbidity 2.15 (1.98-2.34); 2 comorbidities 4.63 (4.54-4.74); ≥3 co-morbidities 4.98 (3.78-6.65). Odds of admission to critical care were increased for all co-morbidities apart from asthma (0.92 (0.91-0.94)) and malignancy (0.85 (0.17-4.21)) with an increased odds of death in all co-morbidities considered apart from asthma. Neurological and cardiac comorbidities were associated with the greatest increase in odds of severe disease or death. Obesity increased the odds of severe disease and death independently of other comorbidities.
Interpretation: Hospitalised CYP at greatest vulnerability of severe disease or death from SARS-CoV-2 infection are infants, teenagers, those with cardiac or neurological conditions, or 2 or more comorbid conditions, and those who are obese. Although odds ratios were high, the absolute increase in risk for most comorbidities was small compared to children without underlying conditions.
| Level 1 |
Objective: There is limited information on the severity of COVID-19 infection in children with comorbidities. The authors investigated the effects of pediatric comorbidities on COVID-19 severity by means of a systematic review and meta-analysis of published literature.
Methods: PubMed, Embase, and Medline databases were searched for publications on pediatric COVID-19 infections published January 1 to October 5, 2020. Articles describing at least one child with and without comorbidities, COVID-19 infection, and reported outcomes were included.
Results: 42 studies containing 275,661 children without comorbidities and 9,353 children with comorbidities were included. Severe COVID-19 was present in 5.1% of children with comorbidities, and in 0.2% without comorbidities. Random-effects analysis revealed a higher risk of severe COVID-19 among children with comorbidities than for healthy children; relative risk ratio 1.79 (95% CI 1.27 – 2.51; I2 = 94%). Children with underlying conditions also had a higher risk of COVID-19-associated mortality; relative risk ratio 2.81 (95% CI 1.31 – 6.02; I2 = 82%). Children with obesity had a relative risk ratio of 2.87 (95% CI 1.16 – 7.07; I2 = 36%).
Conclusions: Children with comorbidities have a higher risk of severe COVID-19 and associated mortality than children without underlying disease. Additional studies are required to further evaluate this relationship.
| Level 2 |
Among 121 SARS-CoV-2-associated deaths reported to CDC among persons aged <21 years in the United States during February 12 to July 31, 2020, 63% occurred in males, 10% of decedents were aged <1 year, 20% were aged 1-9 years, 70% were aged 10-20 years, 45% were Hispanic persons, 29% were non-Hispanic Black (Black) persons, and 4% were non-Hispanic American Indian or Alaska Native (AI/AN) persons. Among these 121 decedents, 91 (75%) had an underlying medical condition, 79 (65%) died after admission to a hospital, and 39 (32%) died at home or in the emergency department (ED). Of those who died 25% (n=30) had no medical comorbidities, 75% (n=91) had at least one underlying condition, and 45%(n=54) had two or more conditions. Asthma 28% (n=34), obesity 27%(n=33), neurological developmental 22% (n=26), and cardiovascular 18%(n=22) were the underlying conditions reported. These data show that nearly 3/4 of SARS-CoV-2-associated deaths among infants, children, adolescents and young adults have occurred in persons aged 10-20 years, with a disproportionate%age among young adults aged 18-20 years and among Hispanics, Blacks, AI/ANs, and persons with underlying medical conditions.
| Level 4 |
Objectives: To describe the characteristics of hospitalized children with SARS-CoV-2 in New York City metropolitan area.
Patients and methods: This was a multicenter, retrospective cohort study at 4 hospitals comprising 82 hospitalized children (0-21 years) who tested positive for SARS-CoV-2 after symptoms and risk screening between March 1 and May 10, 2020. The authors subdivided patients on the basis of their admission to acute or critical care units and by age groups. Further sub-analyses were performed between patients requiring respiratory support or no respiratory support.
