
How long does immunity last after COVID-19 vaccination? Does immunity wane faster in certain sub-populations? How safe and effective are booster doses of COVID-19 vaccine?
The following information resources have been selected by the National Health Library and Knowledge Service Evidence Virtual Team in response to a question from the National Immunisation Advisory Committee (NIAC). The resources are listed in our estimated order of relevance to practicing healthcare professionals confronted with this scenario in an Irish context. In respect of the evolving global situation and rapidly changing evidence base, it is advised to use hyperlinked sources in this document to ensure that the information you are disseminating to the public or applying in clinical practice is the most current, valid and accurate. For further information on the methodology used in the compilation of this document ¾ including a complete list of sources consulted ¾ please see our National Health Library and Knowledge Service Summary of Evidence Protocol.
Download Full Summary of Evidence (PDF)
Main Points
- Data from vaccination campaigns and ongoing studies have not fully answered the question of how long protection from COVID-19 vaccines will last. Data on the impact of new SARS-CoV-2 variants are limited, but are expected soon. Data from an ongoing multinational pivotal efficacy study showed that despite a gradually declining trend in vaccine efficacy, the Pfizer-BioNTech vaccine had an acceptable safety profile and was highly efficacious in preventing COVID-19 up to 6 months post-vaccination.
- In Britain, the Joint Committee on Vaccination and Immunisation (JCVI)4 recommend an additional dose of COVID-19 vaccine for those who are severely immunosuppressed. To date, the JCVI has not recommended booster doses for other groups.
- In the United States, the Advisory Committee on Immunization Practices (ACIP) recommend that individuals with certain immunocompromising conditions who received a two-dose mRNA vaccine series should receive a third dose of the same vaccine. Immunocompromising conditions that warrant a third dose include active use of chemotherapy for cancer; hematologic malignancies; hematopoietic stem cell or solid organ transplant; advanced or untreated HIV infection with CD4 cell count <200 cells/microL; moderate or severe primary immunodeficiency disorder; and use of immunosuppressive medications.
- Patients receiving dialysis may mount an attenuated immune response to COVID-19 vaccination. Standard vaccination series provide insufficient protection to some haemodialysis patients; immune monitoring and adaption of vaccination protocols may be considered.
- Individuals aged ³60 years will need to be closely monitored and may require earlier booster vaccinations to ensure long-lasting immunity and protection against infection.
- Solid-organ transplant recipients may develop a substantially lower immunological response to mRNA-based vaccines. Data indicate that administration of a third dose of vaccine to solid-organ transplant recipients significantly improved immunogenicity.
- There is significant heterogeneity of humoral immune response to COVID-19 vaccines among immunosuppressed individuals, highlighting an urgent need to optimize COVID-19 prevention in these patients.
Summary of Evidence
The European Medicines Agency (EMA) and European Centre for Disease Prevention and Control (ECDC)3state that it is currently too early to confirm if or when a booster dose for COVID-19 vaccines will be needed. Data from vaccination campaigns and ongoing studies do not yet indicate how long protection from the vaccines will last, or clarify the potential impact of SARS-CoV-2 variants. Data from an ongoing multinational pivotal efficacy study showed that despite a gradually declining trend in vaccine efficacy, the Pfizer-BioNTech vaccine had an acceptable safety profile and was highly efficacious in preventing COVID-19 up to 6 months post-vaccination6. Real-world effectiveness data are of particular interest to supplement data from clinical trials.
Preliminary results from an ongoing clinical trial of a modified Moderna vaccine administered as a booster 6 months after the standard two-dose series showed that the third dose induced increases in antibody neutralization titers to the wild type and variant strains B.1.351 and P.111.
In Britain, the Joint Committee on Vaccination and Immunisation (JCVI)4 recommend that any potential booster programme should begin in September in order to maximise protection for those who are most vulnerable to serious COVID-19 in advance of the winter months; should run concurrent with influenza vaccination programmes; and should be offered in two stages, with immunosuppressed individuals, those living in residential care homes for older persons, adults over 70 years, adults over 16 years who are considered clinically extremely vulnerable, and frontline health and social care workers prioritized for early vaccination. To date [August 2021], the JCVI has only recommended an additional dose of vaccination for immunosuppressed individuals.
In the United States, the Advisory Committee on Immunization Practices (ACIP)5 recommend that individuals with certain immunocompromising conditions who received a two-dose mRNA vaccine series should receive a third dose of the same vaccine. Immunocompromising conditions that warrant a third dose include active use of chemotherapy for cancer; hematologic malignancies; hematopoietic stem cell or solid organ transplant; advanced or untreated HIV infection with CD4 cell count <200 cells/microL; moderate or severe primary immunodeficiency disorder; and use of immunosuppressive medications. Several other countries have made similar recommendations regarding immunocompromised individuals; Israel has decided to offer a booster vaccination to the entire eligible population37.
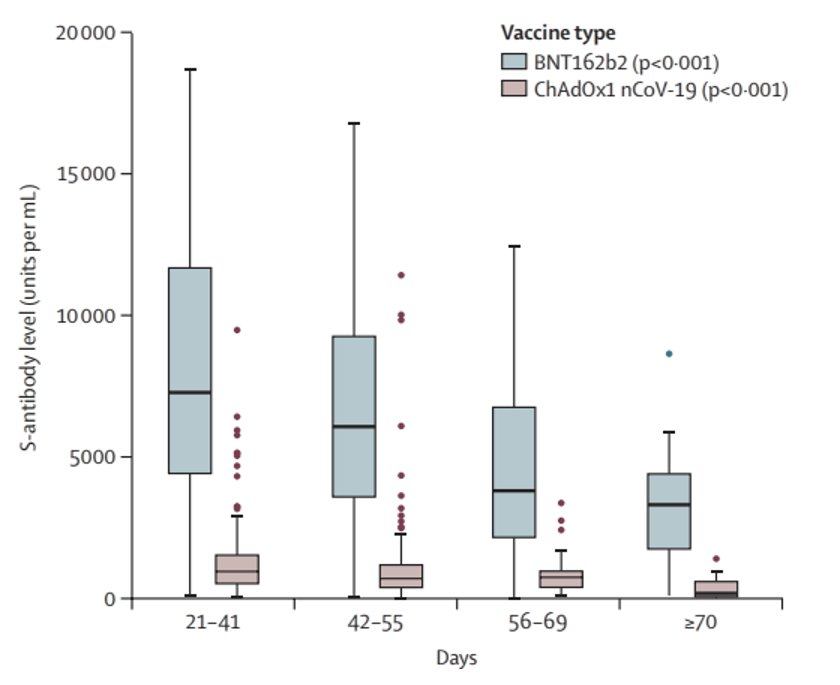
Shrotri et al9 observed waning S-antibody at defined time-points after a second dose of both the AstraZeneca and Pfizer-BioNTech vaccines, with levels reducing by about 5-fold for the AstraZeneca and two-fold for the Pfizer-BioNTech vaccine after ³70 days. This trend remained consistent when results were stratified by sex, age, and clinical vulnerability.
Nace et al8 found that healthier older adults mounted detectable antibody responses when vaccinated with mRNA-based COVID-19 vaccines. Data indicated that some degree of immunity was present during the immediate period following vaccination; however, the authors caution that protective effects remain to be determined in larger studies as clinical protection is afforded by ongoing adaptive immunity, which is known to decrease in older adults8, 24.
Anand et al7 state that patients receiving dialysis may mount an attenuated immune response to COVID-19 vaccination. Longlune et al25 suggest that among chronic dialysis patients, a third vaccine dose may be required in non-responders to a two-dose series. Stumpf et al12 found that 8 weeks after the second dose of an mRNA-based vaccine, SARS-CoV-2 seroconversion efficacy in dialysis patients was similar to controls (> 95%), but markedly impaired in kidney transplant recipients (42%). Immunosuppressive drug number and type, as well as vaccine type, were found to be major determinants of seroconversion failure in both dialysis and transplant patients. Similarly, Espi et al27 conclude that standard vaccination series provide insufficient protection to some haemodialysis patients, and suggest that immune monitoring and adaption of vaccination protocols are indicated12, 27.
Müller et al19 observed lower frequencies of neutralizing antibodies in older Pfizer-BioNTech vaccine recipients. The authors submit that the ³60 years age-group may need to be closely monitored and may require earlier re-vaccination and/or an increased vaccine dose to ensure longer-lasting immunity and protection against infection. Pannus et al20 submit that adapted vaccination regimens may be needed to provide optimal protection against COVID-19 to vulnerable populations such as nursing home residents. Among older haemodialysis patients, Jahn et al18 found that antibody responses to SARS-CoV-2 vaccination negatively correlated with age, leading to significantly lower antibody titers in patients ³60 years.
In reports of transplant recipients who received a third dose of mRNA vaccines, seroconversion rates were higher after the additional dose, although approximately 50% to 70% who were seronegative after two doses remained seronegative5.
Rabinowich et al13 found that liver transplant recipients developed a substantially lower immunological response to the Pfizer-BioNTech vaccine. Factors influencing serological antibody response included older age, renal function and immunosuppressive medications. Schramm et al14 observed poor humoral and T-cell response to the Pfizer-BioNTech vaccine among cardiothoracic transplant recipients. Kamar et al22 demonstrated that administration of a third dose of the Pfizer-BioNTech vaccine to solid-organ transplant recipients significantly improved immunogenicity. Administration of a third dose of the Pfizer-BioNTech vaccine to solid-organ transplant recipients significantly improved immunogenicity. Similarly, Benotmane et al23 found that a third dose of the Moderna vaccine induced a serologic response in 49% of kidney transplant recipients who did not respond after two doses.
In interim analysis of an ongoing observational prospective cohort study, Haidar et al15 found that seropositivity for the presence of IgG against SARS-CoV-2 was significantly lower among immunocompromised patients. The authors’ findings demonstrate the heterogeneity of humoral immune response to COVID-19 vaccines based on underlying immunosuppressive condition, and highlight an urgent need to optimize and individualize COVID-19 prevention in these patients15, 16.
Shroff et al17 observed immune response to a two-dose mRNA-based vaccine series in patients with solid tumors on immunosuppressive cancer therapy at levels similar to those of a control cohort after the first immunization. The authors propose that a third immunization might elevate antibody responses in cancer patients to levels seen in healthy individuals after a second dose. Re et al26 demonstrated that a third dose of the Pfizer-BioNTech vaccine stimulated humoral immune response among patients with lymphoid malignancies, in particular patients with multiple myeloma who had higher anti-S baseline titer after the second dose, and those with no anti-CD20 treatment history within a year.
Although both diabetics and non-diabetics displayed a robust response to the two-dose Pfizer-BioNTech vaccination series, Ali et al21 observed that diabetics had 13.86 BAU/ml (95%CI: −27.08 to −0.64BAU/ml, p=0.041), less IgG antibodies and 4.42% (95%CI: −8.53 to −0.32%, p=0.036) less neutralizing antibodies than non-diabetics.
Irish and/or International Guidance
| Level 1 |
In France, the Conseil d’Orientation de la Stratégie Vaccinale recommends that a third dose of an mRNA COVID-19 vaccine is necessary for people who are severely immunocompromised: solid organ transplant recipients; recent bone marrow transplant recipients; dialysis patients; and patients with autoimmune conditions requiring strong immunosuppressive therapy such as anti-CD20 monoclonal antibodies and antimetabolites.
A third dose should be given at least 4 weeks after the second dose and as soon as possible after that interval. A decision on vaccinating patients with chronic renal failure or cancer or receiving other immunosuppressive therapies will be made at a later stage.
| Level 1 |
In France, the Conseil Scientifique COVID-19 recommend a booster dose to those aged 80+ years ¾ whether living in a nursing home or at home ¾ and to immunocompromised individuals. The Conseil acknowledge that data underpinning the recommendation are limited, but argue that initial studies showing earlier waning of antibodies in these sub-populations and the potential impact on the health system suggest that a booster dose is a reasonable proposition.
| Level 1 |
Will a booster dose be needed after completing the recommended vaccination course?