Results: 23 (28%) patients required critical care. 29 (35%) patients required respiratory support, with 9% needing mechanical ventilation, and 1 requiring extracorporeal support. All patients survived to discharge. Children with any comorbidity were more likely to require critical care (70% vs 37%, P = .008), with obesity as the most common risk factor for critical care (63% vs 28%, P = .02). Children with asthma were more likely to receive respiratory support (28% vs 8%, P = .02), with no difference in need for critical care (P = .26). Children admitted to critical care had higher rates of renal dysfunction at presentation (43% vs 10%, P = .002).
Conclusions: Children with comorbidities (obesity and asthma in particular) were at increased risk for critical care admission and/or need for respiratory support. Children with renal dysfunction at presentation were more likely to require critical care.
| Level 4 |
To assess the relevance of systematic SARS-CoV-2 screening of all children admitted to hospital, the authors conducted a prospective multicenter study including 438 consecutive hospitalized children. A symptom-based SARS-CoV-2 testing strategy failed to identify 45% (95% CI, 24%-68%) of hospitalized children infected by SARS-CoV-2. SARS-CoV-2 PCR was positive for 22/438 children (5.0%). Patients with underlying conditions were not more frequently infected by SARS-CoV-2 than other children (9/209, 4.3% vs. 13/229, 5.7%, respectively, p=0.63), nor were patients with chronic immunosuppressive treatment (2/33, 6.1% vs. 20/405, 4.9%, p=1.0). The authors suggest that to limit intra-hospital transmission, a systematic screening of children admitted to hospital should be considered.
Collateral Health Impacts
| Level 1 |
Emerging research suggests that the global prevalence of child and adolescent mental illness has increased considerably during COVID-19. However, substantial variability in prevalence rates have been reported across the literature.
Objective: To ascertain more precise estimates of the global prevalence of child and adolescent clinically elevated depression and anxiety symptoms during COVID-19; to compare these rates with pre-pandemic estimates; and to examine whether demographic (eg, age, sex), geographical (ie, global region), or methodological (eg, pandemic data collection time point, informant of mental illness, study quality) factors explained variation in prevalence rates across studies.
Data sources: Four databases were searched (PsycInfo, Embase, MEDLINE, and Cochrane Central Register of Controlled Trials) from January 1, 2020, to February 16, 2021, and unpublished studies were searched in PsycArXiv on March 8, 2021, for studies reporting on child/adolescent depression and anxiety symptoms.
Main outcomes and measures: Prevalence rates of clinically elevated depression and anxiety symptoms in youth.
Results: Random-effect meta-analyses were conducted. Twenty-nine studies including 80 879 participants met full inclusion criteria. Pooled prevalence estimates of clinically elevated depression and anxiety symptoms were 25.2% (95% CI, 21.2%-29.7%) and 20.5% (95% CI, 17.2%-24.4%), respectively. Moderator analyses revealed that the prevalence of clinically elevated depression and anxiety symptoms were higher in studies collected later in the pandemic and in girls. Depression symptoms were higher in older children.
Conclusions and relevance: Pooled estimates obtained in the first year of the COVID-19 pandemic suggest that 1 in 4 young people globally are experiencing clinically elevated depression symptoms, while 1 in 5 young people are experiencing clinically elevated anxiety symptoms. These pooled estimates, which increased over time, are double the pre-pandemic estimates.
| Level 4 |
To assess changes in mental health-related ED visits among US children aged <18 years, data from CDC’s National Syndromic Surveillance Program (NSSP) from January 1 through October 17, 2020, were compared with those collected during the same period in 2019. During weeks 1-11 (January 1-March 15, 2020), the average reported number of children’s mental health-related ED visits overall was higher in 2020 than in 2019, whereas the proportion of children’s mental health-related visits was similar. Beginning in week 12 (March 16) the number of mental health-related ED visits among children decreased 43% concurrent with the widespread implementation of COVID-19 mitigation measures; simultaneously, the proportion of mental health-related ED visits increased sharply beginning in mid-March 2020 (week 12) and continued into October (week 42) with increases of 24% among children aged 5-11 years and 31% among adolescents aged 12-17 years, compared with the same period in 2019. The increased proportion of children’s mental health-related ED visits during March-October 2020 might be artificially inflated as a consequence of the substantial decrease in overall ED visits during the same period and variation in the number of EDs reporting to NSSP. However, these findings provide initial insight into children’s mental health in the context of the COVID-19 pandemic and highlight the importance of continued monitoring of children’s mental health throughout the pandemic, ensuring access to care during public health crises, and improving healthy coping strategies and resiliency among children and families.
| Level 4 |
To evaluate pandemic-related changes in weight in school-aged youths, the authors compared the body mass index (BMI; calculated as weight in kilograms divided by height in meters squared) of youths aged 5 to 17 years during the pandemic in 2020 with BMI in the same period before the pandemic in 2019.
Methods: A retrospective cohort study using Kaiser Permanente Southern California (KPSC) electronic health record data. Youths between 5 and 17 years with continuous health care coverage were included if they had an in-person visit with at least 1 BMI measure before the pandemic (March 2019-January 2020) and another BMI measure during the pandemic (March 2020-January 2021 with at least 1 BMI after June 16, 2020, ie, about 3 months into the pandemic). Youths with complex chronic conditions were excluded. Outcomes were the absolute distance of a youth’s BMI from the median BMI for sex and age, weight adjusted for height, and overweight or obesity (≥85th or ≥95th%ile of BMI for age, respectively). Models were adjusted for sex, race and ethnicity, state-subsidized health insurance, neighborhood education, neighborhood income, and number of parks in the census tract. Mixed-effects models also included BMI-for-age class at baseline.
Results: The cohort (n = 191 509) was racially and ethnically diverse (10.4% Asian and Pacific Islander, 50.4% Hispanic, 7.0% non-Hispanic Black, and 25.3% non-Hispanic White) with 49.6% girls, a mean age of 11.6 years (SD, 3.8 years), and a mean pre-pandemic BMI of 20.7 (SD, 5.4). The study population was comparable with the overall pediatric population with regard to sex, age, race and ethnicity, and socioeconomic factors. Before the pandemic, 38.9% of youths in the cohort were overweight or obese compared with 39.4% in the KPSC source population.
Youths gained more weight during the COVID-19 pandemic than before the pandemic. The greatest change in the distance from the median BMI for age occurred among 5- through 11-year-olds with an increased BMI of 1.57, compared with 0.91 among 12- through 15-year-olds and 0.48 among 16- through 17-year-olds. Adjusting for height, this translates to a mean gain among 5- through 11-year-olds of 2.30 kg (95% CI, 2.24-2.36 kg) more during the pandemic than during the reference period, 2.31 kg (95% CI, 2.20-2.44 kg) more among 12- through 15-year-olds, and 1.03 kg (95% CI, 0.85-1.20 kg) more among 16- through 17-year-olds. Overweight or obesity increased among 5- through 11-year-olds from 36.2% to 45.7% during the pandemic, an absolute increase of 8.7% and relative increase of 23.8% compared with the reference period. The absolute increase in overweight or obesity was 5.2% among 12- through 15-year-olds (relative increase, 13.4%) and 3.1% (relative increase, 8.3%) among 16- through 17-year-olds. Most of the increase among youths aged 5 through 11 years and 12 through 15 years was due to an increase in obesity.