The European Medicines Agency (EMA) and European Centre for Disease Prevention and Control (EDCD) affirm that vaccination remains one of the best protective measures against COVID-19. Recommendations for vaccination are in place in all European Union (EU) member states, and roll-out of vaccination is ongoing. The EMA and ECDC urge EU citizens to get vaccinated and adhere to the recommended dose series. Vaccination is particularly important in the context of transmission the Delta variant of SARS-CoV-2; of the need to protect citizens, especially those at risk of severe COVID-19; and of the impetus to open up societies and relax restrictions.
The EMA and ECDC state that it is currently too early to confirm if and/or when a booster dose for COVID-19 vaccines will be needed. Data from vaccination campaigns and ongoing studies do not yet indicate how long protection from vaccines will last or clarify the potential impact of SARS-CoV-2 variants. Real-world effectiveness data from Europe and other parts of the world are of particular interest to supplement data from clinical trials. The EMA is also engaging with vaccine developers to coordinate submission of these data so that regulatory steps toward permitting the use of a booster dose may be completed as soon as possible.
| Level 1 |
In a situation where social mixing and social contact return toward pre-pandemic norms, the Joint Committee on Vaccination and Immunisation (JCVI) in Britain state that it is expected that winter 2021/’22 will be the first season when SARS-CoV-2 will co-circulate alongside other respiratory viruses, including seasonal influenza. Seasonal influenza and SARS-CoV-2 viruses have the potential to add substantially to the winter pressures usually faced by the National Health Service (NHS), particularly if infection waves from both viruses coincide. The timing and magnitude of potential influenza and SARS-CoV2 infection waves for winter 2021/’22 are currently unknown.
In the view of the JCVI, the primary objective of a 2021 COVID-19 booster programme is to reduce the occurrence of serious COVID-19 disease. Any potential booster programme should begin in September 2021 in order to maximise protection for those who are most vulnerable to serious COVID-19 in advance of the winter months. Influenza vaccines are also delivered in September/October, and the JCVI considers that a synergistic approach to the delivery of COVID-19 and influenza vaccination would support delivery and maximise uptake of both vaccines.
Any potential COVID-19 booster programme should be offered in two stages:
- Stage 1. The following persons should be offered a third dose COVID-19 booster vaccine and the annual influenza vaccine as soon as possible from September 2021:
- adults aged 16 years and over who are immunosuppressed
- those living in residential care homes for older adults
- all adults aged 70 years or over
- adults aged 16 years and over who are considered clinically extremely vulnerable
- frontline health and social care workers
- Stage 2. The following persons should be offered a third dose COVID-19 booster vaccine as soon as practicable after Stage 1, with equal emphasis on deployment of the influenza vaccine where eligible:
- all adults aged 50 years and over
- adults aged 16 to 49 years who are in an influenza or COVID-19 at-risk group
- adult household contacts of immunosuppressed individuals
As most younger adults will only receive their second COVID-19 vaccine dose in late summer, the JCVI will consider the benefits of booster vaccination in this age-group at a later time when more data are available. The initial objective for winter 2021/’22 is for persons in Stage 1 and Stage 2 above to receive their influenza and COVID-19 vaccines in good time.
Vaccines designed specifically against variants of concern will not be available in time for booster re-vaccination during autumn 2021. The use of variant vaccines will be considered by the JCVI in due course.
Additional scientific data will become available which will require further consideration by the JCVI ahead of any final advice. These include:
- further data on the safety and effectiveness of COVID-19 vaccines
- clinical trial and real-world effectiveness data on the durability of protection beyond 6 months
- clinical trial data on immune responses following booster re-vaccination
- clinical trial data on reactogenicity and immunogenicity following booster re-vaccination with the same or alternative COVID-19 vaccines
- clinical trial data on other COVID-19 vaccines in development
- the emergence of any new variants of concern
- data on the duration of immunity following a primary course
- data on the effects of on-going SARS-CoV2 circulation in the population and its potential to confer long-term public health benefits
Point of Care Tools
| Level 2 |
UpToDate (2021) COVID-19: Vaccines to prevent SARS-CoV-2 infection[5]
See Section: ADDITIONAL VACCINE DOSE
The authors agree with recommendations from the Advisory Committee on Immunization Practices (ACIP) in the United States that individuals with certain immunocompromising conditions who received a two-dose mRNA vaccine series should receive a third dose of the same vaccine. The emergency use authorization for the mRNA vaccines was updated to include a third dose to be given at least 28 days after the second dose for such individuals.
Immunocompromising conditions that warrant a third dose include active use of chemotherapy for cancer, hematologic malignancies, hematopoietic stem cell or solid organ transplant, advanced or untreated HIV infection with CD4 cell count <200 cells/microL, moderate or severe primary immunodeficiency disorder, and use of immunosuppressive medications. Several other countries including France, Germany and Israel have made similar recommendations. If an immunocompromised patient receives an additional vaccine dose, other protective measures should be continued as immune response may still not be optimal.
In reports of transplant recipients who received a third dose of mRNA vaccines, seroconversion rates were higher after the additional dose, although approximately 50% to 70% who were seronegative after two doses remained seronegative. Adverse effects were similar to those reported after prior doses. Longitudinal follow-up and evaluation of cellular immune responses are needed to more completely characterize the impact of additional vaccine doses.
Irish and/or International Literature
| Level 2 |
Thomas et al (2021) Six Month Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine[6]
The BNT162b2 Pfizer-BioNTech COVID-19 vaccine is highly efficacious against COVID-19 and is currently authorized for emergency use or conditional approval globally. At the time of authorization, data beyond two months post-vaccination were not yet available.
Methods: In an ongoing placebo-controlled, observer-blinded, multinational pivotal efficacy study, 44,165 ≥16-year-old participants and 2,264 12-15-year-old participants were randomized to receive two doses, 21 days apart, of 30 µg BNT162b2 or placebo. Study endpoints reported are vaccine efficacy (VE) against laboratory-confirmed COVID-19 and safety data up to 6 months post-vaccination.
Results: BNT162b2 continued to be safe and well tolerated. Few participants had adverse events leading to study withdrawal. VE against COVID-19 was 91% (95% CI 89.0%-93.2%) through up to 6 months of follow-up among evaluable participants and irrespective of previous SARS-CoV-2 infection. VE of 86%-100% was seen across countries and in populations with diverse characteristics of age, sex, race/ethnicity and COVID-19 risk factors in participants without evidence of previous SARS-CoV-2 infection. VE against severe disease was 97% (95% CI 80.3%−99.9%). In South Africa, where the SARS-CoV-2 variant of concern B.1.351 (Beta) was predominant, 100% (95% CI 53.5, 100.0) VE was observed.
Conclusion: With up to 6 months of follow-up and despite a gradually declining trend in vaccine efficacy, BNT162b2 had an acceptable safety profile and was highly efficacious in preventing COVID-19. Note: Only 24 vaccine and 128 placebo recipients were followed for greater than 4 months after the second vaccine dose. The 12-15 age group were recruited later, so data were only available for 2 months post-vaccination.
| Level 2 |
Anand et al (2021) Antibody Response to COVID-19 Vaccination in Patients Receiving Dialysis[7]
Patients receiving dialysis may mount impaired responses to COVID-19 vaccination.
Methods: The authors report antibody response to vaccination from 1140 patients without, and 493 patients with pre-vaccination SARS-CoV-2 RBD antibody. Commercially available assays (Siemens) were used to test remainder plasma monthly in association with vaccination date and type, and assess prevalence of absent total receptor binding antibody, and absent or attenuated (index value < 10) semiquantitative receptor binding domain IgG index values. Poisson regression was used to evaluate risk factors for absent or attenuated response to vaccination.
Results: Among patients who were seronegative vs. seropositive before vaccination, 62% and 56% were ≥65 years old, 20% and 24% were Hispanic, and 22% and 23% were Black. Median IgG index values rose steadily over time, and were higher among seropositive than seronegative patients after completing vaccination (150 [25th, 75th percentile 23.2, 150.0] vs. 41.6 [11.3, 150.0]). Among 610 patients who completed vaccination (assessed ≥14 days later, median 29 days later), the prevalence of absent total RBD response, and absent and attenuated semiquantitative IgG response was 4.4% (95% CI 3.1, 6.4%), 3.4% (2.4, 5.2%), and 14.3% (11.7, 17.3%), respectively. Risk factors for absent or attenuated response included longer vintage of end-stage kidney disease, and lower pre-vaccination serum albumin.
Conclusions: More than one in five patients receiving dialysis had evidence of an attenuated immune response to COVID19 vaccination.
| Level 2 |
Objective: COVID-19 disproportionately impacts residents in long-term care facilities. The objective of the present study was to quantify the presence and magnitude of antibody response in vaccinated older adult residents at assisted living, personal care and independent living communities.
Design: A cross-sectional quality improvement study was conducted from March 15 to April 1, 2021 in the greater Pittsburgh region.
Setting and population: Participants were older adult residents at assisted living, personal care and independent living communities, who received mRNA-based COVID-19 vaccine. Conditions that impair immune responses were exclusionary criteria.
Methods: Sera were collected to measure IgG anti-SARS-CoV-2 antibody level with reflex to total anti-SARS-CoV-2 immunoglobulin levels, and blinded evaluation of SARS-CoV-2 pseudovirus neutralization titers. Descriptive statistics, Pearson correlation coefficients and multiple linear regression analysis evaluated relationships between factors potentially associated with antibody levels. Spearman correlations were calculated between antibody levels and neutralization titers.
Results: All participants (N = 70) had received two rounds of vaccination and were found to have antibodies with wide variation in relative levels. Antibody levels trended lower in males, advanced age, current use of steroids, and longer length of time from vaccination. Pseudovirus neutralization titer levels were strongly correlated (P < .001) with Beckman Coulter antibody levels [D614 G NT50, rs = 0.91; B.1.1.7 NT50, rs = 0.91].
Conclusions and implications: Higher functioning, healthier older adults mounted detectable antibody responses when vaccinated with mRNA-based COVID-19 vaccines. Data indicate some degree of immunity is present during the immediate period following vaccination. However, protective effects remain to be determined in larger studies as clinical protection is afforded by ongoing adaptive immunity, which is known to decrease in older adults. This study provides important preliminary results on level of population risk in older adult residents at assisted living, personal care and independent living communities to inform reopening strategies. The authors caution that the results are not likely to be translatable for nursing home residents.
| Level 2 |
Vaccines based on the Spike glycoprotein of SARS-CoV-2 are being rolled out globally in order to control transmission and limit morbidity and mortality associated with COVID-19. Current evidence indicates strong immunogenicity and high short-term efficacy for the Pfizer-BioNTech (BNT162b2) and AstraZeneca (ChAdOx1) COVID-19 vaccines. Both vaccines are delivered through a prime/boost strategy, and many countries have used dose intervals longer than 3–4 weeks, anticipating to maximise first-dose coverage and immunogenicity. With continued high global incidence and potential for more transmissible SARS-CoV-2 variants, data on longer-term vaccine efficacy and antibody dynamics in infection-naive individuals are essential in order to clarify the need for further booster doses.
To identify early indications of waning antibody levels to the Spike protein (S-antibody) after a two-dose vaccination series, the authors conducted a cross-sectional analysis of fully vaccinated adults aged ≥18 years who submitted capillary blood samples for Virus Watch, a longitudinal community cohort study in England and Wales. Sera were tested using Elecsys Anti-SARS-CoV-2 S and N electro-chemiluminescent immunoassays (Roche Diagnostics, Basel, Switzerland); the S assay targets total antibodies to the S1 subunit of the Spike protein (range 0.4–25,000 units per mL [U/mL]), whereas the N assay targets total antibodies to the full-length Nucleocapsid protein, which was interpreted as a proxy for previous SARS-CoV-2 infection (specificity 99.8% [99.3%–100%]). Serological results were mapped with demographic and clinical information collected at enrolment, and with weekly self-reported vaccination status.
605 adults submitted a valid sample on June 14–15, 2021. 321 (53%) of 605 participants were women, and the median age was 63 years (IQR 58–67). Of 605 participants, 186 (31%) were categorised as clinically vulnerable, 117 (19%) as clinically extremely vulnerable, and 302 (50%) as not clinically vulnerable. Participants contributed a single sample, taken 14–154 days after their second vaccine dose (median 42 days [IQR 30–53]). 197 (33%) of 605 samples were from BNT162b2 vaccines and 405 (67%) samples were from ChAdOx1 vaccines; vaccine type was missing for three (<1%) participants. The median interval between first and second doses was 77 days (IQR 70–78).