Discussion: Significant weight gain occurred during the COVID-19 pandemic among youths in KPSC, especially among the youngest children. These findings, if generalizable to the US, suggest an increase in pediatric obesity due to the pandemic.
| Level 4 |
During the COVID-19 pandemic, children and adolescents spent more time than usual away from structured school settings, and families who were already disproportionally affected by obesity risk factors might have had additional disruptions in income, food, and other social determinants of health. As a result, children and adolescents might have experienced circumstances that accelerated weight gain, including increased stress, irregular mealtimes, less access to nutritious foods, increased screen time, and fewer opportunities for physical activity. CDC used data from IQVIA’s Ambulatory Electronic Medical Records database to compare longitudinal trends in body mass index (BMI, kg/m2) among a cohort of 432,302 persons aged 2-19 years before and during the COVID-19 pandemic (January 1, 2018-February 29, 2020 and March 1, 2020-November 30, 2020, respectively). Between the pre-pandemic and pandemic periods, the rate of BMI increase approximately doubled, from 0.052 (95% CI = 0.051-0.052 to 0.100 (95% CI = 0.098-0.101) kg/m2/month (ratio = 1.93 [95% CI = 1.90-1.96]). Persons aged 2-19 years with overweight or obesity during the pre-pandemic period experienced significantly higher rates of BMI increase during the pandemic period than did those with healthy weight. These findings underscore the importance of efforts to prevent excess weight gain during and following the COVID-19 pandemic, as well as during future public health emergencies, including increased access to efforts that promote healthy behaviors. These efforts could include screening by health care providers for BMI, food security, and social determinants of health, increased access to evidence-based pediatric weight management programs and food assistance resources, and state, community, and school resources to facilitate healthy eating, physical activity, and chronic disease prevention.
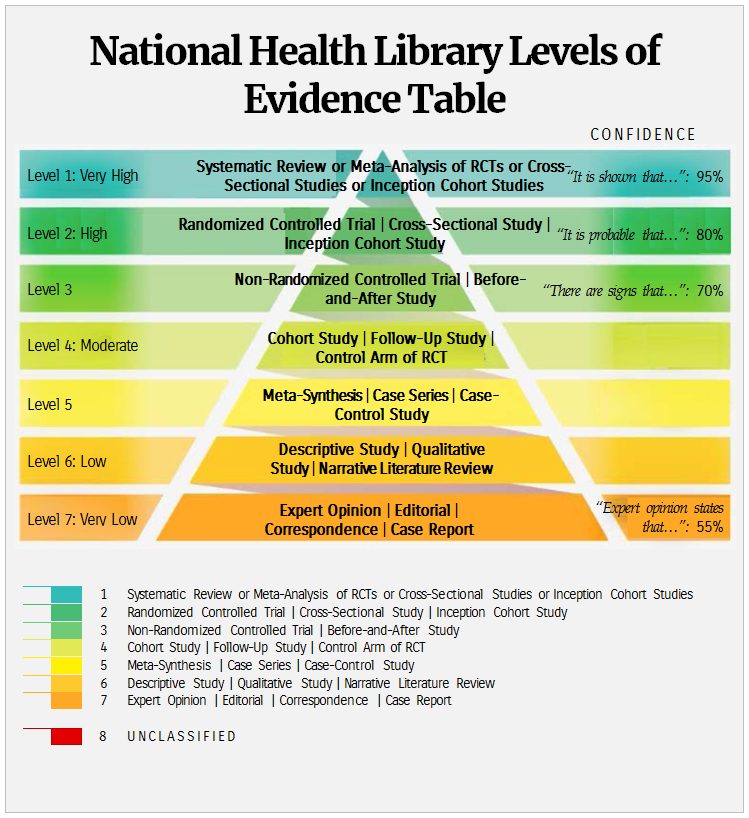
References
[1] Delahoy MJ, Ujamaa D, Whitaker M, et al. Hospitalizations Associated with COVID-19 Among Children and Adolescents — COVID-NET, 14 States, March 1, 2020–August 14, 2021. MMWR Morb Mortal Wkly Rep 2021;70:1255–1260. DOI: http://dx.doi.org/10.15585/mmwr.mm7036e2 [accessed 25/11/21]
[2] Siegel DA, [et al] (2021) Trends in COVID-19 Cases, Emergency Department Visits, and Hospital Admissions Among Children and Adolescents Aged 0-17 Years – United States, August 2020-August 2021. MMWR Morb Mortal Wkly Rep. 2021 Sep 10;70(36):1249-1254. doi: 10.15585/mmwr.mm7036e1. Erratum in: MMWR Morb Mortal Wkly Rep. 2021 Sep 24;70(38):1355. PMID: 34499628; PMCID: PMC8437056. [accessed 25/11/21]
[3] BMJ Best Practice (2021) Coronavirus disease 2019 (COVID-19). Accessed 28 November, 2021.
[4] UpToDate (2021) UpToDate (2021) COVID-19: Clinical manifestations and diagnosis in children. Accessed 25 November, 2021.
[5] Jones (2021) SARS-CoV-2 Epidemiology in children [PowerPoint Presentation] Available at https://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2021-11-2-3/03-COVID-Jefferson-508.pdf [accessed 25/11/21]
[6] Smith, C. [et al.] (2021) Deaths in children and young people in England after SARS-CoV-2 infection during the first pandemic year. Nat Med (2021). https://doi.org/10.1038/s41591-021-01578-1 [accessed 25/11/21]
[7] Woodruff RC, [et al.] (2021) COVID-NET surveillance team. Risk Factors for Severe COVID-19 in Children. Pediatrics. 2021 Oct 22:e2021053418. doi: 10.1542/peds.2021-053418. Epub ahead of print. PMID: 34686570. [accessed 25/06/21]
[8] Levin Z, Choyke K, Georgiou A, Sen S, Karaca-Mandic P. Trends in Pediatric Hospitalizations for Coronavirus Disease 2019. JAMA Pediatr. 2021;175(4):415–417. doi:10.1001/jamapediatrics.2020.5535 [accessed 25/11/21]
[9] Molteni, E. [et al] (2021) Illness characteristics of COVID-19 in children infected with the SARS-CoV-2 Delta variant medRxiv 2021.10.06.21264467; doi: https://doi.org/10.1101/2021.10.06.21264467 [accessed 25/11/21]
[10] Ward, JL [et al] (2021) Risk factors for intensive care admission and death amongst children and young people admitted to hospital with COVID-19 and PIMS-TS in England during the first pandemic year. medRxiv 2021.07.01.21259785; doi: https://doi.org/10.1101/2021.07.01.21259785 [accessed 25.11.21]
[11] Preston LE, [et al.] (2021) Characteristics and Disease Severity of US Children and Adolescents Diagnosed With COVID-19. JAMA Netw Open. 2021 Apr 1;4(4):e215298. doi: 10.1001/jamanetworkopen.2021.5298. PMID: 33835179; PMCID: PMC8035649. [accessed 25/11/21]
[12] Dawood FS, [et al.] (2021) Incidence Rates, Household Infection Risk, and Clinical Characteristics of SARS-CoV-2 Infection Among Children and Adults in Utah and New York City, New York. JAMA Pediatr. 2022 Jan 1;176(1):59-67. doi: 10.1001/jamapediatrics.2021.4217. PMID: 34623377; PMCID: PMC8501415. [accessed 25/11/21]
[13] Graff K, [et al.] (2021) Risk Factors for Severe COVID-19 in Children. Pediatr Infect Dis J. 2021 Apr 1;40(4):e137-e145. doi: 10.1097/INF.0000000000003043. PMID: 33538539. [accessed 25/11/21]
[14] Parcha, V. [et al] (2021). A retrospective cohort study of 12,306 pediatric COVID-19 patients in the United States. Sci Rep 11, 10231 (2021). https://doi.org/10.1038/s41598-021-89553-1 [accessed 25/11/21]
[15] Madewell ZJ, [et al] (2021) Factors Associated With Household Transmission of SARS-CoV-2: An Updated Systematic Review and Meta-analysis. JAMA Netw Open. 2021 Aug 2;4(8):e2122240. doi: 10.1001/jamanetworkopen.2021.22240. PMID: 34448865; PMCID: PMC8397928. [accessed 25/11/21]
[16] Irfan, O., [et al] (2021) Risk of infection and transmission of SARS-CoV-2 among children and adolescents in households, communities and educational settings: A systematic review and meta-analysis. Journal of global health vol. 11 05013. 17 Jul. 2021, doi:10.7189/jogh.11.05013 [accessed 25/11/21]
[17] Viner, RM [et al] (2021) Susceptibility to SARS-CoV-2 Infection Among Children and Adolescents Compared With Adults: A Systematic Review and Meta-analysis. JAMA Pediatr. 2021 Feb 1;175(2):143-156. doi: 10.1001/jamapediatrics.2020.4573. Erratum in: JAMA Pediatr. 2021 Feb 1;175(2):212. PMID: 32975552; PMCID: PMC7519436. [accessed 25/11/21]
[18] UpToDate (2021) UpToDate (2021) COVID-19: Clinical manifestations and diagnosis in children. Accessed 25 November, 2021.