Participants with previous infection (N-seropositive; n=47) had a median S-antibody level of 9091 U/mL (IQR 3143 to 16 135), with 2.5-fold lower median levels for ChAdOx1 (median 5179 [IQR 2432.5 to 9513.5]) than BNT162b2 (median 13 025 [9091 to ≥25 000]). N-seronegative individuals had 7-fold lower average S-antibody levels than N-seropositive individuals (median 1257 U/mL [616 to 3526]) and 6-fold lower median levels were seen after ChAdOx1 (median 864 [IQR 481 to 1395]) compared to BNT162b2 (median 5311 [3133 to 8829]) within this infection-naive group.
The authors examined the distribution of S-antibody levels for confirmed N-seronegative samples 14–20 days, 21–41 days, 42–55 days, 56–69 days, and 70 days or more after second vaccination to infer the general trend in antibody levels with time, stratified by vaccine type, with p values derived from non-parametric tests for trend. A significant trend of declining S-antibody levels was seen with time for both ChAdOx1 (p<0·001) and BNT162b2 (p<0·001), with levels reducing by about 5-fold for ChAdOx1, and by about two-fold for BNT162b2, between 21–41 days and 70 days or more after the second dose. This trend remained consistent when results were stratified by sex, age, and clinical vulnerability. For BNT162b2, S-antibody levels reduced from a median of 7506 U/mL (IQR 4925–11 950) at 21–41 days, to 3320 U/mL (1566–4433) at 70 or more days. For ChAdOx1, S-antibody levels reduced from a median of 1201 U/mL (IQR 609–1865) at 0–20 days to 190 U/mL (67–644) at 70 or more days.
In the context of recent advice in support of booster vaccinations from the Joint Committee on Vaccination and Immunisation (JCVI), and given the potentially rapid S-antibody decline suggested by these data, the authors propose that heterologous regimens, which preliminary data suggest elicit stronger antibody and T-cell responses, might provide more durable immunity and greater protection against emerging variants. However, the ultimate effect of different dose intervals and various heterologous combinations on clinical outcomes remain important unanswered questions.
The authors further propose that the ethical basis for universal booster dose deployment in high-income settings should be carefully considered in the context of widening global vaccine inequities.
Figure: levels of antibody against the Spike glycoprotein of SARS-CoV-2 (S-antibody) at defined time-points after second dose of vaccination in individuals with no previous infection, stratified by vaccine type
| Level 2 |
COVID-19 vaccine supply shortages are causing concerns about compromised immunity in some countries as the interval between first and second doses extends. Conversely, countries with no supply constraints are considering administering a third dose. The authors assessed the persistence of immunogenicity after a single dose, the immunity after an extended interval between the first and second doses of ChAdOx1 nCoV-19 (AZD1222), and the response to a third dose as a late booster.
Methods: Volunteers aged 18-55 years who were enrolled in a Phase I/II or Phase II/III clinical trial of ChAdOx1 nCoV-19 and had received either a single dose or two doses of 5×10 10 viral particles were invited back for vaccination. Reactogenicity and immunogenicity of a delayed second dose or a third dose are reported.
Findings: Antibody titres after a single dose and measured on day 362 remain higher than the titres measured on day 0 (62.61 EU; 95% CI 47.43-82.64 vs. 1 EU 95% CI 1-16). 30 participants received a late second dose of ChAdOx1 nCoV-19 (median 44 weeks after first dose), antibody titres were higher in those with a longer interval between first and second doses (median EU for 8-12, 15-25, and 44-46 weeks were 923 [IQR 525-1764], 1860 [IQR 917-4934] and 3738 [IQR 1824-6625] respectively). 90 participants received a third dose and antibody titres were significantly higher following a third dose (FRNT50 612 [IQR 351-920]) when compared with the response 28 days after a second dose (FRNT 50 319 [IQR 176-591]. T-cell responses were also boosted after a third dose. Reactogenicity after a late second dose or a third dose was lower than reactogenicity after a first dose.
Interpretation: A longer delay before the second dose of ChAdOx1 nCoV-19 leads to an increased antibody titre after the second dose. A third dose of ChAdOx1 nCoV-19 induces antibodies to a level that correlate with high efficacy after second dose and boosts T-cell responses.
| Level 2 |
The mRNA-1273 (Moderna) prototype vaccine showed 94% efficacy in prevention of symptomatic COVID-19 disease in a phase III clinical trial. Recently, SARS-CoV-2 variants have emerged which have shown decreased susceptibility to neutralization by vaccine-induced antibody, most notably the B.1.351 variant, although the overall impact on vaccine efficacy remains to be determined. In addition, recent evidence of waning antibody levels after infection or vaccination point to the need for periodic boosting of immunity. Here, the authors present the preliminary evaluation of a clinical study on the use of the prototype mRNA-1273 or modified COVID-19 mRNA vaccines, designed to target emerging SARS-CoV-2 variants as booster vaccines in participants previously vaccinated approximately 6 months earlier with two doses of the prototype vaccine, mRNA-1273. The modified vaccines include a monovalent mRNA-1273.351 encoding for the S protein found in the B.1.351 variant and multivalent mRNA-1273.211 comprising a 1:1 mix of mRNA-1273 and mRNA-1273.351. As single 50 µg booster vaccinations, both mRNA-1273 and mRNA-1273.351 had acceptable safety profiles and were immunogenic. Antibody neutralization titers against B.1.351 and P.1 variants measured by SARS-CoV-2 pseudovirus neutralization (PsVN) assays before the booster vaccinations, approximately 6 to 8 months after the primary series, were low or below the assay limit of quantification, although geometric mean titers vs. the wild-type strain remained above levels likely to be protective. Two weeks after the booster vaccinations, titers against the wild-type original strain, B.1.351 and P.1 variants increased to levels similar to or higher than peak titers after the primary series vaccinations. Although both mRNA-1273 and mRNA-1273.351 boosted neutralization of the wild-type original strain, and B.1.351 and P.1 variants, mRNA-1273.351 appeared to be more effective at increasing neutralization of the B.1.351 virus vs. a boost with mRNA-1273. The vaccine trial is ongoing and boosting of clinical trial participants with the multivalent mRNA-1273.211 is currently being evaluated.
| Level 4 |
Dialysis and kidney transplant patients are vulnerable populations for COVID-19 related disease and mortality.
Methods: A prospective study exploring the eight-week time course of specific cellular (interferon-γ release assay and flow cytometry) or/and humoral immune responses (ELISA) to SARS-CoV-2 boost vaccination in more than 3100 participants ¾ including medical personnel, dialysis patients and kidney transplant recipients ¾ using mRNA vaccines BNT162b2 or mRNA-1273.
Results: SARS-CoV-2-vaccination induced seroconversion efficacy in dialysis patients was similar to medical personnel (> 95%), but markedly impaired in kidney transplant recipients (42%). T-cellular immunity largely mimicked humoral results. Major risk factors of seroconversion failure were immunosuppressive drug number and type, and vaccine type. Seroconversion rates induced by mRNA-1273 compared to BNT162b2 vaccine were 97% to 88% (p < 0.001) in dialysis and 49% to 26% in transplant patients, respectively. Specific IgG directed against the new binding domain of the Spike protein (RDB) were significantly higher in dialysis patients vaccinated by mRNA-1273 (95%) compared to BNT162b2 (85%, p < 0.001). Vaccination appeared safe and highly effective, demonstrating an almost complete lack of symptomatic COVID-19 disease after boost vaccination as well as ceased disease incidences during third pandemic wave in dialysis patients.
Conclusion: Dialysis patients exhibit a remarkably high seroconversion rate of 95% after boost vaccination, while humoral response is impaired in the majority of transplant recipients. Immunosuppressive drug number and type as well as vaccine type are major determinants of seroconversion failure in both dialysis and transplant patients suggesting immune monitoring and adaption of vaccination protocols.
| Level 4 |
Two SARS-CoV-2 mRNA vaccines were approved to prevent COVID-19 infection, with reported vaccine efficacy of 95%. Liver transplant (LT) recipients are at risk of lower vaccine immunogenicity and were not included in the registration trials. The authors assessed vaccine immunogenicity and safety among the LT sub-population.
Methods: LT recipients followed at the Tel-Aviv Sourasky Medical Center and healthy volunteers were tested for SARS-CoV-2 IgG antibodies directed against the Spike-protein (S) and Nucleocapsid-protein (N) 10-20 days after receiving the second Pfizer-BioNTech BNT162b2 SARS-CoV-2 vaccine dose. Information regarding vaccine side-effects and clinical data was collected from patients and medical records.
Results: 80 LT recipients were enrolled. Mean age was 60 years and 30% were female. 25 healthy volunteer controls were younger (mean age 52.7 years, p = 0.013) and mostly female (68%, p = 0.002). All participants were negative for IgG N-protein serology, indicating immunity did not result from prior COVID-19 infection. All controls were positive for IgG S-protein serology. Immunogenicity among LT recipients was significantly lower with positive serology in only 47.5% (p <0.001). Antibody titer was also significantly lower in the LT group (mean 95.41 AU/ml vs. 200.5 AU/ml in controls, p <0.001). Predictors for negative response among LT recipients were older age, lower estimated glomerular filtration rate, and treatment with high dose steroids and mycophenolate mofetil. No serious adverse events were reported in either group.
Conclusion: LT recipients developed substantially lower immunological response to the Pfizer-BioNTech SARS-CoV-2 mRNA-based vaccine. Factors influencing serological antibody response include older age, renal function and immunosuppressive medications.
| Level 4 |
Objectives: Immunocompromised patients have been excluded from studies of SARS-CoV-2 mRNA vaccines. The immune response to vaccines against other infectious agents has been shown to be blunted in such patients. The authors aimed to analyze the humoral and cellular response to prime-boost vaccination with the BNT162b2 vaccine (Pfizer-BioNTech) in cardiothoracic transplant recipients.
Methods and results: A total of 50 transplant patients [1-3 years post heart (42), lung (7), or heart-lung (1) transplant, mean age 55 ± 10 years] and a control group of 50 healthy staff members were included. Blood samples were analysed 21 days after the prime and the boosting dose, respectively, to quantify anti-SARS-CoV-2 Spike protein (S) immunoglobulin titres (Abbott, Euroimmun and RocheElecsys Immunoassays) and the functional inhibitory capacity of neutralizing antibodies (Genscript). To test for a specific T-cell response, heparinized whole blood was stimulated with SARS-CoV-2 specific peptides, covering domains of the viral Spike, nucleocapsid and membrane protein, and the interferon-γ release was measured (QuantiFERON Monitor ELISA, Qiagen). The vast majority of transplant patients (90%) showed neither a detectable humoral nor a T-cell response three weeks after the completed two-dose BNT162b2 vaccination. These results are in sharp contrast to the robust immunogenicity seen in the control group: 98% exhibited seroconversion after the prime dose already, with a further significant increase of IgG titres after the booster dose (average > tenfold increase), a more than 90% inhibition capability of neutralizing antibodies as well as evidence of T-cell responsiveness.
Conclusions: The findings of poor immune responses to a two-dose BNT162b2 vaccination in cardiothoracic transplant patients have a significant impact for organ transplant recipients specifically, and possibly for immunocompromised patients in general.
| Level 4 |
Immunocompromised patients were excluded from COVID-19 vaccine clinical trials. The objective of the present study was to measure antibody responses, levels, and neutralization capability after COVID-19 vaccination among immunocompromised patients and compare against those of immunocompetent healthcare workers.
This is an interim analysis of an ongoing observational prospective cohort study which launched on April 14, 2021 across Western Pennsylvania. Participants were healthy healthcare workers (HCWs) and immunocompromised patients who had completed their COVID-19 vaccination series. Individuals with a history of COVID-19 were not eligible. Serum was collected to measure for the presence of IgG against the SARS-CoV-2 Spike protein using a semi-quantitative assay. Antibody levels were available for comparison. A quasi-random subset of patients was selected for pseudovirus neutralization assays. Seropositivity with 95% Clopper-Pearson exact confidence intervals and distribution of antibody levels were measured. To identify risk factors for seronegativity, clinical characteristics were univariately compared between antibody reactive and non-reactive individuals within the immunocompromised group.