[19] NCIRS (2021) COVID-19 Delta variant in schools and early childhood education and care services in NSW, Australia: 16 June to 31 July 2021 Available at https://www.ncirs.org.au/COVID-19-delta-variant-schools-and-early-childhood-education-and-care-services-nsw-australia-16 [accessed 25/11/21]
[20] Paul LA, [et al] (2021) Association of Age and Pediatric Household Transmission of SARS-CoV-2 Infection. JAMA Pediatr. 2021 Nov 1;175(11):1151-1158. doi: 10.1001/jamapediatrics.2021.2770. PMID: 34398179; PMCID: PMC8369380. [accessed 25/11/21]
[21] Chun, June Young [et al] (2021) Age-Varying Susceptibility to the Delta Variant (B.1.617.2) of SARS-CoV-2. Available at SSRN: https://ssrn.com/abstract=3951778 or http://dx.doi.org/10.2139/ssrn.3951778 [accessed 25/11/21]
[22] Hoste L, [et al.] (2021) Multisystem inflammatory syndrome in children related to COVID-19: a systematic review. Eur J Pediatr. 2021 Jul;180(7):2019-2034. doi: 10.1007/s00431-021-03993-5. Epub 2021 Feb 18. PMID: 33599835; PMCID: PMC7890544. [accessed 25/11/21]
[23] UpToDate (2021) UpToDate (2021) COVID-19: Multisystem inflammatory syndrome in children (MIS-C): Clinical features, evaluation, and diagnosis. Accessed
[24] Flood J, [et al.] (2021) Paediatric multisystem inflammatory syndrome temporally associated with SARS-CoV-2 (PIMS-TS): Prospective, national surveillance, United Kingdom and Ireland, 2020. Lancet Reg Health Eur. 2021 Apr;3:100075. doi: 10.1016/j.lanepe.2021.100075. Epub 2021 Mar 22. PMID: 34027512; PMCID: PMC8132575. [accessed 25/11/21]
[25] Dawood FS, [et al.] (2021) Incidence Rates, Household Infection Risk, and Clinical Characteristics of SARS-CoV-2 Infection Among Children and Adults in Utah and New York City, New York. JAMA Pediatr. 2022 Jan 1;176(1):59-67. doi: 10.1001/jamapediatrics.2021.4217. PMID: 34623377; PMCID: PMC8501415. [accessed 25/11/21]
[26] Payne, AB. [et al.] (2021) Incidence of Multisystem Inflammatory Syndrome in Children Among US Persons Infected With SARS-CoV-2. JAMA Netw Open. 2021 Jun 1;4(6):e2116420. doi: 10.1001/jamanetworkopen.2021.16420. PMID: 34110391; PMCID: PMC8193431. [accessed 25/11/21]
[27] Lee EH, [et al.] (2021) Race/Ethnicity Among Children With COVID-19-Associated Multisystem Inflammatory Syndrome. JAMA Netw Open. 2020 Nov 2;3(11):e2030280. doi: 10.1001/jamanetworkopen.2020.30280. PMID: 33252688; PMCID: PMC7705594. [accessed 25/11/21]
[28] Brizuela, M [et al.] (2021) Influence of sex on disease severity in children with COVID-19 and Multisystem Inflammatory Syndrome in Latin America. medRxiv 2021.02.07.21251212; doi: https://doi.org/10.1101/2021.02.07.21251212 [accessed 25/11/21]
[29] Feldstein LR, [et al.] (2021) Characteristics and Outcomes of US Children and Adolescents With Multisystem Inflammatory Syndrome in Children (MIS-C) Compared With Severe Acute COVID-19. JAMA. 2021 Mar 16;325(11):1074-1087. doi: 10.1001/jama.2021.2091. PMID: 33625505; PMCID: PMC7905703. [accessed 25/11/21]
[30] Buonsenso D, [et al] (2021) Preliminary evidence on long COVID in children. Acta Paediatr. 2021 Jul;110(7):2208-2211. doi: 10.1111/apa.15870. Epub 2021 Apr 18. PMID: 33835507; PMCID: PMC8251440. [accessed 25/11/21]
[31] Borch, L., [et al.] (2021) Long COVID symptoms and duration in SARS-CoV-2 positive children — a nationwide cohort study. Eur J Pediatr (2022). https://doi.org/10.1007/s00431-021-04345-z [accessed 25/11/21]
[32] Miller, F., [et al.] (2021) Prevalence of persistent symptoms in children during the COVID-19 pandemic: evidence from a household cohort study in England and Wales. medRxiv 2021.05.28.21257602; doi: https://doi.org/10.1101/2021.05.28.21257602 [accessed 25/11/21]
[33] Say D, [et al.] (2021) Post-acute COVID-19 outcomes in children with mild and asymptomatic disease. Lancet Child Adolesc Health. 2021 Jun;5(6):e22-e23. doi: 10.1016/S2352-4642(21)00124-3. Epub 2021 Apr 21. PMID: 33891880; PMCID: PMC8057863. [accessed 25/11/21]
[34] Osmanov IM, [et al] (2021) Risk factors for long COVID in previously hospitalised children using the ISARIC Global follow-up protocol: A prospective cohort study. Eur Respir J. 2021 Jul 1:2101341. doi: 10.1183/13993003.01341-2021. Epub ahead of print. PMID: 34210789; PMCID: PMC8576804. [accessed 25/11/21]
[35] Sterky E, [et al.] (2021) Persistent symptoms in Swedish children after hospitalisation due to COVID-19. Acta Paediatr. 2021 Sep;110(9):2578-2580. doi: 10.1111/apa.15999. Epub 2021 Jul 3. PMID: 34157167; PMCID: PMC8444740. [accessed 25/11/21]
[36] Bottino I, [et al.] (2021) Can Asymptomatic or Non-Severe SARS-CoV-2 Infection Cause Medium-Term Pulmonary Sequelae in Children? Front Pediatr. 2021 May 13;9:621019. doi: 10.3389/fped.2021.621019. PMID: 34084763; PMCID: PMC8168403. [accessed 25/11/21]
[37] Radtke T, [et al] (2021) Long-term Symptoms After SARS-CoV-2 Infection in Children and Adolescents. JAMA. 2021 Jul 15;326(9):869–71. doi: 10.1001/jama.2021.11880. Epub ahead of print. PMID: 34264266; PMCID: PMC8283661. [accessed 25/11/21]
[38] Harwood, R., [et al] (2021) Which children and young people are at higher risk of severe disease and death after SARS-CoV-2 infection: a systematic review and individual patient meta-analysis. medRxiv 2021.06.30.21259763; doi: https://doi.org/10.1101/2021.06.30.21259763 [accessed 25/11/21]
[39] Tsankov BK, [et al] (2021) COVID-19 Infection and Pediatric Comorbidities: A Systematic Review and Meta-Analysis. Int J Infect Dis. 2021 Feb;103:246-256. doi: 10.1016/j.ijid.2020.11.163. Epub 2020 Nov 20. PMID: 33227520; PMCID: PMC7679116. [accessed 25/11/21]
[40] Bixler D, [et al] (2021) SARS-CoV-2-Associated Deaths Among Persons Aged <21 Years – United States, February 12-July 31, 2020. MMWR Morb Mortal Wkly Rep. 2020 Sep 18;69(37):1324-1329. doi: 10.15585/mmwr.mm6937e4. PMID: 32941417. [accessed 25/11/21]