107 HCWs and 489 immunocompromised patients were enrolled. Compared to HCWs, seropositivity was significantly lower (p<.001) among immunocompromised patients with solid organ transplant (SOT), autoimmune, hematological malignancies, and solid tumors (HCW=98.1%; SOT=37.2%; autoimmune=83.8%; hematological malignancies=54.7%; and solid tumor=82.4%, p < 0.05). Over 94% of patients with Human Immunodeficiency Virus were seropositive. Among seropositive patients, antibody levels were much lower among SOT (4.5 [2.1,13.1], p=.020). Neutralization titers tightly correlated with antibody levels (Spearman r = 0.91, p < 0.0001).
The authors’ findings demonstrate the heterogeneity of humoral immune response to COVID-19 vaccines based on underlying immunosuppressive condition and highlight an urgent need to optimize and individualize COVID-19 prevention in these patients; and also have implications on public health guidance, particularly given revised Centers for Disease Control and Prevention recommendations permitting vaccinated individuals to cease masking and social distancing in most settings. Future studies are warranted to determine assessment of cellular immunity, longitudinal measurement of immune responses, and the safety and efficacy of revaccination.
| Level 4 |
As SARS-CoV-2 vaccination coverage increases in the United States, there is a need to understand the real-world effectiveness against severe COVID-19 and among people at increased risk for poor outcomes.
Methods: In a multicenter case-control analysis of US adults hospitalized March 11 – May 5, 2021, the authors evaluated vaccine effectiveness to prevent COVID-19 hospitalizations by comparing odds of prior vaccination with an mRNA vaccine (Pfizer-BioNTech or Moderna) between cases hospitalized with COVID-19 and hospital-based controls who tested negative for SARS-CoV-2.
Results: Among 1210 participants, median age was 58 years, 22.8% were Black, 13.8% were Hispanic, and 20.6% had immunosuppression. SARS-CoV-2 lineage B.1.1.7 was the most common variant (59.7% of sequenced viruses). Full vaccination (receipt of two vaccine doses ≥14 days before illness onset) had been received by 45/590 (7.6%) cases and 215/620 (34.7%) controls. Overall vaccine effectiveness was 86.9% (95% CI: 80.4 to 91.2%). Vaccine effectiveness was similar for Pfizer-BioNTech and Moderna vaccines, and highest in adults aged 18-49 years (97.3%; 95% CI: 78.9 to 99.7%). Among 45 patients with vaccine-breakthrough COVID hospitalizations, 44 (97.8%) were ≥50 years old and 20 (44.4%) had immunosuppression. Vaccine effectiveness was lower among patients with immunosuppression (59.2%; 95% CI: 11.9 to 81.1%) than without immunosuppression (91.3%; 95% CI: 85.5 to 94.7%).
Conclusion: During March-May 2021, SARS-CoV-2 mRNA vaccines were highly effective for preventing COVID-19 hospitalizations among US adults. SARS-CoV-2 vaccination was beneficial for patients with immunosuppression, but effectiveness was lower in the immunosuppressed population.
| Level 4 |
Vaccines against SARS-CoV-2 have shown high efficacy, but immunocompromised participants were excluded from controlled clinical trials. The authors evaluated immune responses to the Pfizer-BioNTech mRNA vaccine in solid tumor patients (n=52) on active cytotoxic anti-cancer therapy. These responses were compared to a control cohort that also received the Pfizer-BioNTech vaccine (n=50). Using live SARS-CoV-2 assays, neutralizing antibodies were detected in 67% and 80% of cancer patients after the first and second immunizations, respectively, with a 3-fold increase in median titers after the booster. Similar trends were observed in serum antibodies against the receptor-binding domain (RBD) and S2 regions of Spike protein, and in IFNγ+ Spike-specific T cells. The magnitude of each of these responses was diminished relative to the control cohort. The authors therefore quantified RBD- and Spike S1-specific memory B cell subsets as predictors of anamnestic responses to viral exposures or additional immunizations. After the second vaccination, Spike-specific plasma cell-biased memory B cells were observed in most cancer patients at levels similar to those of the control cohort after the first immunization. These data suggest that a third immunization might elevate antibody responses in cancer patients to levels seen in healthy individuals after a second dose. Trials should be conducted to test these predictions.
| Level 4 |
mRNA-based SARS-CoV-2 vaccines offer a preventive strategy against severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) infections that is of interest in the care of patients on hemodialysis (HDPs). The authors measured humoral immune responses in 72 HDPs after standard vaccination with two doses of the mRNA-based SARS-CoV-2 vaccine BNT162b2 (Pfizer-BioNTech). Antibody responses were evaluated with an anti-SARS-CoV-2 IgG ChemiLuminescent ImmunoAssay (CLIA) two weeks after the second dose. In addition, SARS-CoV-2 IgG was determined in a control of 16 healthy healthcare workers (HCWs). The control group of HCWs showed a strong antibody response with a median (MD (Q1; Q3)) antibody titer of 800.0 AU/mL (520.5; 800.0). In comparison to HCWs, HDPs under 60 years of age responded equally (597.0 AU/mL (410.5; 800.0), p = 0.051). However, the antibody responses of the HDPs negatively correlated with age (r2 = 0.2954 p < 0.0001), leading to significantly lower antibody titers in HDPs over 60 years (280.0 AU/mL (45.7; 477.0), p < 0.0001). To thoroughly understand the immunogenicity of the new mRNA-based vaccines in HDPs, longitudinal data on the effectiveness and durability of antibody responses are needed. Modifications of immunization schedules should be considered in HDPs with low or without antibody responsiveness after standard vaccination in order to boost immune reactivity and prolong protective effects in these vulnerable patients
| Level 4 |
Real-life data on immune responses elicited in the most vulnerable group of vaccinated individuals over 80 years of age is still underrepresented despite prioritization in vaccination campaigns.
Methods: A cohort study with two age-groups, young vaccinees below the age of 60 and older vaccinees over the age of 60, to compare their antibody responses to the first and second dose of the Pfizer-BioNTech BNT162b2 COVID-19 vaccination.
Results: A majority of participants in both groups produced specific IgG antibody titers against SARS-CoV-2 Spike protein. Titers were significantly lower in the older age-group. Although the increment of antibody levels after the second immunization was higher in older individuals, the absolute mean titer of the older age-group remained lower than the younger age-group. After the second vaccination, 31.3% of the older age-group had no detectable neutralizing antibodies in contrast to the younger group, in which only 2.2% had no detectable neutralizing antibodies.
Conclusion: These data showed differences between the antibody responses raised after the first and second BNT162b2 vaccination, in particular lower frequencies of neutralizing antibodies in the older age-group. The authors submit that the ³60 years age-group may need to be closely monitored and may require earlier re-vaccination and/or an increased vaccine dose to ensure longer-lasting immunity and protection against infection.
| Level 4 |
Residents of nursing homes are at high risk of COVID-19 related morbidity and death and may respond poorly to vaccination because of old age and frequent comorbidities.
Methods: 40 residents and 40 staff members either naive or previously infected with SARS-CoV-2 were recruited in two nursing homes in Belgium before immunization with two doses of 30µg BNT162b2 mRNA vaccine at day 0 and day 21. Binding antibodies (Ab) to SARS-CoV-2 receptor binding domain (RBD), Spike domains S1 and S2, RBD Ab avidity, and neutralizing Ab against SARS-CoV-2 wild type and B.1.351 variant were assessed at days 0, 21, 28, and 49.
Results: SARS-CoV-2 naive residents had lower Ab responses to the BNT162b2 mRNA vaccination than naive staff. These poor responses involved lower levels of IgG to all domains of the vaccine antigen, lower avidity of RBD IgG, and lower levels of Ab neutralizing the vaccine strain. No naive resident had detectable neutralizing Ab to the B.1.351 variant. High and comparable Ab responses were observed in residents and staff previously infected with SARS-CoV-2. Clustering analysis revealed that poor vaccine responders not only included naive residents but also naive staff, emphasizing the heterogeneity of responses to mRNA vaccination in the general population.
Conclusions: The poor Ab responses to mRNA vaccination observed in infection naive residents and in some naive staff members of nursing homes suggest suboptimal protection against breakthrough infection, especially with variants of concern. Adapted vaccination regimens may be needed to provide optimal protection against COVID-19 to vulnerable populations.
| Level 4 |
Given their increased susceptibility to COVID-19, the question arises whether individuals with type-2 diabetes mellitus (T2DM) and other metabolic conditions can respond effectively to mRNA-based vaccines. The authors aimed to evaluate the levels of anti-SARS-CoV-2 IgG and neutralizing antibodies in people with T2DM and/or other metabolic risk factors compared to the general population. The present study included 262 individuals vaccinated with two doses of the BNT162b2 (Pfizer–BioNTech) mRNA vaccine. Both T2DM and non-diabetic individuals had a robust response to vaccination as demonstrated by their high antibody titers. However, both SARS-CoV-2 IgG and neutralizing antibodies titers were lower in people with T2DM. Their levels were 154±49.1 vs. 138±59.4BAU/mL for IgG and 87.1±11.6 vs. 79.7±19.5% for neutralizing antibodies in individuals without diabetes compared to those with T2DM, respectively. In a multiple linear regression adjusted for individual characteristics, comorbidities, previous COVID-19 infection, and duration since second vaccine dose, diabetics had 13.86 BAU/ml (95%CI: −27.08 to −0.64BAU/ml, p=0.041) less IgG antibodies and 4.42% (95%CI: −8.53 to −0.32%, p=0.036) less neutralizing antibodies than non-diabetics. Hypertension and obesity did not show significant changes in antibody titers. Taken together, both type-2 diabetic and non-diabetic individuals elicited strong immune responses to SARS-CoV-2 BNT162b2 mRNA vaccine; nonetheless, lower levels were seen in people with diabetes. Continuous monitoring of the antibody levels might be a good indicator to guide personalized needs for further booster shots to maintain adaptive immunity.
| Level 4 |
Kamar et al (2021) Three Doses of an mRNA COVID-19 Vaccine in Solid-Organ Transplant Recipients[22]
A weak immune response to two doses of vaccine against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has been observed in recipients of solid-organ transplants. Severe cases of COVID-19 have also been reported in transplant recipients who had received two doses of vaccine. These reports prompted the French National Authority for Health to recommend the use of a third dose in immunosuppressed patients. Here, the authors report the humoral response in a group of 101 consecutive solid-organ transplant recipients (mean age, 58±2 years; 69% were men) who were given three doses of the messenger RNA vaccine BNT162b2 (Pfizer–BioNTech). The group included 78 kidney-transplant recipients, 12 liver-transplant recipients, 8 lung-transplant or heart-transplant recipients, and 3 pancreas-transplant recipients. The first two doses were given 1 month apart, and the third dose was administered 61±1 days after the second dose. The time between transplantation and the initiation of vaccination was 97±8 months. Immunosuppression was due to the use of glucocorticoids (in 87% of patients), calcineurin inhibitors (in 79% of patients), mycophenolic acid (in 63% of patients), mammalian target of rapamycin inhibitors (in 30% of patients), and belatacept (in 12% of patients). The levels of antibodies to SARS-CoV-2 Spike protein were assessed in all the patients with the use of the Wantai enzyme-linked immunosorbent assay (Beijing Wantai Biological Pharmacy Enterprise). Antibody titers are expressed as the ratio of the sample signal to a calibrator-assigned cutoff signal (the signal-to-cutoff ratio).
The prevalence of anti–SARS-CoV-2 antibodies was 0% (95% CI, 0 to 4; 0 of 101 patients) before the first dose, 4% (95% CI, 1 to 10; 4 of 101 patients) before the second dose, 40% (95% CI, 31 to 51; 40 of 99 patients) before the third dose, and 68% (95% CI, 58 to 77; 67 of 99 patients) 4 weeks after the third dose. Among the 59 patients who had been seronegative before the third dose, 26 (44%) were seropositive at 4 weeks after the third dose (mean [±SD] signal-to-cutoff ratio, 690±293). All 40 patients who had been seropositive before the third dose were still seropositive 4 weeks later; their antibody titers increased from 36±12 before the third dose to 2676±350 one month after the third dose (P<0.001). Patients who did not have an antibody response were older, had a higher degree of immunosuppression, and had a lower estimated glomerular filtration rate than patients who had an antibody response. COVID-19 had not developed in any of the patients after they received the three vaccine doses. No serious adverse events were reported after the administration of the third dose, and no acute rejection episodes occurred.
The authors demonstrated that administration of a third dose of the BNT162b2 vaccine to solid-organ transplant recipients significantly improved the immunogenicity of the vaccine, with no cases of COVID-19 reported in any of the patients. However, a large proportion of the patients remain at risk for COVID-19. Barrier measures should be maintained, and vaccination of the relatives of these patients should be encouraged.
| Level 4 |
Studies have reported low seroconversion rates (58% after the second dose) in solid organ transplant recipients who received a messenger RNA (mRNA) SARS-CoV-2 vaccine. Based on this evidence, the French National Authority for Health issued a recommendation in April 2021 to administer a third vaccine dose in immunosuppressed patients who did not respond after two doses. The authors examined the antibody responses of kidney transplant recipients who did not respond to two doses and received a third dose (100 μg) of the Moderna mRNA-1273 COVID-19 vaccine.
Methods: All kidney transplant recipients followed up in the outpatient Kidney Transplantation Department of Strasbourg University Hospital between January 20, 2021, and June 3, 2021, with a negative history for COVID-19 and SARS-CoV-2 anti-Spike IgG levels less than 50 arbitrary units (AU)/mL on the day of the first vaccine injection and one month after the second dose were included. All patients received a third vaccine dose between April 9, 2021, and May 12, 2021.
Anti–receptor-binding domain IgG response after the third vaccine dose was assessed using the ARCHITECT IgG II Quant test (Abbott). According to the manufacturer’s threshold, titers greater than 50 AU/mL were considered positive (detection range, 6.8–80 000 AU/mL; positive agreement, 99.4%; negative agreement, 99.6%). The results of this assay have been shown to correlate with in vitro neutralization of SARS-CoV-2. Mean differences were calculated using general linear models. All calculations were performed using GraphPad Prism version 8.0 (GraphPad) and SPSS version 2020.0.0 (IBM). P < .05 (2-sided) was considered statistically significant.
Results: One month after the second dose, 159 kidney transplant recipients had IgG levels less than 50 AU/mL. The median age was 57.6 years (interquartile range [IQR], 49.6-66.1 years), 61.6% were men, and the median time from transplantation was 5.3 years (IQR, 1.9-11.1 years). 95 patients (59.7%) had no antibody response after two doses (titers <6.8 AU/mL), and 64 patients (40.3%) showed a response below the positivity limit (titers, 6.8-49.9 AU/mL). The third dose was injected a median of 51 days (IQR, 48-59 days) after the second dose. The antibody response was measured a median of 28 days (IQR, 27-33 days) after the third vaccine injection, and 78 patients (49%) had antibody levels greater than 50 AU/mL (median antibody titers of responders, 586 AU/mL; IQR, 197.2-1920.1 AU/mL). Patients who had a weak response after the second dose were more likely to develop an antibody response after the third dose compared with those without an antibody response (81.3% vs. 27.4%, respectively; mean adjusted difference of antibody titers, 894.89 AU/mL [95% CI, 377.41-1410.37]; P = .001). Patients taking tacrolimus, mycophenolate, and steroids were less likely to develop anti–SARS-CoV-2 antibodies than those treated with other regimens (35% vs. 63%, respectively; mean adjusted difference of antibody titers, −697.28 AU/mL [95% CI, −1193.00 to −201.56]; P = .006). No severe adverse events were observed after the third dose.
Discussion: This study found that a third dose of mRNA-1273 vaccine induced a serologic response in 49% of kidney transplant recipients who did not respond after two doses. The findings in this large group of kidney transplant recipients are in accordance with other studies of solid organ transplant recipients. However, 51% of the patients did not develop anti–SARS-CoV-2 antibodies after the third dose, especially those receiving triple immunosuppression. The possibility that patients developed cellular immunity capable of conferring protection against severe disease was not assessed. However, the occurrence of severe COVID-19 in some vaccinated transplant recipients may suggest a lack of immunity.
| Level 4 |
Although the SARS-CoV-2 mRNA vaccines have demonstrated high efficacy, limited data exist on the duration of immune response and its correlation to age and side-effects.
Methods: The authors monitored antibody and memory T cell responses to Spike protein after the two-dose Pfizer-BioNTech BNT162b2 mRNA vaccine for a follow-up period of 3 months among 122 study participants.
Findings: A robust antibody response was observed after the second vaccination dose. However, antibody levels declined at 6 and 12 weeks post-vaccination, indicating a waning of the immune response. Average antibody levels remained higher compared to pre-vaccination or in COVID-19 convalescent individuals. Antibodies efficiently blocked ACE2 receptors binding to the Spike proteins of 4 variants of concern at one week, but decreased at three months, in particular with the B.1.351 and P1 isolates. 87% of individuals developed Spike-specific memory T cell responses which were lower in individuals with increased proportions of immunosenescent CD8+ TEMRA cells. A decreased vaccination efficacy was observed in older individuals, suggesting a detrimental impact of age on outcome.
Interpretation: BNT162b2 induces a strong antibody response to 4 variants of concern at one week post-vaccination, but decreases thereafter, in particular among older individuals. T cell responses, although detectable in the majority, were lower in individuals with immunosenescence. The deterioration of vaccine response needs to be monitored in order to define the optimal timing of re-vaccination.
Figure: S-RBD IgG levels before vaccination, after the single and two-dose immunizations with the Pfizer-BioNTech vaccine, one, 6 and 12 weeks after the second dose, and in COVID-19 convalescent and negative control sera

| Level 4 |
Patients with chronic kidney disease, dialysis patients and kidney-transplant patients are at high risk of developing severe coronavirus disease-19 (COVID-19). Data regarding the immunogenicity of anti-SARS-CoV-2 mRNA vaccines in dialysis patients were published recently. The authors assessed the immunogenicity of anti-SARS-CoV-2 mRNA vaccines in dialysis patients.
Patients and methods: 109 patients on hemodialysis (n = 85) or peritoneal dialysis (n = 24) received two injections of 30-μg doses of the Pfizer-BioNTech BNT162b2 mRNA COVID-19 vaccine administered intramuscularly 28 days apart. Those who were still seronegative after the second dose were given a third dose one month later. Anti-SARS-CoV-2 antibodies were tested before and after vaccination.
Results: Ninety-one out of the 102 patients who had at least a one-month follow-up after the second (n = 97) or the third (n = 5) vaccine doses had anti-SARS-CoV-2 antibodies. The seroconversion rate was 88.7% (86 out of 97 patients) among SARS-CoV-2 seronegative patients at the initiation of vaccination. Receiving immunosuppressive therapy was an independent predictive factor for non-response to vaccination.
Conclusion: Due to high immunogenicity and safety of mRNA vaccines, the authors strongly recommend prioritizing a two-dose vaccination series for dialysis patients. A third dose may be required in non-responders to two doses. When possible, patients waiting for a kidney transplantation should be offered the vaccine before transplantation.
| Level 4 |
Immunocompromised patients such as patients with hematological malignancies have impaired immune response to two doses of the BNT162b2 (Pfizer-BioNtech) vaccine against SARS-CoV-2. Evaluation of a repeated immune stimulation with a third vaccine dose is needed.
METHODS: A vaccine monitoring observatory was conducted in outpatients who were treated for lymphoid malignancies (LM) to monitor both immune and cellular response measured the day of administration of the third dose of the mRNA vaccine BNT162b2 and again three to four weeks later. Elecsys® Anti-SARS-CoV-2 immunoassay was used to asses to the level of SARS-CoV-2 anti-Spike (S) antibodies (Abs) titer and SARS-CoV-2-specific T-cell responses were assessed by a whole blood Interferon-Gamma Release Immuno Assay (IGRA) (QuantiFERON Human IFN-gamma SARS-CoV-2, Qiagen®).
RESULTS: Among the 43 assessable patients (suffering from chronic lymphocytic leukemia (CLL) (n=15), indolent and aggressive B cell non-Hodgkin lymphoma (NHL) (n=14), and multiple myeloma (MM) (n=16)), 18 (41,8%) had no anti-S Abs before the dose 3 of BNT162b2 vaccine (n=9 CLL, n=8 NHL, n=1 MM), and all 18 remained negative after dose 3. Among the 25 patients with positive anti-S titers before dose 3, all patients remained positive and 23 patients increased their anti-S titer after dose 3. Patients with CLL and/or with previous anti-CD20 therapy treated within 12 months of administration of dose 3 had no significant increase of the humoral response. Among 22 available patients, dose 3 of BNT162b2 vaccine significantly increased median IFN-gamma secretion. On eight (36.4%) patients who were double-negative for both immune and cellular response, five (22.7%) remained double-negative after dose 3.
CONCLUSIONS: Dose 3 of BNT162b2 vaccine stimulated humoral immune response among patients with LM, in particular patients with MM who had higher anti-S baseline titer after dose 2, and those with no anti-CD20 treatment history within a year. T-cell response was increased among patients in particular with no active chemotherapy regimen. The authors assert that these data support the use of an early third vaccine dose among immunocompromised patients followed for LM.
| Level 4 |
Patients on maintenance hemodialysis (MHD) are at high risk of infection with SARS-Cov-2 and death due to COVID-19. This vulnerable population has been prioritized for vaccination, but the level of protection achieved in these immunocompromised patients is unclear.
Objectives: To evaluate the protection of MHD patients against COVID-19 after two doses (2D) of BNT162b2, and the safety and impact on immune responses of a third dose (3D).
Design: A prospective observational study.
Setting, Patients, intervention and measurements: The REIN national registry was used to compare the severity of 1474 cases of COVID-19 diagnosed in MHD patients after zero, one or two doses of mRNA vaccine. Anti-Spike receptor binding domain (RBD) IgG and interferon gamma-producing CD4+ and CD8+ specific-T cells were measured after 2D and 3D of BNT162b2 in a monocentric cohort of 75 MHD patients.
Results: Vaccination reduced disease severity but 11% of MHD patients infected after 2D still died. Tolerance to 3D of BNT162b2 was excellent. MHD patients with humoral response similar to healthy volunteers after 2D did not generate more immune effectors after 3D and had more side effects. In contrast, 2/3 of MHD patients with suboptimal response after 2D reached optimal titer of anti-RBD IgG and/or developed Spike-specific CD8+ T cells after 3D. Presence of Spike-specific CD4+ T cells after 2D was associated with response to 3D in multivariate analysis (OR=4.80 [1.23−21.54]; p=0.029).
Limitations: A limited number of patients were injected with 3D.
Conclusion: The standard scheme of vaccination provides insufficient protection to some MHD patients. Anti-RBD IgG and specific CD4+ T cells should be measured after 2D. Among patients with suboptimal humoral response, those with specific CD4+ T cells may benefit from a third dose of vaccine.
| Level 5 |
The antibody response after two doses of an mRNA vaccine against SARS-CoV-2 is excellent in the general population, but the response is different in recipients of solid organ transplants. Markedly attenuated antibody responses in transplant recipients after two doses of an mRNA vaccine against SARS-CoV-2 have been observed. In addition, reports of COVID-19 breakthrough infections in vaccinated transplant recipients have prompted interest in administering an additional vaccine dose.
Objective: To describe antibody responses and vaccine reactions in recipients of solid organ transplants who had a suboptimal response to standard vaccination and subsequently received a third dose of vaccine between 20 March, 2021, and 10 May, 2021.
Thirty patients reported receiving a third dose of vaccine. Their median age was 57 years (interquartile range [IQR], 44 to 62 years), 17 were women, and one identified as non-White. None of the patients reported an illness before vaccination that was consistent with COVID-19 or a positive result on polymerase chain reaction (PCR) assay. In 25 patients, maintenance immunosuppression included tacrolimus or cyclosporine plus mycophenolate. In addition, corticosteroids were used for 24 patients, sirolimus for one, and belatacept for one. The median time between transplantation and initial vaccination was 4.5 years (IQR, 2.3 to 10.5 years). During the initial vaccination, 57% of the 30 patients received 2 doses of the BNT162b2 vaccine (Pfizer/BioNTech), and 43% received 2 doses of the mRNA-1273 vaccine (Moderna).