[41] Verma S, [et al] (2021) Characteristics of Hospitalized Children With SARS-CoV-2 in the New York City Metropolitan Area. Hosp Pediatr. 2021 Jan;11(1):71-78. doi: 10.1542/hpeds.2020-001917. Epub 2020 Oct 8. PMID: 33033078. [accessed 25/11/21]
[42] Poline J, [et al] (2021) Systematic Severe Acute Respiratory Syndrome Coronavirus 2 Screening at Hospital Admission in Children: A French Prospective Multicenter Study. Clin Infect Dis. 2021 Jun 15;72(12):2215-2217. doi: 10.1093/cid/ciaa1044. PMID: 32710743; PMCID: PMC7454330. [accessed 25/11/21]
[43] Racine N, [et al] (2021) Global Prevalence of Depressive and Anxiety Symptoms in Children and Adolescents During COVID-19: A Meta-analysis. JAMA Pediatr. 2021 Nov 1;175(11):1142-1150. doi: 10.1001/jamapediatrics.2021.2482. PMID: 34369987; PMCID: PMC8353576. [accessed 25/11/21]
[44] Leeb RT, [et al] (2021) Mental Health-Related Emergency Department Visits Among Children Aged <18 Years During the COVID-19 Pandemic – United States, January 1-October 17, 2020. MMWR Morb Mortal Wkly Rep. 2020 Nov 13;69(45):1675-1680. doi: 10.15585/mmwr.mm6945a3. PMID: 33180751; PMCID: PMC7660659. [accessed 25/11/21]
[45] Woolford SJ, [et al] (2021) Changes in Body Mass Index Among Children and Adolescents During the COVID-19 Pandemic. JAMA. 2021;326(14):1434–1436. doi:10.1001/jama.2021.15036 [accessed 25/11/21]
[46] Lange SJ, [et al] (2021) Longitudinal Trends in Body Mass Index Before and During the COVID-19 Pandemic Among Persons Aged 2-19 Years – United States, 2018-2020. MMWR Morb Mortal Wkly Rep. 2021 Sep 17;70(37):1278-1283. doi: 10.15585/mmwr.mm7037a3. Erratum in: MMWR Morb Mortal Wkly Rep. 2021 Sep 24;70(38):1355. PMID: 34529635; PMCID: PMC8445379. [accessed 25/11/21]
Produced by the members of the National Health Library and Knowledge Service Evidence Team†. Current as at November 2021. This evidence summary collates the best available evidence at the time of writing and does not replace clinical judgement or guidance. Emerging literature or subsequent developments in respect of COVID-19 may require amendment to the information or sources listed in the document. Although all reasonable care has been taken in the compilation of content, the National Health Library and Knowledge Service Evidence Team makes no representations or warranties expressed or implied as to the accuracy or suitability of the information or sources listed in the document. This evidence summary is the property of the National Health Library and Knowledge Service and subsequent re-use or distribution in whole or in part should include acknowledgement of the service.
Denise Duffy, Librarian, University Hospital Galway [Author]; Isabelle Delaunois Librarian, University Hospital Limerick [Author]; Brendan Leen, Area Library Manager, HSE South [Editor]; NIAC Sub-Group Contributors: Philippa White, Aileen Conway, Catherine Crowe, Geraldine Casey, Margaret Brennan, Oisin Hennigan

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License