The authors tested all patients for antibodies against the Spike protein at a median of 9 days (IQR, 2 to 33 days) before they received their third dose of vaccine; 24 patients had negative antibody titers, and 6 patients had low-positive antibody titers. Patients received the third dose of vaccine a median of 67 days (IQR, 54 to 81 days) after the second dose of their initial vaccine series; 15 patients received the Janssen Ad26.COV2.S vaccine, 9 received the Moderna mRNA-1273 vaccine, and 6 received the Pfizer-BioNTech BNT162b2 vaccine.
Antibody testing was repeated a median of 14 days (IQR, 14 to 17 days) after the third dose of vaccine. Of the 6 patients with low-positive antibody titers before the third dose, all had high-positive antibody titers after the third dose. In contrast, of the 24 patients with negative antibody titers before the third dose, only 6 (25%) had high-positive antibody titers after the third dose. Two (8%) had low-positive antibody titers, and 16 (67%) remained negative.
Twenty-three patients completed a questionnaire 7 days after receiving their third dose that asked about specific vaccine reactions. Fifteen patients reported mild or moderate local reactions, and one reported severe arm pain. The most frequent systemic reaction was mild or moderate fatigue in 14 participants; one patient reported severe headache, and one patient reported severe myalgia. No patient reported fever, and no anaphylactoid reactions or neurologic complications were observed. One heart transplant recipient had biopsy-proven, antibody-mediated rejection 7 days after her third dose of vaccine in the setting of acute volume overload. She did not experience an increase in her titer of antibodies against the Spike protein. Heart function remained normal. Immunosuppressive intensification was not initiated. In addition, no patient reported PCR-confirmed COVID-19 during additional follow-up, although the duration of follow-up was limited.
Discussion: The authors state that it is encouraging that antibody titers increased after the third dose in one third of patients who had negative antibody titers and in all patients who had low-positive antibody titers; and that vaccine reactions seem acceptable, given the benefits that these vaccines may confer. Antibody responses, however, appear to vary; and potential risks, such as organ rejection, should be evaluated on an individual basis.
| Level 5 |
Dialysis patients are at increased risk of severe coronavirus disease 2019 (COVID-19) infections. Although these patients are obviously a high priority for vaccination, there are some concerns regarding the efficacy of vaccines. Indeed, dialysis patients are considered to be less prone to respond to vaccines. However, few data exist concerning humoral response to SARS-CoV-2 vaccination with BNT162b2 (Pfizer-BioNTech) in patients on hemodialysis (HD). However, about 90% of HD patients exhibit antibody positivity after two injections of vaccine. Nevertheless, factors associated with poor response are not well described.
The authors studied 50 HD patients who were COVID-19 naive (no clinical history, negative serology) and 15 HD patients with a history of COVID-19 infections. All the patients received two doses of the BNT162b2 mRNA COVID-19 vaccine. Humoral response (SARS-CoV-2 immunoassay, Abbott®) and factors associated with this response were studied. As a relevant threshold cannot be determined, the threshold provided by the manufacturer and a more empirical threshold defined by a value above the first quartile of results (224 UA/mL) were used.
Among naive patients, 45 (90%) had an antibody titre >50 UA/mL and 37 (74%) >224 UA/mL (threshold of the first quartile) one month after the second dose. All non-responder patients were or have been under immunosuppressive drugs (titre <50 UA/mL). Considering a threshold of 224 UA/mL, a present or past history of immunosuppressive drugs was more frequent in non-responder patients (54% vs. 23%; P = 0.007). Non-responder patients had higher C reactive protein (CRP) concentrations (13.6 ± 9.3 vs. 5.7 ± 3.9 mg/L; P = 0.016) and lower lymphocyte count (1046 ± 301 vs. 1363 ± 316/mm2; P = 0.031). There was a close inverse relationship between CRP concentration and antibody level (r = −0.26; P = 0.021). Other clinical and biological parameters were similar in responders and non-responders.
Among previously exposed HD patients, a stronger response to vaccine than that in naive patients was observed [5516 (895–40 000) vs. 1837 (0–7459) UA/mL; P < 0.001).
The authors report in a single-centre study that 90% of dialysis patients have a vaccine response after two doses of BNT162b2 mRNA COVID-19 vaccine; and further observe that immune status markedly affects vaccination response.
The dialysis population is heterogeneous. In this study, 30% of patients received or had received immunosuppressive drugs. Optimal response to vaccination in this group was only 53%, as opposed to 85% in those who did not take immunosuppressive drugs. Of note, a reduced response to BNT162b2 mRNA COVID-19 vaccine has been already reported in kidney transplant patients. Exposure to such medications seems to be an important point to consider in the vaccination strategy.
HD patients exhibit both immune deficiency, which is similar to accelerated immune senescence, and inflammation, which is in part related to chronic innate immune activation. The term ‘inflammaging’ is frequently proposed to include these two aspects. The authors report that inflammaging characterized by low lymphocyte count and elevated CRP levels is associated with a decreased humoral response to the BNT162b2 mRNA COVID-19 vaccine. More accurate determination of the individual immune profile is required to better define vaccination protocol in dialysis patients.
Surprisingly, age was not associated with vaccination response. This may be explained by the low proportion of young patients. However, very old patients seem to have a similar response to patients in the age range 50–70 years.
Patients with a history of COVID-19 infection have an explosive reaction after two doses of BNT162b2 mRNA COVID-19 vaccine. A single injection could be considered in these patients.
Two doses of BNT162b2 mRNA COVID-19 vaccine provide a strong humoral response in three-quarters of dialysis patients. The individual immune status seems to be more important to consider than the status of dialysed persons.
| Level 6 |
Predictive models of immune protection from COVID-19 are urgently needed to identify correlates of protection to assist in the future deployment of vaccines. The authors analyzed the relationship between in vitro neutralization levels and the observed protection from SARS-CoV-2 infection using data from 7 current vaccines and from convalescent cohorts. The neutralization level for 50% protection against detectable SARS-CoV-2 infection was estimated to be 20.2% of the mean convalescent level (95% CI = 14.4%–28.4%). The estimated neutralization level required for 50% protection from severe infection was significantly lower (3% of the mean convalescent level; 95% CI = 0.7%–13%, P = 0.0004). Modelling of the decay of the neutralization titer over the first 250 days after immunization predicted that a significant loss in protection from SARS-CoV-2 infection will occur, although protection from severe disease should be largely retained. Neutralization titers against some SARS-CoV-2 variants of concern were reduced compared with the vaccine strain.
| Level 6 |
Interim results from a phase III trial of the Moderna mRNA-1273 SARS-CoV-2 vaccine indicated 94% efficacy in preventing coronavirus disease 2019 (COVID-19). The durability of protection is currently unknown. The authors describe mRNA1273-elicited binding and neutralizing antibodies in 33 healthy adult participants in an ongoing phase I trial, stratified according to age, at 180 days after the second dose of 100 μg (day 209).
Antibody activity remained high in all age groups at day 209. Binding antibodies, measured by means of an enzyme-linked immunosorbent assay against SARS-CoV-2 Spike receptor–binding domain, had geometric mean end-point titers (GMTs) of 92,451 (95% CI, 57,148 to 149,562) in participants 18 to 55 years of age, 62,424 (95% CI, 36,765 to 105,990) in those 56 to 70 years of age, and 49,373 (95% CI, 25,171 to 96,849) in those 71 years of age or older. Nearly all participants had detectable activity in a pseudovirus neutralization assay, with 50% inhibitory dilution (ID50) GMTs of 80 (95% CI, 40 to 135), 57 (95% CI, 30 to 106), and 59 (95% CI, 29 to 121), respectively. On the more sensitive live-virus focus-reduction neutralization mNeonGreen test, all of the participants had detectable activity, with ID50 GMTs of 406 (95% CI, 286 to 578), 171 (95% CI, 95 to 307), and 131 (95% CI, 69 to 251), respectively. These GMTs were lower in participants 56 to 70 years of age (P=0.02) and in those 71 years of age or older (P=0.004) than in those 18 to 55 years of age.
The estimated half-life of binding antibodies after day 43 for all of the participants was 52 days (95% CI, 46 to 58) calculated with the use of an exponential decay model, which assumes a steady decay rate over time, and 109 days (95% CI, 92 to 136) calculated with the use of a power-law model (at day 119), which assumes that decay rates decrease over time. The neutralizing antibody half-life estimates in the two models were 69 days (95% CI, 61 to 76) and 173 days (95% CI, 144 to 225) for pseudovirus neutralization and 68 days (95% CI, 61 to 75) and 202 days (95% CI, 159 to 272) for live-virus neutralization. These results are consistent with published observations of convalescent patients with COVID-19 through 8 months after symptom onset.
Although the antibody titers and assays that best correlate with vaccine efficacy are not currently known, antibodies that were elicited by mRNA-1273 persisted through 6 months after the second dose, as detected by three distinct serologic assays. Ongoing studies are monitoring immune responses beyond 6 months as well as determining the effect of a booster dose to extend the duration and breadth of activity against emerging viral variants.
| Level 6 |
Turner et al (2021) SARS-CoV-2 mRNA vaccines induce persistent human germinal centre responses[32]
The authors examined antigen-specific B cell responses in peripheral blood (n = 41) and draining lymph nodes in 14 individuals who had received two doses of BNT162b2, an mRNA-based vaccine that encodes the full-length SARS-CoV-2 Spike (S) gene. Circulating IgG- and IgA-secreting plasmablasts that target the S protein peaked one week after the second immunization and then declined, becoming undetectable three weeks later. These plasmablast responses preceded maximal levels of serum anti-S binding and neutralizing antibodies to an early circulating SARS-CoV-2 strain as well as emerging variants, especially in individuals who had previously been infected with SARS-CoV-2 (who produced the most robust serological responses). By examining fine needle aspirates of draining axillary lymph nodes, the authors identified germinal centre B cells that bound S protein in all participants who were sampled after primary immunization. High frequencies of S-binding germinal centre B cells and plasmablasts were sustained in these draining lymph nodes for at least 12 weeks after the booster immunization. S-binding monoclonal antibodies derived from germinal centre B cells predominantly targeted the receptor-binding domain of the S protein, and fewer clones bound to the N-terminal domain or to epitopes shared with the S proteins of the human betacoronaviruses OC43 and HKU1. These latter cross-reactive B cell clones had higher levels of somatic hypermutation as compared to those that recognized only the SARS-CoV-2 S protein, which suggests a memory B cell origin. The authors demonstrate that SARS-CoV-2 mRNA-based vaccination of humans induces a persistent germinal centre B cell response, which enables the generation of robust humoral immunity.
| Level 6 |
Recently, antibody titer levels have been followed in 33 adults who received the Moderna mRNA-1273 vaccine for 6 months. With single dose estimated effectiveness of 92.1%, the authors combine these data with corresponding antibody levels to model and estimate the long-term durability of the vaccine. Additionally, studies about differences in antibody neutralization to SARS-CoV-2 variants are integrated in order to gain insight into how variants can affect the durability of the vaccine.
The estimated days after first injection for binding antibodies to fall below levels of those from day 15 is 411 days. The estimated days after first injection to fall below the lower limit of detection of 20 GMTs is 327 days for pseudovirus neutralization and 461 days for live virus neutralization. The authors’ model has pseudovirus neutralization against variant B.1.351 falling below 20 GMT on day 100; variant P.1 on day 202; variant B.1.429 on day 258; and variant B.1.1.7 on day 309.
Data used contain many limitations including a small sample size with older age bias, sensitivity of the neutralization assays, and limited data on variants. Nonetheless, the authors assert that the mRNA-1273 two-dose vaccine can provide over a year of protection against COVID-19 from the initial D614G variant. It is likely by the second year, protection against COVID-19 will fall below single dose efficacy. Therefore, consideration should be given to a booster shot a year after the first set of vaccines. If there is an observed increase in variants with higher resistance such as B.1.351 and P.1, a booster vaccine against the newer variants should be considered to increase protection against resistant variants.
| Level 6 |
A higher risk of death from COVID- 19 has been shown for patients with solid cancers or haematological malignancies (HM). Patients with cancer were quickly prioritised in early 2021 for vaccination, although dependent on very unequal availability at a global level. Impaired immunogenicity of SARS-CoV-2 mRNA vaccines in immunocompromised patients was rapidly reported as early as April 2021; and the humoral response of the SARS-CoV-2 vaccination is considered insufficient in patients followed for HM, particularly when these patients are on anti-CD20 treatment. Thus, improving vaccination coverage by strengthening immune stimulation should be evaluated in patients under active treatment against cancer. The authors discuss three different approaches: a third dose of early vaccine (repeated immune stimulation), heterologous prime-boost vaccination (multimodal immune stimulation) and a double-dose strategy (maximisation of immune response).
| Level 7 |
The COVID-19 pandemic poses unique challenges regarding the optimal care of patients with rheumatic diseases who may have an increased risk of infection and hospitalisation. It is therefore highly important to ensure successful vaccination of these patients. The messenger RNA vaccine BNT162b2 (Comirnaty, Pfizer-BioNTech) against SARS-CoV-2 strongly reduces infection, transmission, hospitalization and death in immunocompetent patients. The development of neutralising antibodies after vaccination has been associated with protection from COVID-19. However, a decreased immunogenicity of several vaccines has been described under immunosuppressive medication, and first reports seem to confirm reduced antibody responses after vaccinations against SARS-CoV-2 in patients on some immunosuppressive medications. This led rheumatologists to address the question of how to deal with patients who show insufficient immunogenicity after vaccination.
The authors describe a case with an initially negative antibody response and seroconversion after repeated booster vaccinations without interruption of immunosuppressive medication. The patient is a 54-year-old man, with a body mass index of 30.7 kg/m². He suffers from seropositive rheumatoid arthritis (RA, since 2013), polycythemia vera and had a leucocytoclastic vasculitis in 2020, confirmed by skin biopsy, which was successfully treated with an initial dose of 100 mg prednisolone. The prednisolone dose was then decreased to 5 mg/day and eventually stopped 5 days before the first vaccination. Leucocytoclastic vasculitis and polycythemia vera were in remission throughout the vaccination periods. The RA had been highly active in 2020, but remained with low disease activity (Disease Activity Score 28-C reactive protein ≤3.2) since January 2021 and throughout the vaccinations under treatment with upadacitinib 15 mg/day and methotrexate 10 mg/week, both since January 2021. Both medications were not paused for the vaccinations because the risk of recurrence of disease activity was considered high, and methotrexate was even increased to 12.5 mg/week between the second and third vaccination. Previous medications included anti-tumour necrosis factor-α antibodies, but not rituximab.
After the first vaccination, the patient suffered from fever, nausea, weakness, tiredness and headache for 5 days. After the second vaccination, he described tiredness for 2 days. Antibody titres against SARS-CoV-2 Spike protein did not show a titre increase from earlier testing in May 2020 to 14 days after the first two vaccinations with BNT162b2. The patient then received an additional cycle of two vaccinations with the same vaccine in a standard dose outside of care, which led to IgA and IgG seroconversion and development of neutralising antibodies until 15 days after the fourth vaccination. The patient reported only mild tiredness for one day after the third and fourth vaccination.
It is possible that a delayed antibody response to the first two vaccinations or the longer interval between the first and fourth vaccination may have contributed to the response ; and that a significant T-cell response already existed after the first two vaccinations, given the clinical reactogenicity. However, after hepatitis B virus vaccinations, testing for antibodies and booster injections have been advised for immunocompromised patients with low titres of protective antibodies independent of T-cell responses. Currently, American College of Rheumatology guidance does not recommend routine measurement of antibody titres after SARS-CoV-2 vaccination, and it remains unclear how to best interpret the results. The German Rheumatology Association acknowledged in a recent statement that booster vaccinations may have to be considered in patients who do not show sufficiently high or long-lasting titres of neutralising antibodies, but this remains subject to an ongoing debate. The present case demonstrates that booster vaccinations in patients with an initially negative antibody response may induce a positive antibody response even without pausing immunosuppression.
Other Sources of Evidence
The World Health Organization called for a moratorium on booster doses until the end of September 2021 to address global disparities in vaccination rates. The pause would help free up vaccine supplies so that all countries could vaccinate at least 10% of their populations.
Out of about 600,000 individuals vaccinated with the third vaccine dose in Israel, fewer than 50 cases of side effects around the time of vaccination have been reported so far. Side effects reported were mild and passed rapidly: local pain in the injection site; fever; nausea.
References
[1] Conseil d’Orientation de la Stratégie Vaccinale (6 April 2021) Elargissement des priorités d’accès à la vaccination anti-COVID-19. https://solidarites-sante.gouv.fr/grands-dossiers/vaccin-COVID-19/COVID-19-conseil-d-orientation-de-la-strategie-vaccinale/article/les-avis-du-conseil-d-orientation-de-la-strategie-vaccinale. Accessed 27/07/21.
[2] Conseil Scientifique COVID-19 (2021) Reagir maintenant pour limiter une nouvelle vague associee au variant delta. https://solidarites-sante.gouv.fr/IMG/pdf/avis_conseil_scientifique_6_juillet_2021_actualise_8_juillet_2021.pdf . Accessed 27/07/21.
[3] European Medicines Agency; European Centre for Disease Prevention and Control (2021) EMA and ECDC update on COVID-19. https:www.ecdc.europa.eu/en/news-events/ema-and-ecdc-update-COVID-19. Accessed 27/07/21.
[4] Department of Health and Social Care (2021) JCVI interim advice: potential COVID-19 booster vaccine programme winter 2021 to 2022. https://www.gov.uk/government/publications/jcvi-interim-advice-on-a-potential-coronavirus-COVID-19-booster-vaccine-programme-for-winter-2021-to-2022/jcvi-interim-advice-potential-COVID-19-booster-vaccine-programme-winter-2021-to-2022. Accessed 28/07/21. See also https://www.gov.uk/government/news/jcvi-issues-advice-on-third-dose-vaccination-for-severely-immunosuppressed. Accessed 09/09/2021.
[5] UpToDate (2021) COVID-19: Vaccines to prevent SARS-CoV-2 infection. https://www.uptodate.com/contents/covid-19-vaccines-to-prevent-sars-cov-2-infection. Accessed 10/08/21.
[6] Six Month Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine Stephen J. Thomas et al. medRxiv 2021.07.28.21261159; doi: https://doi.org/10.1101/2021.07.28.21261159.
[7] Anand S, Montez-Rath ME, Han J, Garcia P, Cadden L, Hunsader P, Kerschmann R, Beyer P, Dittrich M, Block GA, Boyd SD, Parsonnet J, Chertow GM. Antibody Response to COVID-19 vaccination in Patients Receiving Dialysis. medRxiv [Preprint]. 2021 May 12:2021.05.06.21256768. doi: 10.1101/2021.05.06.21256768. Update in: J Am Soc Nephrol. 2021 Jun 11;: PMID: 34013281; PMCID: PMC8132255.
[8] Nace DA, Kip KE, Mellors JW, Peck Palmer OM, Shurin MR, Mulvey K, Crandall M, Sobolewski MD, Enick PN, McCormick KD, Jacobs JL, Kane AL, Lukanski A, Kip PL, Wells A. Antibody Responses After mRNA-Based COVID-19 Vaccination in Residential Older Adults: Implications for Reopening. J Am Med Dir Assoc. 2021 Aug;22(8):1593-1598. doi: 10.1016/j.jamda.2021.06.006. Epub 2021 Jun 12. PMID: 34129831; PMCID: PMC8196346.
[9] Shrotri M, Navaratnam AMD, Nguyen V, Byrne T, Geismar C, Fragaszy E, Beale S, Fong WLE, Patel P, Kovar J, Hayward AC, Aldridge RW; Virus Watch Collaborative. Spike-antibody waning after second dose of BNT162b2 or ChAdOx1. Lancet. 2021 Jul 31;398(10298):385-387. doi: 10.1016/S0140-6736(21)01642-1. Epub 2021 Jul 17. PMID: 34274038; PMCID: PMC8285117.
[10] Flaxman, Amy and Marchevsky, Natalie and Jenkin, Daniel and Aboagye, Jeremy and Aley, Parvinder K. and Angus, Brian John and Belij-Rammerstorfer, Sandra and Bibi, Sagida and Bittaye, Mustapha and Cappuccini, Federica and Cicconi, Paola and Clutterbuck, Elizabeth and Davies, Sophie and Dejnirattisai, Wanwisa and Dold, Christina and Ewer, Katie and Folegatti, Pedro M. and Fowler, Jamie and Hill, Adrian V. S. and Kerridge, Simon and Minassian, Angela M. and Mongkolspaya, Juthathip and Farooq Mujadidi, Yama and Plested, Emma and Ramasamy, Maheshi N. and Robinson, Hannah and Sanders, Helen and Sheehan, Emma and Smith, Holly and Snape, Matthew D. and Song, Rinn and Woods, Danielle and Screaton, Gavin R. and Gilbert, Sarah C. and Voysey, Merryn and Pollard, Andrew and Lambe, Teresa and Group, The Oxford COVID Vaccine, Tolerability and Immunogenicity After a Late Second Dose or a Third Dose of ChAdOx1 nCoV-19 (AZD1222). Available at SSRN: https://ssrn.com/abstract=3873839 or http://dx.doi.org/10.2139/ssrn.3873839.
[11] Preliminary Analysis of Safety and Immunogenicity of a SARS-CoV-2 Variant Vaccine Booster Kai Wu, Angela Choi, Matthew Koch, LingZhi Ma, Anna Hill, Naveen Nunna, Wenmei Huang, Judy Oestreicher, Tonya Colpitts, Hamilton Bennett,
Holly Legault, Yamuna Paila, Biliana Nestorova, Baoyu Ding, Rolando Pajon, Jacqueline M Miller, Brett Leav, Andrea Carfi, Roderick McPhee, Darin K Edwards medRxiv 2021.05.05.21256716; doi: https://doi.org/10.1101/2021.05.05.21256716
[12] Stumpf J, Siepmann T, Lindner T, Karger C, Schwöbel J, Anders L, Faulhaber-Walter R, Schewe J, Martin H, Schirutschke H, Barnett K, Hüther J, Müller P, Langer T, Pluntke T, Anding-Rost K, Meistring F, Stehr T, Pietzonka A, Escher K, Cerny S, Rothe H, Pistrosch F, Seidel H, Paliege A, Beige J, Bast I, Steglich A, Gembardt F, Kessel F, Kröger H, Arndt P, Sradnick J, Frank K, Klimova A, Mauer R, Grählert X, Anft M, Blazquez-Navarro A, Westhoff TH, Stervbo U, Tonn T, Babel N, Hugo C. Humoral and cellular immunity to SARS-CoV-2 vaccination in renal transplant versus dialysis patients: A prospective, multicenter observational study using mRNA-1273 or BNT162b2 mRNA vaccine. Lancet Reg Health Eur. 2021 Jul 23:100178. doi: 10.1016/j.lanepe.2021.100178. Epub ahead of print. PMID: 34318288; PMCID: PMC8299287.
[13] Rabinowich L, Grupper A, Baruch R, Ben-Yehoyada M, Halperin T, Turner D, Katchman E, Levi S, Houri I, Lubezky N, Shibolet O, Katchman H. Low immunogenicity to SARS-CoV-2 vaccination among liver transplant recipients. J Hepatol. 2021 Aug;75(2):435-438. doi: 10.1016/j.jhep.2021.04.020. Epub 2021 Apr 21. PMID: 33892006; PMCID: PMC8058047.
[14] Schramm R, Costard-Jäckle A, Rivinius R, Fischer B, Müller B, Boeken U, Haneya A, Provaznik Z, Knabbe C, Gummert J. Poor humoral and T-cell response to two-dose SARS-CoV-2 messenger RNA vaccine BNT162b2 in cardiothoracic transplant recipients. Clin Res Cardiol. 2021 Aug;110(8):1142-1149. doi: 10.1007/s00392-021-01880-5. Epub 2021 Jul 9. PMID: 34241676; PMCID: PMC8267767.
[15] Immunogenicity of COVID-19 Vaccination in Immunocompromised Patients: An Observational, Prospective Cohort Study Interim Analysis Ghady Haidar, Mounzer Agha, Amy Lukanski, Kelsey Linstrum, Rachel Troyan, Andrew Bilderback, Scott Rothenberger, Deborah K. McMahon, Melissa Crandall, P. Nathan Enick, Michelle Sobolewksi, Kevin Collins, Marc B. Schwartz, Jeffrey M. Dueker, Fernanda P. Silveira, Mary E. Keebler, Abhinav Humar, James D. Luketich, Matthew R. Morrell, Joseph M. Pilewski, John F. McDyer, Bhanu Pappu, Robert L. Ferris, Stanley M. Marks, Cynthia Klamar-Blain, Urvi M. Parikh, Amy Heaps, Paula L. Kip, Alan Wells, Tami Minnier, Derek Angus, John W. Mellors medRxiv 2021.06.28.21259576; doi: https://doi.org/10.1101/2021.06.28.21259576
[16] Tenforde MW, [et al] Effectiveness of SARS-CoV-2 mRNA Vaccines for Preventing COVID-19 Hospitalizations in the United States. medRxiv [Preprint]. 2021 Jul 8:2021.07.08.21259776. doi: 10.1101/2021.07.08.21259776. PMID: 34268515; PMCID: PMC8282104.
[17] Shroff RT, Chalasani P, Wei R, Pennington D, Quirk G, Schoenle MV, Uhrlaub JL, Ripperger TJ, Jergović M, Dalgai S, Wolf A, Hammad H, Carrier A, Scott AJ, Nikolich-Žugich J, Worobey M, Sprissler R, Dake M, LaFleur BJ, Bhattacharya D. Immune Responses to COVID-19 mRNA Vaccines in Patients with Solid Tumors on Active, Immunosuppressive Cancer Therapy. medRxiv [Preprint]. 2021 May 14:2021.05.13.21257129. doi: 10.1101/2021.05.13.21257129. PMID: 34013289; PMCID: PMC8132263.
[18] Jahn M, Korth J, Dorsch O, Anastasiou OE, Sorge-Hädicke B, Tyczynski B, Gäckler A, Witzke O, Dittmer U, Dolff S, Wilde B, Kribben A. Humoral Response to SARS-CoV-2-Vaccination with BNT162b2 (Pfizer-BioNTech) in Patients on Hemodialysis. Vaccines (Basel). 2021 Apr 8;9(4):360. doi: 10.3390/vaccines9040360. PMID: 33918085; PMCID: PMC8070660.
[19] Müller L, Andrée M, Moskorz W, Drexler I, Walotka L, Grothmann R, Ptok J, Hillebrandt J, Ritchie A, Rabl D, Ostermann PN, Robitzsch R, Hauka S, Walker A, Menne C, Grutza R, Timm J, Adams O, Schaal H. Age-dependent immune response to the Biontech/Pfizer BNT162b2 COVID-19 vaccination. Clin Infect Dis. 2021 Apr 27:ciab381. doi: 10.1093/cid/ciab381. Epub ahead of print. PMID: 33906236; PMCID: PMC8135422.
[20] Poor antibody response to BioNTech/Pfizer COVID-19 vaccination in SARS-CoV-2 naïve residents of nursing homes Pieter Pannus, Kristof Y Neven, Stéphane De Craeye, Leo Heyndrickx, Sara Vande Kerckhove, Daphnée Georges, Johan Michiels, Antoine Francotte, Marc Van Den Bulcke, Maan Zrein, Steven Van Gucht, Marie-Noëlle Schmickler, Mathieu Verbrugghe, André Matagne, Isabelle Thomas, Katelijne Dierick, Joshua A. Weiner, Margaret E. Ackerman, Stanislas Goriely, Maria E Goossens, Kevin K. Ariën, Isabelle Desombere, Arnaud Marchant medRxiv 2021.06.08.21258366; doi: https://doi.org/10.1101/2021.06.08.21258366
[21] Robust antibody levels in both diabetic and non-diabetic individuals after BNT162b2 mRNA COVID-19 vaccination Hamad Ali, Abdelmohsen Al-Terki, Sardar Sindhu, Barrak Alahmad, Maha Hammad, Salman Al-Sabah, Mohammad Alghounaim, Mohammad H. Jamal, Ali Aldei, Mohammad J. Mairza, Maitham Husain, Sriraman Deverajan, Rasheed Ahmad, Preethi Cherian, Irina Alkhairi, Abdullah Alkandari, Jehad Abubaker, Mohamed Abu-Farha, Fahd Al-Mulla medRxiv 2021.07.23.21261042; doi: https://doi.org/10.1101/2021.07.23.21261042
[22] Kamar N, Abravanel F, Marion O, Couat C, Izopet J, Del Bello A. Three Doses of an mRNA Covid-19 Vaccine in Solid-Organ Transplant Recipients. N Engl J Med. 2021 Aug 12;385(7):661-662. doi: 10.1056/NEJMc2108861. Epub 2021 Jun 23. PMID: 34161700; PMCID: PMC8262620.
[23] Benotmane I, Gautier G, Perrin P, Olagne J, Cognard N, Fafi-Kremer S, Caillard S. Antibody Response After a Third Dose of the mRNA-1273 SARS-CoV-2 Vaccine in Kidney Transplant Recipients With Minimal Serologic Response to 2 Doses. JAMA. 2021 Jul 23. doi: 10.1001/jama.2021.12339. Epub ahead of print. PMID: 34297036.
[24] Declined antibody responses to COVID-19 mRNA vaccine within first three months Paul Naaber, Liina Tserel, Kadri Kangro, Epp Sepp, Virge Jürjenson, Ainika Adamson, Liis Haljasmägi, Pauliina Rumm, Regina Maruste, Jaanika Kärner, Joachim M. Gerhold, Anu Planken, Mart Ustav, Kai Kisand, Pärt Peterson. medRxiv 2021.04.19.21255714; doi: https://doi.org/10.1101/2021.04.19.21255714
[25] Longlune N, Nogier MB, Miedougé M, Gabilan C, Cartou C, Seigneuric B, Del Bello A, Marion O, Faguer S, Izopet J, Kamar N. High immunogenicity of a messenger RNA based vaccine against SARS-CoV-2 in chronic dialysis patients. Nephrol Dial Transplant. 2021 May 31:gfab193. doi: 10.1093/ndt/gfab193. Epub ahead of print. PMID: 34057463; PMCID: PMC8195197.
[26] Humoral and cellular responses after a third dose of BNT162b2 vaccine in patients treated for lymphoid malignancies Daniel Re, Barbara Seitz-Polski, Michel Carles, Vesna Brglez, Daisy Graça, Sylvia Benzaken, Stéphane Liguori, Khaled Zahreddine, Margaux Delforge, Benjamin Verrière, Emmanuel Chamorey, Barrière Jérôme medRxiv 2021.07.18.21260669; doi: https://doi.org/10.1101/2021.07.18.21260669
[27] Justification, safety, and efficacy of a third dose of mRNA vaccine in maintenance hemodialysis patients: a prospective observational study Maxime Espi, Xavier Charmetant, Thomas Barba, Caroline Pelletier, Laetitia Koppe, Elodie Chalencon, Emilie Kalbacher, Virginie Mathias, Anne Ovize, Emmanuelle Cart-Tanneur, Christine Bouz, Laurence Pellegrina, Emmanuel Morelon, Laurent Juillard, Denis Fouque, Cécile Couchoud, Olivier Thaunat medRxiv 2021.07.02.21259913; doi: https://doi.org/10.1101/2021.07.02.21259913
[28] Werbel WA, Boyarsky BJ, Ou MT, Massie AB, Tobian AAR, Garonzik-Wang JM, Segev DL. Safety and Immunogenicity of a Third Dose of SARS-CoV-2 Vaccine in Solid Organ Transplant Recipients: A Case Series. Ann Intern Med. 2021 Jun 15:L21-0282. doi: 10.7326/L21-0282. Epub ahead of print. PMID: 34125572; PMCID: PMC8252023.
[29] Ducloux D, Colladant M, Chabannes M, Yannaraki M, Courivaud C. Humoral response after 3 doses of the BNT162b2 mRNA COVID-19 vaccine in patients on hemodialysis. Kidney Int. 2021 Sep;100(3):702-704. doi: 10.1016/j.kint.2021.06.025. Epub 2021 Jun 30. PMID: 34216675; PMCID: PMC8243640.
[30] Khoury, D.S., Cromer, D., Reynaldi, A. et al. Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-CoV-2 infection. Nat Med 27, 1205–1211 (2021). https://doi.org/10.1038/s41591-021-01377-8
[31] Doria-Rose N, Suthar MS, Makowski M, O’Connell S, McDermott AB, Flach B, Ledgerwood JE, Mascola JR, Graham BS, Lin BC, O’Dell S, Schmidt SD, Widge AT, Edara VV, Anderson EJ, Lai L, Floyd K, Rouphael NG, Zarnitsyna V, Roberts PC, Makhene M, Buchanan W, Luke CJ, Beigel JH, Jackson LA, Neuzil KM, Bennett H, Leav B, Albert J, Kunwar P; mRNA-1273 Study Group. Antibody Persistence through 6 Months after the Second Dose of mRNA-1273 Vaccine for Covid-19. N Engl J Med. 2021 Jun 10;384(23):2259-2261. doi: 10.1056/NEJMc2103916. Epub 2021 Apr 6. PMID: 33822494.
[32] Turner JS, O’Halloran JA, Kalaidina E, Kim W, Schmitz AJ, Zhou JQ, Lei T, Thapa M, Chen RE, Case JB, Amanat F, Rauseo AM, Haile A, Xie X, Klebert MK, Suessen T, Middleton WD, Shi PY, Krammer F, Teefey SA, Diamond MS, Presti RM, Ellebedy AH. SARS-CoV-2 mRNA vaccines induce persistent human germinal centre responses. Nature. 2021 Aug;596(7870):109-113. doi: 10.1038/s41586-021-03738-2. Epub 2021 Jun 28. PMID: 34182569.
[33] Modeling and Predicting Antibody Durability for mRNA-1273 Vaccine for SARS-CoV-2 Variants George Luo, Zhongbo Hu, John J. Letterio medRxiv 2021.05.04.21256537; doi: https://doi.org/10.1101/2021.05.04.21256537
[34] Barrière J, Re D, Peyrade F, Carles M. Current perspectives for SARS-CoV-2 vaccination efficacy improvement in patients with active treatment against cancer. Eur J Cancer. 2021 Sep;154:66-72. doi: 10.1016/j.ejca.2021.06.008. Epub 2021 Jun 18. PMID: 34243079; PMCID: PMC8260097.
[35] Albach FN, Burmester GR, Biesen R. Successful BNT162b2 booster vaccinations in a patient with rheumatoid arthritis and initially negative antibody response. Ann Rheum Dis. 2021 Jun 24:annrheumdis-2021-220834. doi: 10.1136/annrheumdis-2021-220834. Epub ahead of print. PMID: 34167947.
[36] World Health Organization (2021) https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-COVID-4-august-2021. Accessed 27/07/21.
[37] Ministry for Health, Israel (2021) https://www.gov.il/en/departments/news/09082021-02 . Accessed 27/07/21
Produced by the members of the National Health Library and Knowledge Service Evidence Team†. Current as t 10 August 2021. This evidence summary collates the best available evidence at the time of writing and does not replace clinical judgement or guidance. Emerging literature or subsequent developments in respect of COVID-19 may require amendment to the information or sources listed in the document. Although all reasonable care has been taken in the compilation of content, the National Health Library and Knowledge Service Evidence Team makes no representations or warranties expressed or implied as to the accuracy or suitability of the information or sources listed in the document. This evidence summary is the property of the National Health Library and Knowledge Service and subsequent re-use or distribution in whole or in part should include acknowledgement of the service.
Gethin White, Librarian, Dr. Steevens’ Hospital [Author]; Siobhan McCarthy, Information Specialist, Health Intelligence Unit, Strategic Planning and Transformation [Author, Editor]; Brendan Leen, Area Library Manager, HSE South [Author, Editor]; NIAC Subgroup Contributors: Dr. Peter O’Reilly; Dr. Geraldine Casey; Philippa White; Dr. Grace Kenny.

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.